Ischemic vs Hemorrhagic Stroke: Key Differences

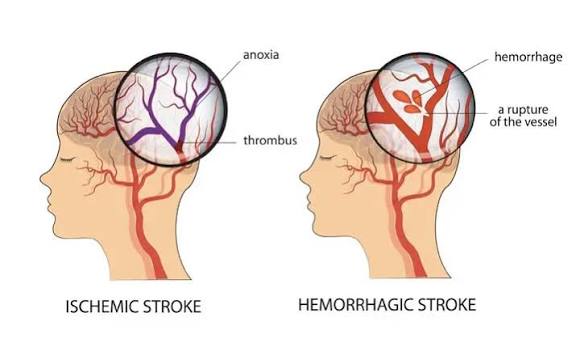
When a stroke occurs, one of the most critical determinations in all of emergency medicine is whether it is ischemic (caused by blocked blood flow) or hemorrhagic (caused by bleeding into or around the brain). This classification is the pivot on which acute stroke treatment turns: IV tPA — the clot-dissolving medication that can restore blood flow in ischemic stroke — is one of the most effective acute neurological treatments when given appropriately, but it dramatically worsens outcomes and increases mortality when given to a patient with hemorrhagic stroke, where its thrombolytic effect prevents the clotting that naturally limits bleeding. The opposite treatment for hemorrhagic stroke — aggressive blood pressure management and reversal of anticoagulation — would be harmful in ischemic stroke by reducing cerebral perfusion to the ischemic penumbra.
This is why brain CT scanning is performed within 10 to 15 minutes of hospital arrival for all suspected stroke patients — not primarily to confirm the stroke diagnosis (which can be made clinically), but to determine the stroke type and guide treatment. Understanding the differences between ischemic and hemorrhagic stroke — in mechanism, presentation, diagnosis, treatment, and prognosis — helps patients and families understand the acute management decisions they may face and the different recovery trajectories of the two conditions.
Ischemic Stroke — When Blood Flow Is Blocked
Ischemic stroke accounts for approximately 87 percent of all strokes and results from occlusion of a cerebral artery, preventing oxygen and glucose delivery to the brain territory the vessel supplies. The ischemic cascade described in dedicated stroke articles — failure of ion pumps, glutamate excitotoxicity, calcium influx, oxidative stress, and mitochondrial dysfunction — produces rapid neuronal death in the ischemic core (where flow is most severely reduced) and threatens the surrounding penumbra (where flow is reduced but neurons remain viable).
The major subtypes of ischemic stroke, classified by mechanism, have distinct causes, presentations, and secondary prevention approaches:
Large artery atherosclerosis accounts for approximately 20 to 25 percent of ischemic strokes. Atherosclerotic plaque in the cervical carotid or vertebral arteries, or in the intracranial large arteries (MCA, ICA, basilar), can cause stroke through two mechanisms: in situ thrombosis (clot forming on a ruptured plaque, acutely occluding the artery) or artery-to-artery embolism (plaque material or thrombus dislodging from the artery wall and traveling distally to occlude a more distal vessel). Large artery atherosclerotic strokes often produce cortical infarcts in the distribution of the affected vessel and may be preceded by TIA from the same mechanism. Carotid endarterectomy (surgical removal of carotid plaque) or stenting significantly reduces recurrent stroke risk in patients with symptomatic high-grade carotid stenosis (70 to 99 percent) — with benefit strongly time-dependent (greatest when performed within 2 weeks of the index stroke or TIA).
Cardioembolic stroke accounts for approximately 20 to 30 percent of ischemic strokes and results from emboli arising from cardiac sources — most commonly the left atrial appendage thrombus in atrial fibrillation, but also valvular vegetations in infective endocarditis, intracardiac thrombus in left ventricular aneurysm or cardiomyopathy, and paradoxical embolism through a patent foramen ovale (PFO). Cardioembolic strokes are typically large cortical infarcts reflecting the size of cardiac emboli and may involve multiple vascular territories simultaneously (suggesting a cardiac rather than vascular source). Anticoagulation is the mainstay of secondary prevention for most cardiac sources; PFO closure may benefit selected younger patients with cryptogenic stroke.
Small vessel occlusion (lacunar stroke) accounts for approximately 25 percent of ischemic strokes and results from occlusion of the small perforating arteries that supply the deep brain structures — basal ganglia, internal capsule, thalamus, brainstem, and periventricular white matter. Lacunar strokes are caused by lipohyalinosis (structural changes in small vessel walls from chronic hypertension) or microatheroma. They produce the classic “pure” lacunar syndromes — pure motor hemiparesis, pure sensory stroke, sensorimotor stroke, ataxic hemiparesis, clumsy hand-dysarthria — without cortical features and generally with better acute outcomes than cortical strokes, though multiple lacunar infarcts over years contribute substantially to vascular dementia.
Cryptogenic stroke — stroke of undetermined etiology after thorough evaluation — accounts for 25 to 30 percent of ischemic strokes. Many cryptogenic strokes represent undetected paroxysmal atrial fibrillation (detected by prolonged cardiac monitoring), patent foramen ovale-related paradoxical embolism, or subclinical large vessel atherosclerosis. ESUS (embolic stroke of undetermined source) — a subset of cryptogenic stroke with embolic features suggesting an undetected embolic source — is an active area of clinical research with ongoing trials evaluating anticoagulation versus antiplatelet therapy.
Hemorrhagic Stroke — When Blood Vessels Rupture
Hemorrhagic stroke accounts for 13 percent of strokes but a disproportionate 35 to 40 percent of stroke deaths, reflecting both the direct destruction of brain tissue by the hematoma and the secondary cascade of injury from blood toxicity, edema, and mass effect. There are two main types:
Intracerebral hemorrhage (ICH) — bleeding directly into the brain parenchyma — is the most common hemorrhagic stroke, representing 10 to 15 percent of all strokes. The most common cause is hypertensive small vessel disease: chronic hypertension causes lipohyalinosis and microaneurysm formation (Charcot-Bouchard microaneurysms) in the small perforating arteries, which can rupture under elevated blood pressure. Hypertensive ICH occurs most commonly in the basal ganglia (especially the putamen), thalamus, pons, and cerebellum — the territories supplied by the perforating arteries most vulnerable to hypertensive damage. Cerebral amyloid angiopathy (CAA) — in which amyloid protein deposits in cortical and leptomeningeal vessel walls — is the primary cause of lobar ICH (affecting the cortical and subcortical regions) in elderly patients, with characteristic “microbleeds” visible on gradient echo MRI sequences. Anticoagulant-related ICH (from warfarin or, less commonly, DOACs) is associated with larger initial hematoma volumes, more frequent hematoma expansion, and higher mortality than hypertensive ICH.
Subarachnoid hemorrhage (SAH) — bleeding into the subarachnoid space surrounding the brain — accounts for approximately 3 percent of all strokes but has particularly high mortality (30 to 40 percent of patients die within the first month) and high morbidity in survivors. The most common cause (approximately 85 percent) is rupture of an intracranial saccular (“berry”) aneurysm — a focal dilatation of a cerebral artery at branch points where hemodynamic stress is greatest, typically at the circle of Willis. SAH presents with the characteristic “thunderclap headache” — sudden onset, maximum intensity within seconds, often described as the worst headache of the patient’s life. The diagnostic and management priorities in SAH are different from ICH: securing the ruptured aneurysm (by surgical clipping or endovascular coiling) to prevent re-bleeding, managing vasospasm (a delayed complication at 4 to 14 days that causes delayed cerebral ischemia), and preventing hydrocephalus from impaired CSF circulation.
Treatment Differences — Why Stroke Type Determines Everything
The treatment approaches for ischemic and hemorrhagic stroke are not just different — they are in many respects opposite, which is why rapid CT-based classification is non-negotiable before any acute stroke treatment:
Ischemic stroke acute treatment: IV alteplase (tPA) within 4.5 hours of symptom onset; mechanical thrombectomy for large vessel occlusion within 24 hours in selected patients with favorable imaging; aggressive management of blood pressure only to prevent hypertensive emergency (otherwise, permissive hypertension in the first 24 to 48 hours maintains perfusion to the penumbra); antiplatelet or anticoagulant therapy based on stroke mechanism; intensive monitoring for cerebral edema and herniation in large hemispheric strokes.
Hemorrhagic stroke acute treatment: No tPA or anticoagulation (contraindicated); immediate reversal of anticoagulation (vitamin K, 4-factor PCC, or idarucizumab/andexanet alfa for DOAC reversal) in anticoagulant-related ICH; aggressive blood pressure lowering to target systolic below 140 mmHg (the INTERACT2 and ATACH-2 trials established blood pressure reduction as a safe strategy to limit hematoma expansion); neurosurgical evaluation for hematoma evacuation (particularly in cerebellar hemorrhage above 3 cm, where surgical evacuation is strongly preferred over medical management due to risk of herniation); ICP monitoring and management in patients with declining neurological status.
The American Stroke Association’s stroke types page provides comprehensive patient education on ischemic and hemorrhagic stroke. The CDC stroke types information explains the causes and differences between stroke categories. The NHLBI stroke types guide covers ischemic, hemorrhagic, and TIA with patient-friendly explanations of causes and treatment approaches.
Related reading: What Is a Stroke? | Stroke Warning Signs: FAST | Atrial Fibrillation | High Blood Pressure and Stroke | Coronary Artery Disease
Sources
- Powers WJ, et al. 2019 AHA/ASA Guideline for the Early Management of Patients With Acute Ischemic Stroke. Stroke. 2019;50(12):e344-e418.
- Hemphill JC, et al. 2015 AHA/ASA Guideline for the Management of Spontaneous Intracerebral Hemorrhage. Stroke. 2015;46(7):2032-2060.
- Connolly ES, et al. 2012 AHA/ASA Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage. Stroke. 2012;43(6):1711-1737.
- Molina CA, et al. Stroke Subtypes, Vascular Risk Factors, and Prognosis. Cerebrovasc Dis. 2006;22(1):2-7.
- Feigin VL, et al. Global and Regional Burden of Stroke 1990-2010. Lancet. 2014;383(9913):245-254.
Diagnosing Stroke Type — What Happens in the Emergency Department
When a patient with suspected stroke arrives at an emergency department, a precise sequence of evaluations occurs simultaneously — each aimed at answering the central question: ischemic or hemorrhagic? The answer determines everything about acute treatment.
Non-contrast CT head is performed within 10 to 15 minutes of arrival in most stroke-capable hospitals — this is the pivotal imaging study. It reliably identifies hemorrhagic stroke immediately: blood appears hyperdense (bright white) on CT, making ICH and SAH immediately visible. Ischemic stroke, however, is often CT-negative in the acute phase — the subtle early ischemic changes (loss of gray-white differentiation, sulcal effacement, hyperdense artery sign) may not be visible for several hours. This CT-negativity does not exclude ischemic stroke; it excludes hemorrhagic stroke, which is the primary purpose of the scan before tPA administration.
CT angiography (CTA) of the head and neck is performed in most patients to identify large vessel occlusion (LVO) — the subset of ischemic strokes where mechanical thrombectomy is indicated. CTA can be acquired in minutes after the non-contrast CT and provides the arterial anatomy needed to plan thrombectomy. It can also identify aneurysms in SAH patients and the source vessel in ICH (such as underlying arteriovenous malformation or tumor causing the hemorrhage).
MRI with DWI (diffusion-weighted imaging) is the most sensitive early imaging for ischemic stroke — DWI identifies ischemic tissue within minutes of stroke onset as an area of restricted diffusion (bright signal). MRI is preferred for posterior circulation strokes (where CT has limited sensitivity) and for identifying small lacunar infarcts. The DWI-FLAIR mismatch pattern (DWI positive, FLAIR negative) indicates a stroke likely within 4.5 hours, which has expanded the IV tPA treatment window for patients with unknown onset times (wake-up stroke).
Laboratory workup includes blood glucose (to exclude hypoglycemia as a stroke mimic and because both hypoglycemia and hyperglycemia worsen ischemic injury), coagulation studies (critical before tPA and for anticoagulant reversal in ICH), CBC, renal function, and a cardiac troponin (elevated in many stroke patients from sympathetic activation and predictive of cardiac complications). Cardiac monitoring (ECG, continuous telemetry) identifies paroxysmal atrial fibrillation as the source of cardioembolic stroke — a key secondary prevention finding.
Risk Factors — Overlapping Causes, Different Mechanisms
Ischemic and hemorrhagic stroke share many risk factors because both reflect vascular disease driven by the same underlying pathophysiology, but their relative contributions differ between the two stroke types:
Hypertension is the dominant modifiable risk factor for both ischemic and hemorrhagic stroke, but its mechanistic contribution is different. For ischemic stroke, hypertension accelerates atherosclerosis in large and medium cerebral arteries and causes the small vessel lipohyalinosis underlying lacunar infarcts. For hemorrhagic stroke (particularly ICH), hypertension directly damages small perforating arteries through lipohyalinosis and Charcot-Bouchard microaneurysm formation, creating vulnerable vessels prone to rupture. The lifetime risk of ICH is 5 to 6 times higher in patients with untreated hypertension than in normotensive patients — making blood pressure control the single most powerful intervention for ICH prevention. Achieving and maintaining blood pressure below 130/80 mmHg reduces the risk of both stroke types substantially.
Atrial fibrillation is a major risk factor for cardioembolic ischemic stroke but is not associated with hemorrhagic stroke in the absence of anticoagulation. However, anticoagulation therapy for AFib — which reduces ischemic stroke risk by 60 to 70 percent — carries a 0.3 to 0.5 percent annual risk of ICH when using DOACs (lower than warfarin’s 0.7 to 1.0 percent annual ICH risk). In patients with very high ICH risk (prior ICH, severe CAA on MRI), the anticoagulation decision for AFib requires individualized risk-benefit analysis.
Anticoagulant and antiplatelet therapy — while essential for preventing cardioembolic and atherosclerotic ischemic stroke — increases hemorrhagic stroke risk. Warfarin-related ICH has a particularly poor prognosis (mortality 50 to 60 percent) because warfarin produces larger initial hematoma volumes and more severe hematoma expansion than spontaneous hypertensive ICH. DOACs have significantly lower ICH risk than warfarin and have largely replaced warfarin for AFib-related stroke prevention. Dual antiplatelet therapy (aspirin plus clopidogrel) increases ICH risk compared to single antiplatelet therapy, which is why current guidelines recommend dual antiplatelet only for limited durations (21 to 90 days depending on the clinical scenario).
Cerebral amyloid angiopathy (CAA) is a risk factor specifically for lobar ICH in elderly patients — it does not increase ischemic stroke risk. CAA is caused by deposition of amyloid beta protein in cortical and leptomeningeal blood vessel walls, making them fragile and prone to rupture. CAA is the dominant cause of ICH in patients over 70 without hypertension and is characterized by microbleeds in cortical and subcortical regions visible on gradient echo or susceptibility-weighted MRI sequences. The presence of extensive CAA changes the risk-benefit calculation for anticoagulation and antiplatelet therapy substantially.
Prognosis and Recovery — How Outcomes Differ Between Stroke Types
Ischemic and hemorrhagic stroke have distinct short-term and long-term prognosis profiles that reflect their different injury mechanisms and treatment options:
Ischemic stroke short-term prognosis: 30-day mortality for ischemic stroke is approximately 8 to 15 percent overall, but varies enormously by stroke severity and treatment. Patients with large hemispheric infarction (malignant MCA infarction with midline shift and herniation) have 30-day mortality exceeding 80 percent without decompressive hemicraniectomy — a surgical procedure that removes part of the skull to relieve pressure, which the HAMLET, DESTINY, and DECIMAL trials established reduces mortality from 78 percent to 29 percent in selected patients under 60. Large basilar artery occlusion treated with thrombectomy has approximately 35 to 45 percent good functional outcome (mRS 0-2) in contemporary trials — a dramatic improvement over natural history (which approaches 80 to 90 percent mortality or severe disability).
Hemorrhagic stroke short-term prognosis: ICH has significantly higher acute mortality than ischemic stroke — 30-day mortality is approximately 35 to 50 percent for moderate to large ICH, with much of this early mortality occurring within the first 24 to 48 hours from hematoma expansion, herniation, and IVH-related hydrocephalus. The ICH Score (which incorporates age, GCS score, ICH volume, infratentorial location, and IVH presence) predicts 30-day mortality ranging from 0 percent (score 0-1) to 97 percent (score 5-6). SAH carries a 30-day mortality of approximately 35 to 40 percent, with re-bleeding (most common in the first 24 hours before aneurysm is secured) being the most feared early complication.
Long-term functional recovery: Among stroke survivors, ischemic stroke generally has better long-term functional outcomes than ICH of similar initial severity — approximately 50 percent of ischemic stroke survivors achieve functional independence (mRS 0-2) at 6 months, compared to approximately 20 percent of ICH survivors with moderate to large initial hematoma volumes. However, ICH survivors who survive beyond 30 days often have better cognitive preservation than ischemic stroke survivors with similar sized cortical infarcts, because ICH causes displacement and compression of brain tissue rather than direct infarction — some of this compressed tissue can recover function as the hematoma is resorbed.
Recurrence risk: Both stroke types carry significant recurrence risk. Ischemic stroke has approximately 10 to 15 percent 90-day recurrence risk if not treated with optimal secondary prevention — which is why urgent evaluation and prevention initiation is critical even for TIA (where the risk is highest, because brain infarction has not yet occurred). ICH recurrence risk is 2 to 3 percent annually, with higher risk in patients with hypertensive ICH who remain uncontrolled and in CAA patients who continue anticoagulation or antiplatelet therapy. The primary prevention of ICH recurrence is aggressive blood pressure control — targeting systolic below 130 mmHg has been shown in observational studies to reduce ICH recurrence by 50 to 70 percent compared to inadequate BP control.
Thrombectomy for Ischemic Stroke — The Treatment Revolution
Mechanical thrombectomy — catheter-based removal of the clot causing large vessel occlusion — represents the most significant advance in stroke treatment in recent decades and dramatically changed outcomes for patients with LVO ischemic stroke. The pivotal trials (MR CLEAN, ESCAPE, SWIFT PRIME, DAWN, DEFUSE 3) established that thrombectomy reduces severe disability or death in LVO stroke patients from approximately 75 percent to approximately 45 percent — an absolute risk reduction of 30 percentage points that translates to approximately 1 in 3 treated patients achieving a fundamentally better outcome.
The original thrombectomy window was 6 hours from symptom onset. The DAWN and DEFUSE 3 trials, both published in 2018, extended this window to 24 hours in selected patients using advanced CT perfusion or MRI-based selection criteria that identify patients with substantial salvageable penumbra — the “mismatch” between the volume of ischemic but viable tissue (the penumbra) and the already infarcted core. This imaging-based selection identifies patients whose slow progression from core to penumbra (because of good collateral vessels) means they retain treatment targets even hours after the vessel occluded.
The impact of thrombectomy eligibility on stroke system of care is substantial: patients with suspected large vessel occlusion are now triaged to thrombectomy-capable centers (comprehensive stroke centers) even when a closer primary stroke center can provide IV tPA, because the functional benefit of thrombectomy — which can only be done at comprehensive centers — outweighs the time cost of the additional transport. Mobile stroke units (ambulances equipped with CT scanners that allow prehospital IV tPA administration and identification of LVO patients for direct transport to comprehensive centers) have been deployed in major urban centers to further compress the time from symptom onset to reperfusion.
Hemorrhagic stroke has no equivalent to thrombectomy — the acute treatment remains primarily medical (blood pressure control, anticoagulation reversal, ICP management), with surgical intervention reserved for specific scenarios: cerebellar hemorrhage with hydrocephalus or mass effect (where surgical evacuation is strongly preferred), lobar ICH in deteriorating patients where surgical risk-benefit may favor evacuation, and ventricular drainage for IVH-related hydrocephalus. Several trials of minimally invasive hematoma evacuation (catheter-based aspiration with alteplase irrigation for IVH, and aspiration systems for ICH) are ongoing, with preliminary results suggesting benefit in selected patients — this remains an active area of investigation.