Type 1 vs Type 2 Diabetes: What Is the Difference?
The question of type 1 vs type 2 diabetes — what separates them, how they develop, and why the distinction matters — is one of the most commonly misunderstood aspects of metabolic health. Both conditions are defined by elevated blood glucose, both carry serious long-term health consequences, and both are called “diabetes.” But they are fundamentally different diseases with different causes, different populations affected, different mechanisms of damage, and different treatment requirements. Confusing the two leads to incorrect assumptions about who is responsible for their diagnosis, what treatment they need, and whether the condition could have been prevented. This guide explains the key differences between Type 1 and Type 2 diabetes in detail — and why those differences matter for understanding, managing, and communicating about these conditions accurately.
The Fundamental Distinction: Cause and Mechanism
The most important difference between type 1 vs type 2 diabetes lies in their underlying cause. These are not mild and severe versions of the same condition — they are mechanistically distinct diseases that happen to produce similar symptoms and the same measurable outcome (elevated blood sugar) through completely different pathways.
Type 1 diabetes is an autoimmune disease. The immune system, which normally defends the body against bacteria and viruses, makes a critical error and begins attacking the insulin-producing beta cells in the pancreas. This attack continues over months to years until the beta cells are destroyed and the pancreas can no longer produce insulin at all. Without insulin, glucose cannot enter cells, blood sugar rises rapidly, and the body begins breaking down fat and muscle for energy — a metabolic crisis that, before the discovery of insulin in 1921, was invariably fatal within months of onset. Type 1 diabetes is not caused by diet, lifestyle, or behavior. It is an autoimmune condition that can develop in anyone, and it has nothing to do with how much sugar a person has eaten.
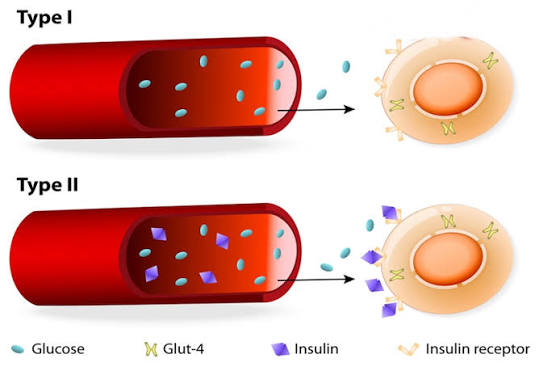
Type 2 diabetes develops through a different process involving two interrelated failures: insulin resistance and declining beta cell function. The beta cells in people with Type 2 diabetes are not destroyed by the immune system — they continue working, sometimes for decades. The problem is that the body’s cells become progressively resistant to the signal that insulin sends, requiring ever-larger amounts of insulin to manage blood sugar. Over time, the pancreatic beta cells cannot keep up with this demand, their function declines, and blood sugar begins rising. Lifestyle factors — particularly excess body weight, physical inactivity, poor diet quality, and insufficient sleep — drive insulin resistance and accelerate beta cell exhaustion. Genetics also play a significant role.
Understanding what is diabetes and how the body normally regulates blood sugar is foundational to understanding both types. See our guide on what is diabetes for a comprehensive overview of the condition and its mechanisms.
Who Gets Type 1 vs Type 2 Diabetes
The populations affected by Type 1 and Type 2 diabetes overlap but differ in important ways.
Type 1 diabetes can develop at any age, but it most commonly appears in childhood, adolescence, and young adulthood — which is why it was historically called “juvenile diabetes,” though this term is now considered outdated and misleading since adults can and do develop Type 1. The peak ages of onset in children are between 4 and 7 years and between 10 and 14 years. A form of Type 1 diabetes called LADA (Latent Autoimmune Diabetes in Adults) develops more slowly in adults aged 30 to 50 and is frequently misdiagnosed as Type 2 because it presents with less dramatic symptoms in older adults. Type 1 affects approximately 5 to 10 percent of all people with diabetes in the United States.
Type 2 diabetes historically was called “adult-onset diabetes” because it rarely appeared before middle age. That term is also now outdated — in parallel with the obesity epidemic, Type 2 diabetes has become increasingly common in children and adolescents, particularly those who are overweight. The risk of Type 2 diabetes increases significantly with age (particularly after 45), but the condition now affects people across all age groups. It accounts for 90 to 95 percent of all diabetes diagnoses.
Ethnicity affects risk for both types but particularly for Type 2: Black, Hispanic, Native American, Asian American, and Pacific Islander adults in the United States face significantly higher rates of Type 2 diabetes than white Americans, partly due to differences in the distribution of metabolic risk factors and partly due to underlying genetic differences in insulin sensitivity and beta cell function at any given body weight.
- Cause: Type 1 = autoimmune beta cell destruction | Type 2 = insulin resistance + beta cell exhaustion
- Insulin production: Type 1 = none (or near none) | Type 2 = reduced but present (especially early)
- Onset: Type 1 = often rapid (days–weeks) | Type 2 = slow and silent (years)
- Age at onset: Type 1 = any age, peaks in childhood | Type 2 = any age, rises sharply after 45
- Body weight: Type 1 = not linked to weight | Type 2 = strongly linked to overweight/obesity
- Treatment: Type 1 = insulin required from diagnosis | Type 2 = lifestyle, oral meds, insulin if needed
- Prevention: Type 1 = not currently preventable | Type 2 = largely preventable with lifestyle changes
Onset and Symptom Progression
The speed at which diabetes develops and produces symptoms differs dramatically between types.
Type 1 diabetes typically presents suddenly and dramatically, particularly in children. Once enough beta cells have been destroyed that insulin production can no longer maintain blood sugar, glucose levels rise rapidly. Symptoms appear and intensify over days to weeks: extreme thirst, very frequent urination, rapid unexplained weight loss, blurry vision, severe fatigue, and sometimes abdominal pain. If undiagnosed, Type 1 can progress to diabetic ketoacidosis (DKA) — a life-threatening condition in which the body, starved of glucose, begins breaking down fat into acidic ketone bodies that overwhelm the blood’s buffering capacity. DKA presents with nausea, vomiting, abdominal pain, fruity-smelling breath, and can lead to loss of consciousness and death if untreated. It is a medical emergency requiring hospital admission.
Type 2 diabetes develops over years to decades and often produces no symptoms at all in its early stages. The gradual progression from normal glucose tolerance to prediabetes to Type 2 diabetes can unfold over a decade or more without any noticeable effects. When symptoms do appear, they are often mild and easily attributed to aging, stress, or fatigue: mild increased thirst, slightly more frequent urination, occasional blurry vision, fatigue after meals. Many people learn they have Type 2 diabetes only through routine blood testing during a physical exam — or, in some cases, when they present with a complication such as a wound that won’t heal, a first kidney disease diagnosis, or vision loss from diabetic retinopathy that has been developing silently for years.
This difference in onset has profound implications. People with Type 1 are usually diagnosed in a crisis; people with Type 2 are often diagnosed incidentally, if at all. Widespread screening is essential to catch Type 2 diabetes before years of elevated blood sugar have already caused irreversible damage.
Insulin: Who Needs It and Why
Insulin is the central treatment difference between Type 1 and Type 2 diabetes, and understanding why clarifies much of the confusion around both conditions.
People with Type 1 diabetes require insulin from the time of diagnosis — there is no alternative. Because their pancreas produces no insulin (or near none), they must replace it externally to survive. Without insulin injections or an insulin pump, blood sugar would rise continuously until DKA developed. Type 1 diabetes management involves calculating insulin doses for every meal based on carbohydrate content, planning around exercise and illness that affect insulin requirements, and monitoring blood sugar continuously. There is no pill that can replace the insulin these individuals must inject or infuse.
People with Type 2 diabetes may or may not need insulin, depending on how far their beta cell function has declined. Early in Type 2, lifestyle changes (diet, exercise, weight loss) combined with oral medications — most commonly metformin — may be sufficient to keep blood sugar under control. As the condition progresses and beta cell function declines further, additional medications may be added. Some people with advanced Type 2 diabetes eventually need insulin as well, when their beta cells can no longer produce enough even with medication support. However, needing insulin does not mean a person has “failed” at managing their condition — it means the underlying disease has progressed, which happens to many people regardless of how carefully they manage it.
The confusion between insulin needs in Type 1 and Type 2 has unfortunately contributed to stigma around insulin use in Type 2 diabetes, with some patients resisting insulin because it feels like giving up. This is a harmful misconception: insulin is a medication that saves lives and reduces complications, and the decision to use it should be made based on medical need, not perceived failure.
Risk Factors: What Increases the Likelihood
The risk factors for Type 1 and Type 2 diabetes are almost entirely different, which reflects their distinct underlying causes.
Type 1 diabetes risk factors:
- Family history: Having a parent or sibling with Type 1 diabetes increases risk, though most people with Type 1 have no affected relatives — suggesting that most cases arise from de novo autoimmune activation rather than simple heredity
- HLA gene variants: Certain combinations of HLA-DR and HLA-DQ genes on chromosome 6 significantly increase susceptibility to the autoimmune attack. Testing for these variants can identify individuals at elevated risk before any symptoms develop
- Autoantibodies: The presence of specific antibodies (islet cell antibodies, insulin antibodies, GAD antibodies) in the blood indicates that the autoimmune process has begun, even before blood sugar rises. These can be detected years before clinical Type 1 develops
- Viral infections: Certain enteroviruses have been associated with triggering the autoimmune cascade in genetically susceptible individuals, though the exact mechanism remains under investigation
- Geography: Type 1 is more common in countries farther from the equator — Finland has one of the highest rates in the world — for reasons that may involve vitamin D, viral exposure patterns, or other environmental factors
Type 2 diabetes risk factors:
- Overweight or obesity: Excess body fat — particularly visceral fat around the abdomen — releases inflammatory hormones that impair insulin signaling throughout the body
- Physical inactivity: Muscle is the primary site of insulin-stimulated glucose uptake. Sedentary lifestyles reduce muscle insulin sensitivity significantly
- Age: Risk rises sharply after 45, when both insulin sensitivity and beta cell function naturally decline with aging
- Family history: Having a parent or sibling with Type 2 diabetes significantly increases risk, reflecting shared genetic susceptibility to insulin resistance
- Prediabetes: Blood sugar in the prediabetes range indicates that insulin resistance is already present. Without intervention, prediabetes progresses to Type 2 diabetes in many people. Learn more in our guide on what is prediabetes
- Prior gestational diabetes: Women who developed gestational diabetes during pregnancy face up to a 50 percent lifetime risk of developing Type 2 diabetes
- Polycystic ovary syndrome (PCOS): A condition that involves insulin resistance as a core feature, significantly elevating Type 2 diabetes risk in affected women
Long-Term Complications: What Both Types Share
Despite their different causes and mechanisms, Type 1 and Type 2 diabetes share the same long-term complications, because both involve elevated blood glucose that damages the same tissues over time. Sustained hyperglycemia causes glycation of proteins throughout the body, accelerated atherosclerosis, damage to the small blood vessels supplying the kidneys, retinas, and peripheral nerves, and impaired immune function.
The major complications include:
- Cardiovascular disease: People with diabetes face two to four times the risk of heart attack and stroke. Heart disease is the leading cause of death in both Type 1 and Type 2 diabetes
- Diabetic kidney disease (nephropathy): The leading cause of chronic kidney disease requiring dialysis in the United States
- Diabetic eye disease (retinopathy): The leading cause of preventable blindness in working-age adults
- Peripheral neuropathy: Nerve damage causing tingling, numbness, burning pain, and eventual loss of sensation in the feet and legs, increasing the risk of serious foot wounds
- Autonomic neuropathy: Damage to the nerves controlling internal organs, affecting digestion (gastroparesis), heart rate variability, and blood pressure regulation
The good news is that these complications are largely preventable with good blood sugar control, blood pressure management, and regular screening. The risk of complications rises steeply when A1C stays above 7 to 8 percent for extended periods, and falls significantly with tighter control. Understanding blood sugar after meals — where much of the glucose exposure accumulates — is also important; see our guide on blood sugar after meals for details.
Prevention: A Key Practical Difference
One of the most practically significant differences between Type 1 and Type 2 diabetes is preventability.
Type 1 diabetes cannot currently be prevented. Because it is an autoimmune condition triggered by genetic and environmental factors not fully under an individual’s control, there are no established lifestyle interventions that reduce its risk. Research into early immune intervention — treating high-risk individuals (identified by autoantibody screening) with immune-modulating therapies before beta cell destruction is complete — is advancing, and one medication (teplizumab) has received FDA approval to delay the onset of clinical Type 1 in at-risk individuals. But prevention at the population level is not yet possible.
Type 2 diabetes is substantially preventable. The evidence base is extensive and consistent. The Diabetes Prevention Program demonstrated a 58 percent reduction in progression from prediabetes to Type 2 diabetes with structured lifestyle intervention (modest weight loss of 5 to 7 percent of body weight, and 150 minutes of moderate activity per week). Similar results have been replicated globally. For people at risk, the message is clear: lifestyle changes made before Type 2 diabetes develops are among the most powerful health interventions available. The window of opportunity offered by a prediabetes diagnosis should not be dismissed.
The Stigma Problem: Why Getting It Right Matters
Confusion between Type 1 and Type 2 diabetes — and particularly the incorrect belief that “diabetes is caused by eating too much sugar” — contributes to significant stigma that affects millions of people. People with Type 1 diabetes frequently encounter the assumption that their condition resulted from poor diet choices. People with Type 2 face moralizing assumptions that they “gave themselves” diabetes through laziness or self-indulgence, which ignores the powerful roles of genetics, socioeconomic factors, food environment, and healthcare access.
Both of these narratives are harmful and factually wrong. Type 1 diabetes is an autoimmune disease with no behavioral cause. Type 2 diabetes results from a complex interaction of genetic predisposition and environmental factors, and the degree of personal agency involved varies enormously among individuals. Accurate understanding of the actual mechanisms — what is blood sugar, how insulin works, what makes cells resistant, how beta cells fail — is the foundation for replacing stigma with effective support and evidence-based care.
Monitoring Blood Sugar: Similar Tools, Different Goals
Both Type 1 and Type 2 diabetes require blood glucose monitoring, but the frequency and purpose differ based on the type and how it is being treated.
People with Type 1 diabetes typically monitor very frequently — often eight to twelve times per day or continuously via a CGM — because every insulin dose must be calibrated to the current blood sugar level, anticipated carbohydrate intake, and upcoming physical activity. Missing a dose or misjudging a correction can lead to dangerous highs or hypoglycemia within hours. For people on insulin pumps with CGM integration (closed-loop or “artificial pancreas” systems), much of this calculation is automated — but understanding the data remains essential. For a detailed look at home monitoring tools, see our guide on home blood sugar monitoring.
People with Type 2 diabetes who are not using insulin often monitor less frequently — sometimes only at fasting once or twice per week to track trends — because their blood sugar fluctuates more gradually and their medication does not require minute-to-minute glucose data to dose safely. However, those on insulin regimens for Type 2 require much more frequent monitoring, similar to Type 1. The A1C test, checked every three to six months, provides the most important long-term measure of control for Type 2 management, reflecting average blood sugar over the prior two to three months. For a full explanation of this test and what the numbers mean, see our guide on the A1C test.
Hypoglycemia Risk: An Important Difference in Day-to-Day Safety
Low blood sugar — hypoglycemia — is a significant concern for people with Type 1 diabetes and for those with Type 2 diabetes using insulin or sulfonylurea medications. However, the risk profiles differ considerably.
People with Type 1 diabetes face hypoglycemia risk every day, at every meal, and during any activity, because their insulin dose must be calculated and matched to glucose levels that are constantly changing. A meal smaller than anticipated, unexpected exercise, or a slightly higher-than-needed insulin dose can all cause blood sugar to drop below 70 mg/dL quickly. Severe hypoglycemia — with confusion, loss of consciousness, or seizure — is a real and recurring risk, particularly overnight when the person cannot monitor their own symptoms. This constant vigilance is one of the most demanding aspects of life with Type 1 diabetes.
People with Type 2 diabetes who manage their condition with lifestyle changes alone, or with medications that do not stimulate insulin secretion (such as metformin, GLP-1 agonists, or SGLT-2 inhibitors), face very low hypoglycemia risk. However, those on sulfonylureas or insulin do face meaningful hypoglycemia risk and need to monitor accordingly. Understanding this difference helps healthcare providers choose medications that maintain effective blood sugar control with the lowest possible risk of dangerous lows.
Outlook and Disease Trajectory
The long-term trajectory differs between the two types in important ways. Type 1 diabetes is a lifelong condition in which the absence of insulin production does not change — management becomes more sophisticated over time with better technology, but the fundamental insulin dependence persists throughout life. There is no reversal or remission for Type 1 in the traditional sense, though islet cell transplantation has produced insulin independence in some patients, and research continues into immunotherapy and beta cell regeneration.
Type 2 diabetes, in contrast, exists on a spectrum. In its early stages, with aggressive lifestyle intervention and sometimes medication, blood sugar can return to the normal range — a state often called “remission.” The DiRECT trial, published in The Lancet, demonstrated that roughly half of people with Type 2 diabetes who lost 15 kilograms or more through a structured low-calorie diet program achieved remission at one year. Remission does not mean the underlying metabolic vulnerability has disappeared — it can return with weight regain or aging — but it demonstrates that Type 2 diabetes is not invariably progressive if metabolic conditions change sufficiently.
Both conditions are compatible with long, healthy, full lives when managed effectively. The key is early diagnosis, consistent management, regular monitoring for complications, and access to current treatment options — including the remarkable advances in continuous glucose monitoring, insulin delivery technology, and newer medication classes that have transformed outcomes for people living with both Type 1 and Type 2 diabetes over the past two decades.
Sources: American Diabetes Association. Standards of Medical Care in Diabetes — 2024. Diabetes Care. 2024;47(Suppl 1):S20–S42. • Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2022. CDC; 2022. • Insel RA, et al. Staging presymptomatic type 1 diabetes: a scientific statement of JDRF, the Endocrine Society, and the American Diabetes Association. Diabetes Care. 2015;38(10):1964–1974.