Most people understand that high cholesterol raises the risk of a heart attack. Far fewer know that cholesterol and stroke risk are connected by the same underlying mechanism — and that the evidence for cholesterol lowering as a stroke prevention strategy is nearly as compelling as the evidence for heart attack prevention.
Stroke kills or disables more people annually than any other single neurological event, and the majority of strokes — approximately 87 percent — are ischemic strokes caused by blood clots blocking cerebral arteries. These are the strokes most directly connected to cholesterol. The link runs primarily through the carotid arteries: elevated LDL drives atherosclerotic plaque in the carotid artery walls, and plaque in the carotids is the most common source of the emboli that block cerebral vessels and cause ischemic stroke.
Understanding cholesterol and stroke risk means understanding ischemic stroke specifically: what causes it, which cholesterol fractions matter most, what the clinical trial evidence shows about LDL lowering as prevention, and what practical steps most effectively reduce risk.
How Cholesterol Contributes to Stroke Risk
A stroke occurs when blood flow to part of the brain is interrupted, causing neuronal death within minutes. The mechanism depends on the type of stroke.
Ischemic stroke — which accounts for approximately 87 percent of all strokes — results from arterial occlusion. The occlusion can happen in two ways: a thrombus (clot) forms directly at the site of an atherosclerotic plaque in a cerebral or carotid artery (thrombotic stroke), or a fragment of plaque or clot breaks off from an upstream location — most commonly the carotid artery bifurcation in the neck — and travels into smaller cerebral arteries where it lodges and blocks flow (embolic stroke). In both mechanisms, atherosclerotic plaque is the critical substrate. Elevated LDL drives the formation and growth of that plaque in the carotid arteries exactly as it does in the coronary arteries. Large artery atherosclerosis — primarily of the carotid and vertebral arteries — accounts for approximately 25 percent of ischemic strokes.
A second pathway connects dyslipidemia to stroke through atrial fibrillation (AF). Metabolic syndrome — characterized by elevated triglycerides, low HDL, abdominal obesity, hypertension, and insulin resistance — increases the risk of developing atrial fibrillation. AF is the most common cardiac source of cardioembolic stroke, accounting for approximately 25 percent of ischemic strokes. People with the dyslipidemia of metabolic syndrome are therefore at elevated stroke risk through two distinct pathways: direct carotid atherosclerosis and AF-mediated cardioembolic stroke.
Hemorrhagic stroke — the remaining 13 percent — is caused by rupture of a blood vessel, not by arterial occlusion. Its primary risk factor is high blood pressure, not elevated LDL. The relationship between cholesterol and hemorrhagic stroke is addressed in detail later in this article.
Cholesterol and Stroke Risk — Which Numbers Matter Most
LDL cholesterol (LDL-C) is the primary atherogenic driver of carotid plaque and the primary lipid target for ischemic stroke prevention. Higher LDL accelerates plaque accumulation in the carotid arteries; lower LDL slows it. The dose-response relationship between LDL and ischemic stroke risk is consistent across large clinical trial meta-analyses.
HDL cholesterol (HDL-C) — low HDL (below 40 mg/dL in men, below 50 mg/dL in women) — is associated with increased ischemic stroke risk in observational studies. The proposed mechanisms include impaired reverse cholesterol transport and direct endothelial protective effects. However, as with coronary heart disease, pharmacologically raising HDL has not reduced stroke rates in clinical trials. Low HDL is a risk marker reflecting metabolic risk, not a direct therapeutic target in isolation. For more on what each cholesterol fraction means, see LDL vs HDL cholesterol.
Triglycerides are associated with increased ischemic stroke risk through several mechanisms. Elevated triglycerides promote the formation of small, dense LDL particles (more atherogenic than large buoyant LDL); they lower HDL; and very high triglycerides are associated with increased risk of atrial fibrillation — which is a major independent stroke risk factor. Non-fasting triglyceride measurements may actually be more predictive of stroke risk than fasting values, because they capture postprandial triglyceride-rich lipoproteins that are atherogenic in their own right.
Lipoprotein(a) — Lp(a) is an independent risk factor for ischemic stroke not captured by the standard lipid panel. Lp(a) promotes atherosclerosis in the carotid and cerebral arteries and inhibits fibrinolysis — making existing clots harder to break down. This combination of pro-atherogenic and pro-thrombotic properties makes elevated Lp(a) particularly dangerous in the cerebrovascular context, and explains a meaningful proportion of ischemic strokes in patients with apparently acceptable LDL-C.
ApoB and non-HDL-C provide more accurate assessments of total atherogenic particle burden than LDL-C alone — particularly in patients with elevated triglycerides, where LDL-C may underestimate the true number of atherogenic particles in circulation.
What the Evidence Shows About LDL Lowering and Stroke Prevention
The clinical trial evidence for LDL lowering as a stroke prevention strategy is substantial, spanning primary prevention, secondary prevention, and large meta-analyses.
The Cholesterol Treatment Trialists’ (CTT) Collaboration — the definitive meta-analysis including over 174,000 patients across 27 major statin trials — found that each 1 mmol/L (approximately 39 mg/dL) reduction in LDL-C is associated with approximately a 17 percent relative reduction in ischemic stroke. This is slightly less than the 22 percent reduction in major coronary events from the same degree of LDL lowering, but it is clinically highly significant and consistent across patient subgroups.
The SPARCL trial (2006) was the landmark study specifically focused on stroke secondary prevention. It randomized 4,731 patients who had had a stroke or TIA within the prior 6 months to atorvastatin 80 mg versus placebo. Over five years, atorvastatin reduced the risk of recurrent stroke by 16 percent relative to placebo — establishing the principle that patients with ischemic stroke or TIA from large artery atherosclerosis should receive high-intensity statin therapy even if they have no known coronary artery disease.
PCSK9 inhibitor data extend the LDL lowering benefit to very low LDL targets. The FOURIER trial demonstrated a 25 percent relative reduction in stroke with evolocumab compared to statin alone, with LDL reduced to a median of approximately 30 mg/dL — confirming that reducing LDL well below 70 mg/dL produces further stroke risk reduction.
The LDL–Hemorrhagic Stroke Question
One genuinely complex nuance in cholesterol and stroke risk is the relationship between low LDL and hemorrhagic stroke. This issue comes up frequently and deserves careful clarification.
Several observational studies — particularly from Asian populations with higher baseline hemorrhagic stroke rates — noted an inverse association between cholesterol levels and hemorrhagic stroke. The proposed mechanism: cholesterol may help maintain the structural integrity of small cerebral vessel walls, and very low cholesterol could impair this function under hypertensive stress.
The SPARCL trial found that atorvastatin 80 mg, while reducing ischemic stroke by 22 percent, was associated with more hemorrhagic strokes than placebo (55 versus 33 events). The absolute risk difference was small — approximately 0.4 percent over five years — and was largely confined to patients with a history of prior hemorrhagic stroke at baseline.
Subsequent larger analyses substantially reassured: the CTT meta-analysis found no statistically significant association between statin therapy and hemorrhagic stroke overall. PCSK9 inhibitor trials achieving median LDL levels around 30 mg/dL showed no significant increase in hemorrhagic stroke. The current consensus is that the substantial benefit of LDL lowering on ischemic stroke — which is far more common — significantly outweighs the marginal hemorrhagic signal seen in specific subgroups. Patients with a prior hemorrhagic stroke represent a distinct risk profile requiring individual assessment.
Cholesterol and Carotid Artery Disease — The Direct Link
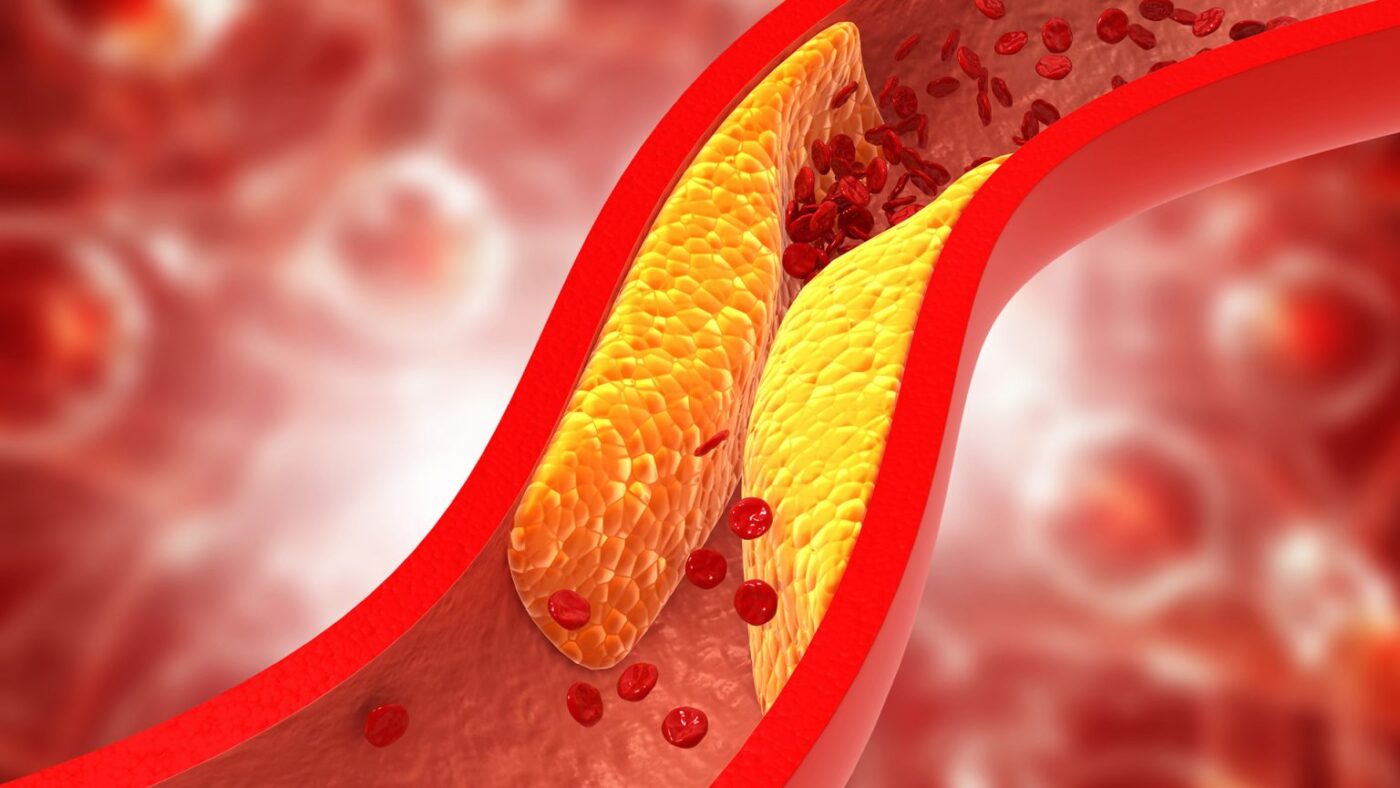
The carotid arteries — the two large arteries running up either side of the neck to supply the brain — are the most clinically important site of cholesterol-driven vascular disease in the context of stroke risk. Atherosclerotic plaque develops at the carotid bifurcation by the same mechanism as in the coronary arteries: LDL oxidation, foam cell formation, fibrous plaque development with a necrotic lipid core.
Carotid plaque creates stroke risk through two mechanisms. First, a plaque can rupture or erode, triggering thrombus formation at the carotid. Fragments are carried into smaller intracranial arteries, where they lodge and cause ischemic stroke. Second, very large plaques cause high-grade stenosis, severely limiting cerebral blood flow.
Carotid plaque is detectable by carotid ultrasound (measures intima-media thickness and visualizes plaque directly), CT angiography (detailed anatomy, identifies calcified versus soft/vulnerable plaque), MRI angiography (cerebral vasculature), and conventional catheter angiography (gold standard for stenosis quantification). For carotid stenosis management: medical therapy — high-intensity statin plus antiplatelet medication — is the mainstay for patients with moderate asymptomatic stenosis. Carotid endarterectomy or carotid artery stenting is recommended for symptomatic high-grade stenosis (above 50–70 percent depending on procedure and guidelines). In all cases, aggressive LDL lowering to below 70 mg/dL slows further plaque progression and stabilizes existing plaque. For more on the plaque formation process, see cholesterol and plaque buildup in arteries.
How to Reduce Cholesterol-Related Stroke Risk
Lipid-lowering therapy. High-intensity statin therapy is the cornerstone of both primary and secondary stroke prevention in patients with high LDL or established large artery atherosclerosis. For secondary prevention after ischemic stroke or TIA from large artery atherosclerosis, AHA/ASA guidelines recommend a target LDL below 70 mg/dL with high-intensity statin; ezetimibe should be added if the target is not reached. For very high-risk patients with recurrent ischemic stroke despite statin plus ezetimibe, a PCSK9 inhibitor is appropriate. For more on what triggers elevated LDL in the first place, see causes of high cholesterol.
Blood pressure control is the single most important modifiable risk factor for stroke overall. LDL and blood pressure work synergistically on the endothelium — hypertension promotes endothelial injury that accelerates LDL infiltration into arterial walls. Controlling blood pressure to below 130/80 mmHg dramatically reduces both ischemic and hemorrhagic stroke risk.
Smoking cessation is essential for stroke prevention. Smoking directly promotes carotid atherosclerosis, increases LDL oxidation, and raises blood thrombogenicity. The excess stroke risk attributable to smoking diminishes substantially within years of cessation.
A Mediterranean-style dietary pattern reduces both LDL and systemic inflammation, improves endothelial function, and has been shown in clinical trials to reduce cardiovascular events including stroke.
Detection and treatment of atrial fibrillation addresses the cardioembolic stroke pathway. People with AF require oral anticoagulation — not just antiplatelet therapy — to prevent cardioembolic stroke. AF screening is particularly important in people with metabolic syndrome and dyslipidemia, who are at elevated AF risk through the mechanisms described above.
For a broader understanding of the disease that connects cholesterol to cerebrovascular events, see what is atherosclerosis. For information on why high cholesterol is so often undetected until an event occurs, see high cholesterol symptoms and why testing matters.
Sources: American Heart Association — Stroke Risk Factors (stroke.org) | Centers for Disease Control and Prevention — Stroke Facts (cdc.gov) | National Heart, Lung, and Blood Institute — Stroke (nhlbi.nih.gov) | Amarenco P et al. (SPARCL). NEJM 2006;355:549–59 | Cholesterol Treatment Trialists’ Collaboration. Lancet 2010;376:1670–81 | Sabatine MS et al. (FOURIER). NEJM 2017;376:1713–22
Stroke vs. TIA: Why the Distinction Matters for Cholesterol Management
A transient ischemic attack (TIA) — often called a “mini-stroke” — produces the same neurological symptoms as an ischemic stroke (sudden weakness on one side of the body, difficulty speaking, vision loss in one eye, facial drooping) but resolves completely within 24 hours, usually within minutes. The resolution occurs because the arterial occlusion is temporary — the embolus breaks up and flow is restored before permanent neuronal death occurs.
TIAs are not benign events. They are urgent warnings. The risk of a full ischemic stroke in the days and weeks following a TIA is high: approximately 10 to 15 percent of people who have a TIA will have a full stroke within 90 days, with the highest risk concentrated in the first 48 hours. This makes TIA one of the most time-sensitive medical situations in cardiovascular medicine.
From a cholesterol management perspective, a TIA from large artery atherosclerosis carries the same treatment implications as a completed ischemic stroke: high-intensity statin therapy targeting LDL below 70 mg/dL, initiated urgently. The SPARCL trial included both stroke and TIA patients in its population — and the benefit of atorvastatin 80 mg was demonstrated across both groups. The premise is straightforward: if a carotid plaque was unstable enough to shed an embolus that caused a TIA, it is likely to be unstable enough to do so again — and the next time, the consequences may be permanent.
Cholesterol management is therefore not a long-term chronic disease intervention in the TIA setting — it is an urgent intervention begun in the hospital or emergency setting, alongside antiplatelet therapy, blood pressure optimization, and (if AF is identified as the cause) anticoagulation.
How Cholesterol Management Fits Into Overall Stroke Prevention
Stroke is a multifactorial disease. Cholesterol — specifically LDL — is one important modifiable risk factor for ischemic stroke, but it is far from the only one. Understanding where LDL management fits relative to other interventions helps prioritize the effort appropriately.
Blood pressure is the single largest contributor to stroke risk of any modifiable factor. The INTERSTROKE study — a large international case-control study of stroke in 32 countries — found that hypertension accounted for the largest fraction of population-attributable risk, exceeding the contribution of lipids, smoking, physical inactivity, and other factors. This does not diminish the importance of LDL lowering; it means that for most stroke patients, blood pressure control is an equally urgent priority, and the two interventions complement rather than substitute for each other.
Smoking is the second most impactful individual modifiable risk factor for ischemic stroke in most Western population analyses. It acts through direct carotid endothelial toxicity, oxidative LDL modification, and prothrombotic effects on platelets and coagulation proteins. A smoker with modestly elevated LDL has dramatically higher carotid atherosclerosis risk than a non-smoker with the same LDL. Smoking cessation reduces stroke risk substantially within one to two years of quitting.
Physical inactivity is an independent stroke risk factor, operating through multiple pathways: higher body weight, more abdominal fat, insulin resistance, dyslipidemia, and higher resting blood pressure are all more prevalent in sedentary individuals. Regular aerobic activity (150 or more minutes per week of moderate intensity) reduces stroke risk through all of these pathways simultaneously, with additional direct benefits on endothelial function and vascular reactivity.
Diabetes substantially amplifies stroke risk at any given LDL level — diabetes approximately doubles the ischemic stroke risk associated with a specific cholesterol value. This is because hyperglycemia accelerates endothelial glycation, oxidative LDL modification, and carotid plaque progression. Glycemic control (though the evidence for cardiovascular benefit of intensive glycemic control is more complex than for blood pressure or LDL) reduces the overall vascular damage that diabetes accelerates.
The practical framework: optimal stroke prevention requires simultaneous attention to LDL (statin therapy), blood pressure (antihypertensive therapy), smoking (cessation programs), physical activity, diet, glycemic control in diabetics, and AF detection and management. Addressing LDL alone while ignoring blood pressure of 160/100 mmHg or ongoing smoking leaves the most impactful risk factors unaddressed. The evidence-based goal is comprehensive risk factor management — LDL is a critical piece, but not the whole picture.
Cholesterol Management After Ischemic Stroke: What to Expect
For patients who have already experienced an ischemic stroke caused by large artery atherosclerosis, cholesterol management becomes a permanent priority — not a temporary measure to be stopped once cholesterol numbers look better on a lab report.
High-intensity statin therapy is typically initiated before hospital discharge after an atherosclerotic ischemic stroke. The most commonly prescribed high-intensity statins are rosuvastatin (20–40 mg daily) and atorvastatin (40–80 mg daily). These doses reduce LDL by 50 percent or more from baseline. The LDL target in secondary prevention after atherosclerotic stroke is below 70 mg/dL; in patients with multiple risk factors or recurrent events, below 55 mg/dL may be targeted.
If LDL does not reach the target on maximum-tolerated statin alone, ezetimibe is added first (typically reducing LDL by an additional 15 to 25 percent with minimal additional side effects). If the target is still not reached, a PCSK9 inhibitor — administered by subcutaneous injection every two to four weeks — is the next step. The combination of high-intensity statin plus ezetimibe plus PCSK9 inhibitor can reduce LDL to 20 to 30 mg/dL in most patients, providing very substantial plaque stabilization and recurrent stroke risk reduction.
Patients sometimes ask whether they can stop statin therapy once their LDL reaches the target. The answer is no — the goal is not a number on a lab test but the ongoing suppression of LDL to levels that prevent further carotid plaque growth and stabilize existing vulnerable plaques. Discontinuing statin therapy in secondary prevention returns LDL to pre-treatment levels within weeks and immediately resumes plaque-building conditions in the carotid arteries.
The Role of Lifestyle in Cholesterol and Stroke Risk Reduction
Medication alone does not capture the full potential for cholesterol-related stroke risk reduction. Lifestyle modifications that lower LDL, reduce inflammation, improve endothelial function, and address other concurrent risk factors (blood pressure, weight, blood sugar) contribute meaningfully to long-term stroke risk reduction — and they amplify the benefit of statin therapy rather than substituting for it.
Diet. A Mediterranean-style dietary pattern — emphasizing vegetables, legumes, whole grains, fish, nuts, and olive oil while limiting saturated fat, processed meats, and refined carbohydrates — reduces LDL and systemic inflammation simultaneously. The PREDIMED trial demonstrated a 30 percent relative reduction in major cardiovascular events in high-risk adults randomized to a Mediterranean diet supplemented with olive oil or nuts, compared to a low-fat control diet. For stroke specifically, the Mediterranean dietary pattern has been associated with reduced ischemic stroke risk in multiple prospective cohort studies, with the benefit operating through LDL lowering, blood pressure reduction, anti-inflammatory effects, and improvements in endothelial function.
Exercise. Regular aerobic activity of at least 150 minutes per week of moderate intensity reduces stroke risk through multiple simultaneous pathways: LDL reduction, blood pressure reduction, HDL increase, triglyceride reduction, improved insulin sensitivity, and direct vascular benefits including enhanced endothelial nitric oxide production. People who are regularly physically active have substantially lower ischemic stroke incidence than sedentary individuals in prospective epidemiological studies, independent of other risk factor differences.
Alcohol moderation. Heavy alcohol consumption (more than two drinks per day consistently) raises blood pressure, increases triglycerides, and is associated with increased stroke risk — including both ischemic and hemorrhagic subtypes. Moderate alcohol intake (one to two drinks per day in men, one in women) has an inconsistent relationship with ischemic stroke risk in observational data. Current guidance does not recommend alcohol consumption as a cardiovascular protective strategy, and anyone with elevated triglycerides, hypertension, or prior stroke should minimize or eliminate alcohol.