Most people have heard the shorthand: LDL is bad cholesterol, HDL is good cholesterol. It is a useful simplification for a first pass, but it obscures the actual biology — and if your doctor is asking you to pay closer attention to these numbers, the shorthand alone won’t help you understand what to do about them.
LDL vs HDL cholesterol is really a story about direction. Both types carry cholesterol through the bloodstream, but they move it in opposite directions and the consequences of that difference are profound. Understanding what each type does, why the balance between them matters, and what shifts that balance gives you a framework that actually informs decisions rather than just creating anxiety about lab results.
What LDL Cholesterol Is and What It Does
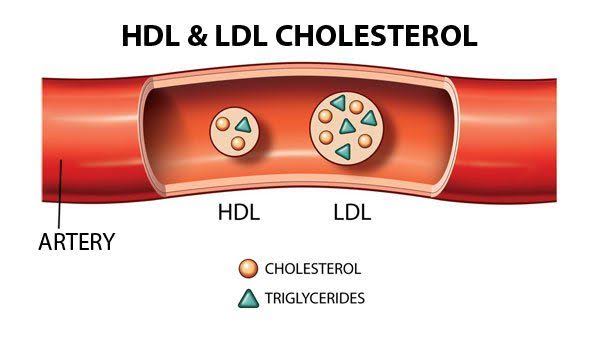
LDL stands for low-density lipoprotein. Lipoproteins are the transport vehicles the body uses to move cholesterol and fats through the watery environment of blood — cholesterol cannot dissolve in water, so it requires these protein-coated carriers to circulate.
LDL particles carry a significant load of cholesterol — roughly 50 percent cholesterol by weight. LDL’s job is to transport cholesterol from the liver, where most of it is produced, out to cells throughout the body. Cells use LDL receptors on their surface to pull in LDL particles and extract the cholesterol they need for cell membrane construction, hormone synthesis, and other metabolic functions.
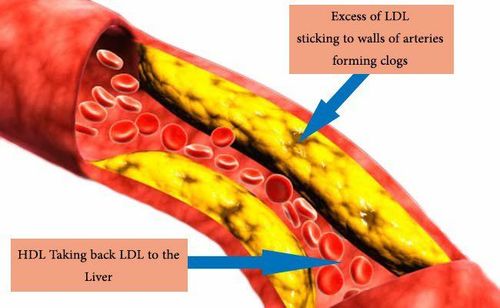
At appropriate levels, LDL is necessary and normal. The problem arises when LDL levels are persistently elevated. Excess LDL particles circulate longer than normal and eventually penetrate the inner lining of artery walls. Once inside, LDL particles become oxidized and trigger an immune response — macrophages are recruited to engulf the oxidized LDL, becoming foam cells. These foam cells accumulate over time and form the fatty streaks that develop into atherosclerotic plaques. Plaques narrow arteries, reduce blood flow, and can rupture — triggering blood clots that cause heart attacks and strokes.
LDL particle size matters too. Not all LDL particles behave identically. Small, dense LDL particles (pattern B) are more atherogenic than large, buoyant LDL particles (pattern A) because they penetrate artery walls more easily and are more susceptible to oxidation. People with metabolic syndrome, insulin resistance, and high triglycerides tend to have a higher proportion of small dense LDL — this is one reason triglycerides appear on cardiovascular risk assessments alongside LDL.
What HDL Cholesterol Is and What It Does
HDL stands for high-density lipoprotein. Compared to LDL, HDL particles are smaller, denser, and contain more protein relative to cholesterol — roughly 50 percent protein. This high protein content is what makes HDL heavy (dense) and gives it a completely different function.
HDL operates in reverse. Instead of delivering cholesterol to cells, HDL collects cholesterol from tissues — including from artery walls and macrophage foam cells — and transports it back to the liver. The liver then recycles the cholesterol, converts it into bile acids, or excretes it. This process is called reverse cholesterol transport, and it is the primary mechanism by which HDL is thought to protect against cardiovascular disease.
HDL also appears to have anti-inflammatory properties that dampen arterial inflammation, antioxidant effects that may inhibit LDL oxidation, and antithrombotic properties that reduce blood clot formation on plaque surfaces.
The HDL paradox. The relationship between HDL and cardiovascular risk is more complex than early research suggested. In observational studies, high HDL consistently correlates with lower cardiovascular event rates. However, clinical trials that pharmacologically raised HDL — using niacin and CETP inhibitors — failed to reduce cardiovascular events despite dramatically increasing HDL levels. The AIM-HIGH trial (2011) and HPS2-THRIVE trial (2014) both showed no benefit from niacin-driven HDL increases. Several CETP inhibitors raised HDL by 40 to 130 percent but produced no clinical benefit, and torcetrapib was associated with increased mortality.
Researchers now recognize that HDL cholesterol concentration and HDL function — how effectively it actually performs reverse cholesterol transport — are not the same thing. “Dysfunctional HDL” may be high in cholesterol but impaired at removing it from arterial tissue. This is why current guidelines focus primarily on LDL reduction as the treatment target rather than HDL elevation.
LDL and HDL Reference Ranges
<100 mg/dL — Optimal for most adults; goal for high-risk patients
100–129 mg/dL — Near optimal
130–159 mg/dL — Borderline high
160–189 mg/dL — High
≥190 mg/dL — Very high; consider familial hypercholesterolemia
40–59 mg/dL — Acceptable
≥60 mg/dL — High; considered protective
LDL targets are not universal thresholds — they are goals adjusted by overall cardiovascular risk. A person with established coronary artery disease has a stricter LDL goal than a healthy person with no risk factors. For more on how these numbers are interpreted in context, see our article on total cholesterol: how to understand your results.
What Your Cholesterol Ratio Means
Total cholesterol to HDL ratio is calculated by dividing total cholesterol by HDL. A ratio below 4.0 is considered desirable; above 5.0 indicates elevated cardiovascular risk. A rising ratio can reflect increasing LDL, decreasing HDL, or both simultaneously.
Non-HDL cholesterol equals total cholesterol minus HDL and captures all cholesterol carried in potentially harmful lipoproteins — LDL, VLDL, IDL, and Lp(a). Because it requires no additional calculation beyond a standard lipid panel, non-HDL is increasingly favored as a more comprehensive risk measure than LDL alone. A non-HDL level below 130 mg/dL is generally desirable.
Apolipoprotein B (ApoB) measures the total count of atherogenic lipoprotein particles. Because each atherogenic particle carries exactly one ApoB molecule, ApoB directly counts potentially harmful particles regardless of their cholesterol content. ApoB can detect elevated particle counts in people whose LDL cholesterol appears normal — this “discordance” between LDL-C and ApoB is an important limitation of standard cholesterol testing. For a detailed look at the lipid panel tests used to measure these values, see our guide to what is a lipid panel.
What Raises LDL and Lowers HDL
Several factors push the cholesterol balance in the wrong direction simultaneously — raising LDL while lowering HDL, which is the worst possible combination for cardiovascular risk.
Saturated fat is the primary dietary driver of elevated LDL. It reduces LDL receptor activity in the liver, decreasing LDL clearance from the blood. Major sources: fatty red meat, butter, full-fat dairy, coconut oil, and palm oil.
Trans fat raises LDL and lowers HDL simultaneously. Partially hydrogenated vegetable oils — the primary trans fat source — have been largely removed from the US food supply since 2018, but trace amounts remain in some processed foods.
Physical inactivity is strongly associated with low HDL. Aerobic exercise is one of the most reliable lifestyle modifications for raising HDL levels.
Smoking directly lowers HDL by approximately 5 mg/dL and appears to oxidize LDL particles, making them more atherogenic.
Refined carbohydrates and added sugars lower HDL and raise triglycerides, which promotes production of small dense LDL particles.
Obesity and insulin resistance — particularly abdominal fat — impair lipid metabolism broadly: raising triglycerides and VLDL, lowering HDL, and shifting LDL composition toward the more atherogenic small dense pattern. To understand the downstream effects of these lipid changes, see our article on triglycerides and heart health.
What Lowers LDL and Raises HDL
The interventions that improve the cholesterol balance operate through several distinct mechanisms.
Replacing saturated fat with unsaturated fat is the dietary change with the strongest evidence. Monounsaturated fats (olive oil, avocados, almonds) and polyunsaturated fats (sunflower oil, walnuts, fatty fish) lower LDL without reducing HDL. This substitution — not simply reducing total fat — is what cardiovascular nutrition guidelines emphasize.
Aerobic exercise consistently raises HDL by 5 to 10 percent with regular practice. The minimum effective dose appears to be about 30 minutes of moderate-intensity aerobic exercise most days of the week. Exercise also modestly reduces LDL and triglycerides.
Weight loss improves the entire lipid profile. Losing 5 to 10 percent of body weight raises HDL, lowers LDL, and reduces triglycerides simultaneously.
Soluble fiber — from oats, barley, beans, and psyllium — binds bile acids in the intestine and reduces LDL by 5 to 10 percent when consumed consistently at 5 to 10 grams daily.
Quitting smoking raises HDL by an average of 4 to 5 mg/dL within weeks of cessation. Smoking cessation also removes the oxidative damage to LDL particles that makes them more atherogenic.
Plant sterols and stanols (2 grams per day) reduce LDL by competing with cholesterol for intestinal absorption. They are available in fortified foods and supplements.
Statins remain the most effective pharmacological intervention for LDL reduction — lowering LDL by 30 to 60 percent depending on dose — while also modestly raising HDL. When lifestyle modifications are insufficient to reach LDL targets, statins are the first-line pharmacological option.
Can You Have High HDL and Still Be at Risk?
The surprising answer is yes. The clinical trial failures described above — niacin and CETP inhibitors — established that pharmacologically elevated HDL does not consistently reduce cardiovascular events. But there is also observational evidence that very high HDL (above 80 mg/dL in some studies) does not confer the expected low risk, particularly when elevated through certain genetic variants.
What this means clinically: if your HDL is low, it is a meaningful risk factor worth addressing through lifestyle change. But if your HDL is high, it does not cancel out elevated LDL or other risk factors. LDL reduction and comprehensive risk factor control remain the primary goals.
When Medication Is Needed
Lifestyle changes are the foundation of cholesterol management and should always be attempted first in people without established cardiovascular disease. When they are insufficient — or when someone already has cardiovascular disease or very high LDL — medications become necessary.
Statins are the first-line pharmacological treatment. They block the liver enzyme that produces cholesterol, increasing LDL receptor expression and clearing more LDL from the blood. For people with established heart disease, stroke, or LDL ≥190 mg/dL, guidelines recommend high-intensity statins regardless of current LDL level.
Ezetimibe blocks intestinal cholesterol absorption and reduces LDL by an additional 15 to 20 percent when added to a statin. The IMPROVE-IT trial showed cardiovascular event reduction when it was combined with a statin.
PCSK9 inhibitors (evolocumab, alirocumab) are injectable antibodies that dramatically increase LDL receptor activity, reducing LDL by 50 to 60 percent even on top of maximally dosed statins. They are used in patients with familial hypercholesterolemia or established cardiovascular disease who do not reach LDL goals on statins alone.
Fibrates are sometimes used for low HDL combined with high triglycerides, primarily because they lower triglycerides by 20 to 50 percent and modestly raise HDL.
The goal is not simply to reach a number on a lab report — it is to reduce the probability of a cardiovascular event. Treatment decisions weigh LDL level, overall cardiovascular risk, and individual patient factors. For a broader overview of what causes high cholesterol and how treatment is decided, see our dedicated article on that topic.
LDL and HDL are not simply “good” and “bad” in any absolute sense. They are complementary components of a lipid transport system that works properly within a certain balance. When LDL rises beyond the liver’s clearance capacity, the arterial damage cascade begins. When HDL falls, less of that excess gets removed. The interventions that lower LDL — diet, exercise, weight loss, smoking cessation — tend to improve HDL simultaneously. They move the whole balance in the right direction, which is why lifestyle modification remains the foundation of treatment regardless of whether medication is also needed.
For related reading, see our articles on what is cholesterol, total cholesterol: how to understand your results, what is a lipid panel, triglycerides and heart health, and causes of high cholesterol.
How LDL and HDL Are Actually Measured
Understanding how these numbers are generated helps interpret their meaning — and their limitations.
A standard lipid panel measures total cholesterol, HDL, and triglycerides directly through enzymatic assays. LDL is typically not measured directly in routine testing — it is calculated using the Friedewald equation: LDL = Total Cholesterol − HDL − (Triglycerides ÷ 5). This formula works reasonably well when triglycerides are in the normal range, but becomes unreliable when triglycerides exceed 400 mg/dL, because the calculation assumes a fixed relationship between triglycerides and VLDL that breaks down at high triglyceride levels.
Direct LDL measurement is available but not routinely performed because it is more expensive. For most clinical decisions, the calculated LDL is sufficient. However, in people with high triglycerides — often those with metabolic syndrome or poorly controlled diabetes — direct LDL or non-HDL cholesterol becomes a more reliable guide.
The fasting question. Traditional lipid panels required 9 to 12 hours of fasting, primarily because recent meals raise triglycerides and cause the Friedewald LDL calculation to shift. However, guidelines have relaxed this requirement for many clinical purposes. Non-fasting total cholesterol, HDL, and non-HDL cholesterol are minimally affected by recent food intake. Non-fasting samples are now accepted for initial screening and routine monitoring in most settings, with fasting samples reserved for triglyceride measurement or when more precision is needed.
What a lipid panel does not capture. A standard lipid panel reports cholesterol concentration — the amount of cholesterol carried per deciliter of blood. It does not directly measure lipoprotein particle number. Two people can have identical LDL-C values but very different numbers of LDL particles: one person with large buoyant LDL carries more cholesterol per particle (fewer particles needed to achieve a given LDL-C), while another with small dense LDL carries less cholesterol per particle (more particles needed). The person with more particles faces greater cardiovascular risk at the same LDL-C. This discordance is one argument for measuring ApoB in addition to standard LDL-C, particularly in people with metabolic syndrome or diabetes.
LDL, HDL, and Cardiovascular Risk in Context
Cholesterol numbers do not determine cardiovascular risk in isolation — they interact with a cluster of other factors that either amplify or dampen their impact.
Blood pressure. Hypertension and elevated LDL compound each other’s risk. High blood pressure damages the arterial endothelium, making it easier for LDL particles to penetrate artery walls and initiate plaque formation. Controlling blood pressure alongside LDL produces greater cardiovascular risk reduction than addressing either factor alone.
Blood sugar and insulin resistance. Elevated blood sugar damages LDL particles through glycation (sugar molecules attaching to the protein component of LDL), making them more atherogenic and less efficiently cleared by LDL receptors. People with type 2 diabetes have a cardiovascular risk equivalent to people with established coronary artery disease by some guidelines, which is why LDL targets for diabetic patients are set as low as for people who have already had a heart attack.
Smoking. Smokers have lower HDL, more oxidized LDL, and higher inflammatory markers — a convergence of lipid and non-lipid risk factors that makes their cardiovascular risk substantially higher than would be predicted from cholesterol numbers alone. Quitting smoking is one of the highest-impact cardiovascular risk reductions available.
Age and sex. LDL naturally rises with age, and the cardiovascular risk associated with a given LDL level rises correspondingly. Women before menopause tend to have higher HDL and lower LDL than age-matched men, a gap that largely closes after menopause when estrogen levels drop. Postmenopausal women may benefit from more aggressive LDL monitoring and management than they received earlier in life.
Family history. A first-degree relative who had a heart attack before age 55 (for fathers) or 65 (for mothers) is a major independent risk factor. People with significant family history may need more aggressive lipid management even if their numbers appear borderline by standard thresholds, because the absolute risk over a lifetime of exposure to elevated LDL is higher.
Inflammation. High-sensitivity C-reactive protein (hsCRP) is a marker of systemic inflammation and an independent cardiovascular risk predictor. It can help reclassify people whose 10-year risk falls in the intermediate range — those who might or might not benefit from statin therapy. The JUPITER trial showed that people with normal LDL but elevated hsCRP benefited from statin therapy, reinforcing the concept that LDL-independent mechanisms (including inflammation) drive cardiovascular risk.
Common Questions About LDL and HDL
Can you have normal total cholesterol but still have high LDL? Yes. Total cholesterol includes all cholesterol components — LDL, HDL, VLDL, and others. A person with low HDL and elevated LDL can have a total cholesterol that appears acceptable while their individual components are problematic. This is why total cholesterol alone is considered an inferior screening tool compared to a full lipid panel.
Does eating fatty food directly raise your LDL? Only in the sense that dietary saturated and trans fats raise LDL over time by affecting liver metabolism. A single high-fat meal raises triglycerides transiently but does not substantially change LDL within the timeframe of a cholesterol test. This is why fasting requirements for LDL measurement are less stringent than for triglycerides.
Is there such a thing as too low LDL? Very low LDL is generally not harmful in itself. People with familial hypobetalipoproteinemia — a genetic condition causing very low LDL from birth — tend to have reduced cardiovascular risk and do not appear to suffer adverse health consequences from low LDL alone. However, extremely low cholesterol in adults who previously had normal levels can occasionally signal underlying disease (certain cancers, liver failure, severe malnutrition) rather than a benign genetic variant, and warrants evaluation if unexplained.
Does HDL always protect against heart disease? At population level, higher HDL is consistently associated with lower cardiovascular risk. But as described above, this relationship does not hold reliably for pharmacologically raised HDL. At the individual level, genetically high HDL also does not always confer protection — some genetic variants raise HDL without improving (and in some cases while worsening) cholesterol transport function.
Can LDL and HDL numbers fluctuate? Yes, though usually not dramatically between measurements a few weeks apart under stable conditions. Cholesterol levels can shift meaningfully with major dietary changes, significant weight change, pregnancy, thyroid disease, and certain medications. Single measurements should be interpreted in context, and trending over multiple tests is more informative than reacting to a single data point.
The Practical Takeaway
The bottom line for understanding LDL vs HDL cholesterol comes down to four principles that hold across guidelines and clinical practice:
First, LDL is the primary actionable target. The causal evidence linking LDL to atherosclerosis is strong, consistent, and mechanistically clear. Lowering LDL reduces cardiovascular events — in clinical trials, every 1 mmol/L (roughly 39 mg/dL) reduction in LDL reduces major cardiovascular events by approximately 22 percent over five years. The evidence base for LDL-lowering interventions (diet, exercise, statins) is among the most robust in cardiovascular medicine.
Second, HDL is a risk indicator but not a reliable treatment target. Low HDL signals increased risk and is worth addressing through lifestyle — but pharmacologically raising HDL has not proven to reduce events. Think of HDL as a gauge that reflects the quality of lipid metabolism rather than a lever to pull independently.
Third, the ratio and non-HDL measures add context that individual numbers miss. A total cholesterol/HDL ratio above 5.0 or a non-HDL above 130 mg/dL can flag elevated risk even when LDL appears borderline, particularly in people with metabolic syndrome or high triglycerides.
Fourth, cholesterol numbers are inputs into a risk calculation, not the final answer. Age, blood pressure, smoking status, diabetes, family history, and inflammatory markers all interact with LDL and HDL levels to determine actual cardiovascular risk. Decisions about treatment should be based on this overall calculation — which is why the conversation with a physician or cardiologist remains essential rather than self-managing based on individual numbers alone.