
When a doctor says cancer has spread, the word “metastatic” can feel like a door closing. For many patients and families, this diagnosis arrives carrying the weight of a worst-case outcome — a belief, often unspoken, that there is little left to do but wait. That fear is understandable. But the full picture of metastatic cancer is more complicated, and for many patients, more hopeful, than that fear allows.
The 5-year relative survival rate for distant-stage cancer — across all types — has more than doubled since the mid-1990s, rising from approximately 17% to 35% for diagnoses made between 2015 and 2021. (NCI SEER, 2024) Some patients with metastatic breast, prostate, or kidney cancer live for many years with well-managed disease. Modern immunotherapy has produced durable remissions in cancers once considered uniformly fatal within months. The story of metastatic cancer in 2026 is not a single story — it’s many.
This article explains what metastatic cancer is, how cancer cells travel to establish tumors in new locations, where they most commonly spread, what current survival data actually tells us, and what modern treatment can realistically accomplish.
What Is Metastatic Cancer?
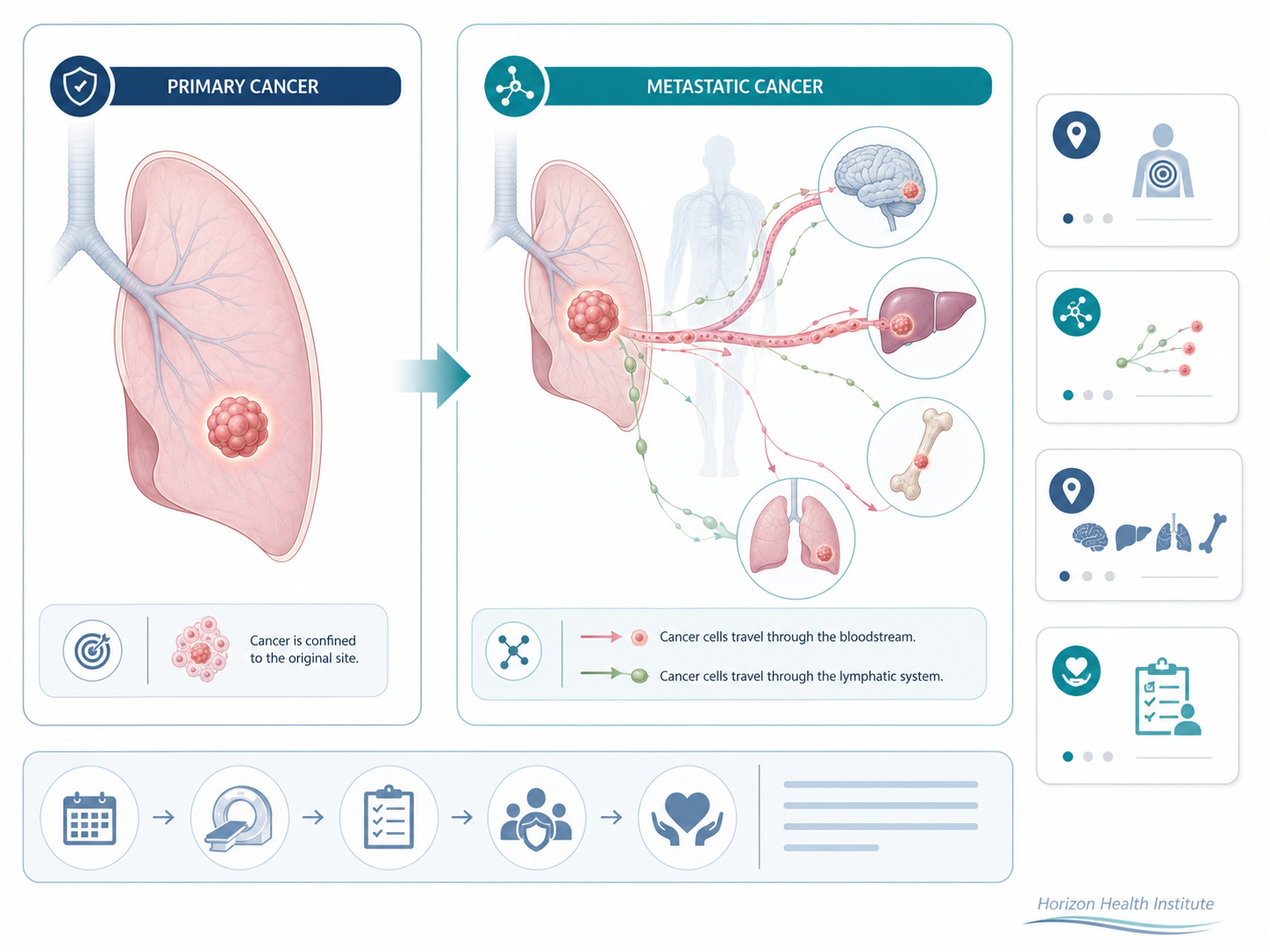
Metastatic cancer is cancer that has spread from its original site — the primary tumor — to one or more other parts of the body. The process is called metastasis, and the new tumors that form are called metastases or secondary tumors. A metastatic tumor always retains the identity of the original cancer: breast cancer that spreads to the liver is still called metastatic breast cancer, not liver cancer, because the cells remain breast cancer cells.
This distinction matters for treatment. Doctors treat metastatic cancer based on the biology of the original cancer cells, not the organ where metastases appear. A person with metastatic colorectal cancer that has spread to the lungs receives colorectal cancer treatment — not lung cancer treatment — because that’s what the tumor cells respond to.
Metastatic cancer is most often classified as Stage IV (or “stage 4 cancer”) in standard staging systems, though the exact designation varies by cancer type. You may also hear “advanced cancer,” “secondary cancer,” or “distant stage cancer” used to describe similar situations. These terms overlap; “metastatic” and “distant stage” are the most precise.
It is estimated that more than 90% of cancer-related deaths in the United States result from metastatic disease rather than from the original tumor. (NCI, 2023) This makes understanding and treating metastasis one of oncology’s central challenges — and one of the areas where the most progress has been made.
How Metastatic Cancer Spreads Through the Body
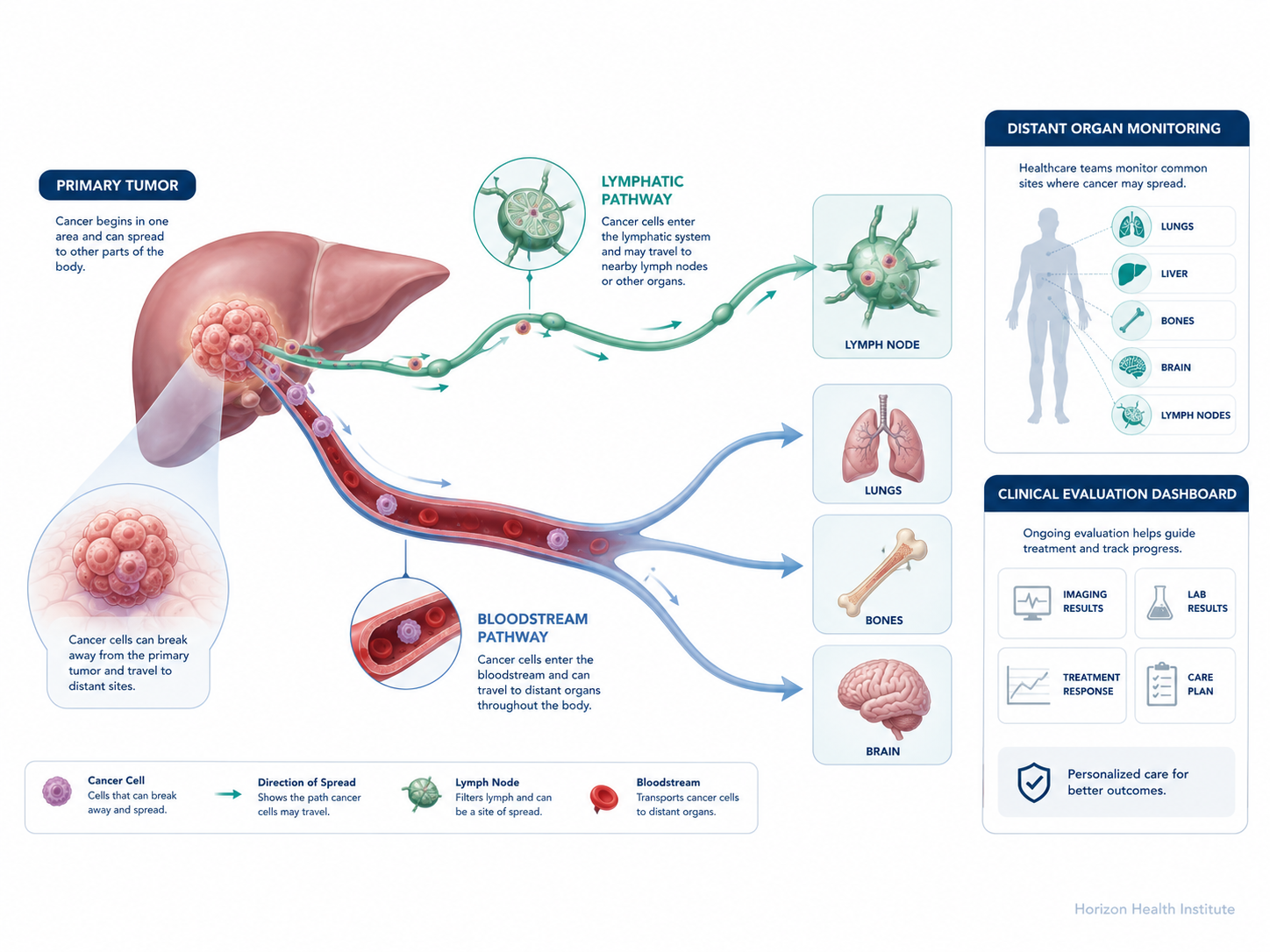
Cancer metastasis is not random. It follows a complex, multi-step biological process — and most cancer cells that break free from a primary tumor never successfully establish a new tumor. They are eliminated along the way. Understanding this process helps explain why certain cancers tend to spread to certain organs and why researchers are developing drugs that target specific steps in this cascade.
The metastatic cascade unfolds in stages:
- Local invasion — Cancer cells at the edge of the primary tumor develop the ability to break through the tissue that normally contains them.
- Intravasation — Cells enter the bloodstream or lymphatic vessels, gaining access to the rest of the body.
- Circulation — Most circulating cancer cells are destroyed by immune defenses or physical forces. A small fraction survive.
- Extravasation — Surviving cells exit the bloodstream and enter a new tissue.
- Colonization — Cells establish a blood supply and begin growing into a secondary tumor.
Cancer uses two primary transportation routes: the bloodstream (hematogenous spread) and the lymphatic system. Lymph nodes — small filtering glands distributed throughout the body — are frequently an early checkpoint. When cancer is found in nearby lymph nodes, it signals that cells have entered the lymphatic system and may be moving toward more distant locations. (NCI, 2022)
The old “seed and soil” theory — first proposed in the 1880s — still helps explain why different cancers favor different organs. Like seeds that need compatible soil to grow, cancer cells are more likely to establish themselves in certain environments. Breast cancer has particular affinity for bone, liver, lungs, and brain. Prostate cancer tends to spread to bone. Colorectal cancer frequently spreads to the liver because blood from the colon passes directly through the portal vein to the liver before returning to the heart.
Where Does Metastatic Cancer Most Commonly Spread?
Cancer can spread to almost any organ or tissue, but four locations account for the majority of metastases across cancer types: bone, liver, lungs, and brain. Each site produces its own pattern of symptoms — which is why knowing where cancer has spread is essential for planning treatment and supportive care.
| Primary Cancer | Most Common Metastasis Sites |
|---|---|
| Breast | Bone, liver, lung, brain |
| Lung | Brain, adrenal glands, bone, liver |
| Prostate | Bone (spine, pelvis) |
| Colorectal | Liver, lung, peritoneum |
| Melanoma | Lung, brain, liver, bone |
| Kidney | Lung, bone, liver, brain |
Bone Metastases
Bone is the most common metastasis site for breast and prostate cancers and is frequently involved in kidney, lung, and thyroid cancers as well. Cancer cells in bone disrupt normal remodeling, weakening structure and causing pain — typically a deep, aching discomfort that worsens at night or with activity. Bone metastases raise the risk of pathological fractures and can compress the spinal cord if they develop near the spine. Treatment usually includes radiation to shrink painful lesions, bone-strengthening drugs like bisphosphonates (zoledronic acid) or denosumab, and sometimes surgery to stabilize affected bones.
Liver Metastases
The liver receives a large share of the body’s blood supply, making it a common destination for colorectal, breast, lung, stomach, and pancreatic cancer cells. Early liver metastases often produce no symptoms. As they grow, they may cause right-side abdominal discomfort, fatigue, weight loss, and — in advanced cases — jaundice (yellowing of the skin and eyes) when bile ducts become compressed. Treatment options range from systemic therapy to ablation techniques and, in select patients with limited liver involvement, surgical removal.
Lung Metastases
The lungs filter the body’s entire blood supply through pulmonary circulation, making them a frequent target for colorectal, breast, kidney, and bone cancers. Small lung metastases often go unnoticed — discovered on a chest CT ordered for another reason. When symptomatic, they may cause a persistent cough, shortness of breath, chest discomfort, or coughing up blood. In patients with a small number of lung metastases, surgical removal (pulmonary metastasectomy) may offer meaningful long-term disease control.
Brain Metastases
Brain metastases are most common in lung, breast, melanoma, kidney, and colorectal cancers. The blood-brain barrier — a protective filter — creates a sanctuary where some cancer cells can escape treatment. Symptoms depend on location: headaches (especially in the morning), vision or speech changes, weakness or numbness on one side, memory problems, or seizures. Treatment options include stereotactic radiosurgery (Gamma Knife, CyberKnife), whole-brain radiation, surgery for accessible lesions, and newer targeted drugs specifically designed to cross the blood-brain barrier.
Metastatic Cancer Survival Rates: What the Numbers Really Show
Survival statistics for metastatic cancer are among the most searched — and most misunderstood — health numbers on the internet. Understanding what they actually mean matters as much as knowing the numbers themselves.
The 5-year relative survival rate for distant-stage cancer across all types was 35% for diagnoses made between 2015 and 2021 — more than double the rate of approximately 17% from the mid-1990s. (NCI SEER, 2024) This reflects three decades of advances in targeted therapy, immunotherapy, and treatment protocols.
Survival rates vary substantially by cancer type:
| Cancer Type | 5-Year Relative Survival Rate (Distant Stage) |
|---|---|
| Thyroid | ~65% |
| Prostate | ~36.6% |
| Breast | ~29% |
| Cervical | ~18% |
| Kidney | ~16.9% |
| Colorectal | ~14.3% |
| Lung | ~8% |
| Pancreatic | ~3.1% |
Source: NCI SEER, 2023
Statistics describe populations, not individuals. A 35% 5-year survival rate means 35 out of 100 people in a given group lived 5 or more years — it does not mean any one person has a 35% chance of surviving. Individual prognosis depends on cancer type, molecular subtype, treatment received, overall health, and many other factors. Also, these figures are based on diagnoses made 5+ years ago — before the most recent treatments became available. Patients diagnosed today will likely benefit from therapies not yet reflected in current statistics.
For some metastatic cancers — particularly breast and prostate — oncologists now routinely speak of treating the disease as a chronic condition, much like diabetes or heart disease. Patients may live 5, 10, or more years with ongoing treatment keeping the cancer controlled. Approximately 170,000 women in the United States are living with metastatic breast cancer right now. (Susan G. Komen, 2025)
When cancer has spread to only a small number of sites — typically 1 to 5 — it may be classified as oligometastatic cancer. In carefully selected patients, aggressively treating all known metastatic sites with surgery or stereotactic radiation — with curative intent — has produced long-term disease control and in some cases apparent cure, particularly in colorectal cancer with isolated liver metastases. (NCI, 2020)
How Metastatic Cancer Is Treated
The goals of treating metastatic cancer differ from the goals of treating early-stage disease. For most metastatic cancers, the primary aim is disease control — slowing or stopping tumor growth, managing symptoms, preserving quality of life, and extending life for as long as possible. This is not giving up. For millions of people, this approach means years of meaningful, active life.
Systemic Therapies
Chemotherapy uses drugs that kill rapidly dividing cells. It remains effective for many cancer types and is often used alongside newer treatments.
Targeted therapy uses drugs that block specific molecular changes cancer cells depend on to grow. These drugs work only in tumors that carry the relevant genetic alteration — which is why molecular testing (biomarker testing or genomic profiling) of the tumor is now standard practice for most newly diagnosed metastatic cancers. HER2-targeted drugs for HER2-positive breast cancer, ALK inhibitors for ALK-positive lung cancer, and BRAF inhibitors for BRAF-mutant melanoma are examples of targeted therapy transforming outcomes.
Immunotherapy — particularly checkpoint inhibitors — removes molecular “brakes” that cancer cells use to hide from immune attack, allowing the immune system to recognize and destroy them. This approach has dramatically improved outcomes in metastatic melanoma, lung, kidney, and bladder cancers, with some patients achieving sustained remissions lasting years. (ACS, 2025)
Antibody-drug conjugates (ADCs) link chemotherapy drugs directly to antibodies that target cancer cells, delivering treatment precisely to tumors while sparing more healthy tissue. Several ADCs have received FDA approval for metastatic breast, lung, and bladder cancers in recent years.
Hormone therapy blocks or lowers hormones that drive tumor growth in estrogen-positive breast cancer and testosterone-driven prostate cancer, and can control disease for extended periods.
Local Therapies for Metastases
- Radiation therapy to relieve pain from bone metastases, treat brain metastases, or address oligometastatic sites with curative intent
- Stereotactic radiosurgery (Gamma Knife, CyberKnife) — highly precise, non-invasive radiation for brain metastases or limited sites of disease
- Surgery to remove an isolated metastasis, prevent a fracture, or relieve obstruction
- Ablation (radiofrequency ablation, cryoablation) to destroy liver or lung metastases without surgery in selected patients
Palliative and Supportive Care
Palliative care is specialized support focused on relieving symptoms and improving quality of life — and it should begin at diagnosis, running alongside disease-controlling treatment from day one. Research published in the New England Journal of Medicine shows that patients who receive early palliative care alongside cancer treatment report better quality of life and, in some studies, live longer than those who receive cancer treatment alone. A palliative care team addresses pain, fatigue, nausea, anxiety, depression, nutritional challenges, and practical needs.
For newly diagnosed metastatic patients, clinical trials deserve serious consideration. Trials provide access to treatments not yet available outside of research — including the very immunotherapy and targeted therapy breakthroughs that are now standard care because of trials conducted a decade ago. Ask your oncologist specifically about trial eligibility at your first appointment.
Can Metastatic Cancer Go Into Remission?
Yes — though the likelihood and durability of remission depend heavily on cancer type and available treatments.
Partial remission means the cancer has shrunk significantly but remains detectable. Complete remission (complete response) means no cancer can be found by standard imaging or blood tests. Durable remission means that complete response has persisted for months or years. In certain metastatic cancers treated with immunotherapy, durable remissions persist even after treatment has stopped.
Before checkpoint inhibitor immunotherapy arrived, median survival for metastatic melanoma was roughly 9 months. Today, approximately 20–30% of patients treated with combination immunotherapy achieve long-term disease control, and some oncologists now use the word “cured” for patients who remain disease-free 5 or more years after completing treatment. In ALK-positive metastatic lung cancer, patients on newer ALK inhibitors like lorlatinib are achieving median progression-free survival exceeding 5 years in clinical trials.
For many other metastatic cancers, the realistic and meaningful goal is stable disease — cancer that is present but not growing. Many patients maintain stable disease for years, living full and active lives, cycling through effective treatments as their cancer evolves. When an oncologist says “we can control this,” that statement carries real weight in 2026. It reflects genuine scientific progress, not wishful thinking.
Questions to Ask Your Oncologist About Metastatic Cancer
Arriving at your first oncology appointment with a written list of questions is one of the most practical things a newly diagnosed patient can do. Here is a checklist based on guidance from leading cancer centers:
About your diagnosis:
About treatment:
About monitoring & support:
Getting a second opinion at a major cancer center or an NCI-designated cancer center is always appropriate after a new metastatic diagnosis — and most oncologists welcome it. Bring someone you trust to every appointment. Take notes, or ask permission to record the conversation. The additional perspective may confirm your treatment plan or open doors to different options, including clinical trials.
Frequently Asked Questions
In most standard staging systems, yes — Stage IV is the designation given when cancer has spread to distant organs or tissues, which is the definition of metastatic. However, staging systems vary by cancer type, and oligometastatic disease increasingly occupies a clinical gray zone where some specialists treat limited spread with curative intent regardless of formal stage classification.
Speed varies enormously. Aggressive cancers — such as triple-negative breast cancer or small cell lung cancer — can develop new metastases in weeks. Others — certain hormone receptor-positive breast cancers or low-grade prostate cancers — may remain stable for months or years. Growth rate depends on cancer type, molecular subtype, and individual biology. Effective treatment can significantly slow or halt progression.
Symptoms depend on where cancer has spread. Bone metastases cause deep, aching pain that worsens at night. Liver metastases may cause fatigue, abdominal fullness, and eventually jaundice. Lung metastases produce a persistent cough or shortness of breath. Brain metastases cause headaches, vision or speech changes, weakness, or confusion. Many small metastases cause no symptoms at all and are found on routine surveillance imaging.
For most metastatic cancers, cure is not the standard goal — but it is not impossible. Certain metastatic cancers, including testicular cancer and some lymphomas, have high cure rates. Oligometastatic disease treated aggressively has produced apparent cures in selected patients. Immunotherapy has produced durable, possibly permanent remissions in subsets of patients with metastatic melanoma and lung cancer. For most patients, long-term disease control — living well for years — is the realistic and achievable aim.
Recurrent cancer is cancer that returns after treatment. A local recurrence happens at the original tumor site. Regional recurrence involves nearby lymph nodes. When cancer returns in a distant organ — the liver, lungs, bones, or brain — it becomes metastatic. Some patients experience a local recurrence first, which is treated, and then later develop distant metastases. Others have their first recurrence as metastatic disease without any prior local return.
A metastatic cancer diagnosis is serious. But it is not one story — it’s many, shaped by cancer type, molecular biology, available treatment, and the patient as an individual. Survival rates have more than doubled in a generation. New treatment classes are producing remissions once considered impossible. Some patients live for years with well-managed metastatic disease, describing it as a chronic condition they live with.
Work with an oncology team experienced in your cancer type. Ask about molecular testing of your tumor. Ask about clinical trials. Consider a second opinion at an NCI-designated cancer center. Ask for palliative care support from the beginning — not as giving up, but as a way to live as well as possible throughout treatment. Understanding your diagnosis clearly is the first step. The next is finding the best team to navigate it with you.
The content on Horizon Health Guide is intended for informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the guidance of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website. If you think you may have a medical emergency, call your doctor, go to the emergency department, or call 911 immediately.
References
- National Cancer Institute. Metastatic Cancer: When Cancer Spreads. cancer.gov/types/metastatic-cancer. Accessed June 2026.
- NCI SEER Program. Cancer Stat Facts: Cancer of Any Site. seer.cancer.gov/statfacts/html/all.html. Accessed June 2026.
- American Cancer Society. Advanced and Metastatic Cancer; Cancer Facts & Figures 2025. cancer.org. Accessed June 2026.
- Cleveland Clinic. Metastasis (Metastatic Cancer): Symptoms & Treatment. clevelandclinic.org. Accessed June 2026.
- Mayo Clinic. Stage 4 (Metastatic) Colon Cancer. mayoclinic.org. Accessed June 2026.
- Susan G. Komen. Metastatic Breast Cancer Facts and Statistics. komen.org. 2025.
- Siegel RL, et al. Cancer Statistics, 2025. CA: A Cancer Journal for Clinicians. 2025.
- Lam et al. Future Trends in Incidence and Long-Term Survival of Metastatic Cancer in the United States. Communications Medicine / Nature. 2023.
- National Cancer Institute. Cancer in Lymph Nodes May Help Tumors Metastasize. cancer.gov. 2022.
- National Cancer Institute. Oligometastatic Cancer — A More Treatable Kind. cancer.gov. 2020.