Difficulty swallowing — the medical term is dysphagia — is a common symptom that most adults experience occasionally. Roughly 1 in 10 people report it at some point, and the vast majority of cases are benign: a minor infection, acid reflux, or food going down too quickly.
But there is a pattern of dysphagia that is not benign — and that pattern is one of medicine’s most important alarm signs. It begins with difficulty swallowing solid foods. Steak first, then denser breads, then soft foods. Over weeks to months, it progresses — eventually to liquids, and in advanced cases, to difficulty swallowing saliva. The progression itself, the fact that it keeps getting worse, is the signal that demands attention.
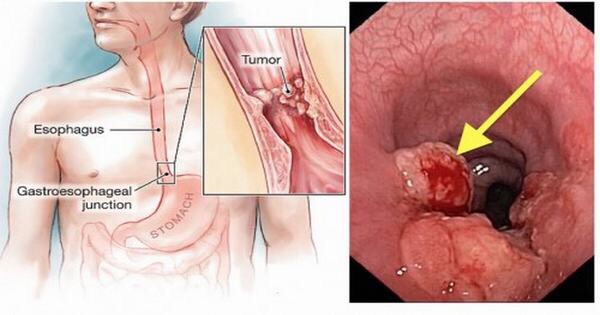
This is the classic presentation of esophageal cancer — one of the most lethal malignancies we know, not because it is untreatable, but because it is almost never caught early. When diagnosed at Stage I, the 5-year survival rate is approximately 47%. When diagnosed with distant metastasis, it falls to around 3%.

Two Types of Dysphagia: Esophageal vs. Oropharyngeal
The first useful distinction is anatomical: where does the difficulty occur?
Oropharyngeal dysphagia means difficulty initiating the act of swallowing — food or liquid sticks at the throat level. This is most commonly associated with neurological diseases (stroke, Parkinson’s, ALS) but also occurs with cancers of the oropharynx, hypopharynx, and larynx.
Esophageal dysphagia means swallowing initiates normally, but food sticks in the chest. This is the type most directly associated with esophageal cancer, peptic strictures, and motility disorders.
The practical self-assessment question: Does the food feel stuck in your throat before you can swallow? Or does it go down and then stop somewhere in your chest?
This distinction matters because it points to different anatomical locations — and different cancers. Throat-level difficulty with hoarseness or a neck mass raises concern for head and neck cancer. Mid-chest food sticking that progressively worsens raises concern for esophageal cancer.
The Classic Cancer Pattern: Progressive Dysphagia
The most important feature of malignancy-associated dysphagia is not severity — it is progression.
A growing esophageal tumor narrows the esophageal lumen progressively. The sequence follows a predictable path:
| Stage | What Becomes Difficult |
|---|---|
| Early | Tough meat, dry bread |
| Intermediate | Soft foods — pasta, cooked vegetables |
| Advanced | All solid food |
| Late | Liquids and own saliva |
Most benign causes of dysphagia have a different temporal pattern:
- Schatzki ring: Episodic dysphagia only with large solid boluses; not progressive
- Eosinophilic esophagitis (EoE): Intermittent; food impaction episodes that come and go for years
- GERD stricture: Stable or very slowly worsening over years
- Achalasia: Both solids AND liquids cause difficulty from onset — the reverse of early cancer
The key word is progressive. Any dysphagia that keeps worsening from week to week requires endoscopic evaluation.
Cancers That Cause Difficulty Swallowing
Esophageal Cancer
The malignancy most directly associated with dysphagia. Approximately 22,370 Americans are diagnosed each year; approximately 16,130 die. The overall 5-year survival is roughly 21% — primarily because most patients present at an advanced stage.
Esophageal cancer has two histologically distinct subtypes:
- Squamous cell carcinoma (SCC): Upper and middle esophagus. Risk factors: tobacco (~5×), heavy alcohol (~5×; combined with tobacco: 30–40× increased risk), hot beverages above 65°C (IARC Group 2A carcinogen).
- Adenocarcinoma (AC): Lower esophagus and gastroesophageal junction. Driven by GERD, Barrett’s esophagus, and obesity. Seven to eight times more common in men. The dominant type in Western countries.
Head and Neck Cancers
Cancers of the oropharynx, hypopharynx, and larynx cause oropharyngeal dysphagia. A combination of dysphagia + hoarseness is a particularly concerning symptom cluster — suggesting recurrent laryngeal nerve involvement. HPV-associated oropharyngeal cancer has risen sharply in incidence, predominantly affecting middle-aged men without significant tobacco or alcohol history.
Lung Cancer
Lung tumors in the right lung or mediastinum can compress the esophagus externally. Mediastinal disease compressing the left recurrent laryngeal nerve produces hoarseness plus dysphagia — a combination that always warrants chest imaging.
Thyroid Cancer, GEJ Cancer, and Lymphoma
Invasive thyroid cancer can compress or invade the esophagus posteriorly. Adenocarcinoma of the gastroesophageal junction behaves like lower esophageal adenocarcinoma, causing progressive dysphagia. Mediastinal lymphoma compresses the esophagus externally and is typically accompanied by B symptoms — fever, night sweats, weight loss.
Barrett’s Esophagus: How GERD Becomes Cancer
Barrett’s esophagus is the critical link between chronic acid reflux and esophageal adenocarcinoma.
Normally, the lower esophagus is lined with squamous epithelium. When chronically bathed in acid and bile from GERD, these cells are gradually replaced by intestinal-type columnar cells — intestinal metaplasia. This transformation is Barrett’s esophagus.
Approximately 5.6% of adults who undergo upper endoscopy in the US have Barrett’s esophagus — more common in obese white males with long-standing symptomatic GERD, but possible in anyone with chronic reflux.
| Barrett’s Stage | Annual Cancer Risk | Recommended Action |
|---|---|---|
| Non-dysplastic | 0.1–0.3% per year | EGD every 3–5 years |
| Low-grade dysplasia | 0.5–1% per year | EGD every 6–12 months or endoscopic ablation |
| High-grade dysplasia | 6–19% per year | Immediate endoscopic eradication therapy |
Non-dysplastic Barrett’s represents a 30–125× increased lifetime risk of adenocarcinoma vs. the general population. Radiofrequency ablation (RFA) eliminates Barrett’s epithelium in over 80% of patients — one of the clearest examples of successful cancer interception in clinical medicine.
Risk Factors for Esophageal Cancer
Squamous Cell Carcinoma
- Tobacco smoking: ~5× increased risk
- Heavy alcohol: ~5× increased risk; combined with tobacco: 30–40× increased risk
- Hot beverages above 65°C (149°F): IARC Group 2A (probable human carcinogen) for SCC — allow drinks to cool before consuming
- Achalasia and Plummer-Vinson syndrome
Adenocarcinoma
- Symptomatic GERD: 5–7× increased risk even without Barrett’s
- Barrett’s esophagus: 30–125× increased risk — the dominant precursor lesion
- Obesity (BMI >35): ~4× increased risk, independent of reflux
- Male sex: 7–8× more common than in women
- Smoking: associated with adenocarcinoma, though less strongly than with SCC
Alarm Symptoms: When Evaluation Cannot Wait
- Progressive dysphagia — especially solids becoming difficult before liquids
- Unintentional weight loss ≥5% of body weight in 6 months or less
- Hematemesis (vomiting blood) or melena (black tarry stool)
- Odynophagia — painful swallowing that is new or progressively worsening
- New iron-deficiency anemia in a man or postmenopausal woman
- Persistent unexplained vomiting
- Any dysphagia in patients with known Barrett’s, prior head/neck radiation, or achalasia
- Dysphagia + hoarseness: recurrent laryngeal nerve involvement; evaluate esophagus AND chest
- Dysphagia + palpable neck nodes: head/neck malignancy or mediastinal disease
- Dysphagia + weight loss + night sweats + fever: lymphoma or advanced esophageal cancer
The Diagnostic Pathway: What to Expect
Upper endoscopy (EGD) is the gold standard. Under sedation, a flexible camera passes through the mouth into the esophagus, stomach, and duodenum. The entire mucosal surface is visualized and any suspicious area is biopsied. Barrett’s surveillance uses the Seattle protocol: four-quadrant biopsies every 2 centimeters throughout the Barrett’s segment.
Barium esophagram is a real-time X-ray study as the patient swallows barium contrast — useful for identifying strictures, webs, extrinsic compression, and motility disorders. The “bird-beak” appearance is pathognomonic for achalasia.
CT chest/abdomen/pelvis stages confirmed cancer. PET-CT adds metabolic imaging for detecting distant disease. Endoscopic ultrasound (EUS) provides the most accurate T staging and N staging, directly determining surgical eligibility and the need for neoadjuvant therapy.
Treatment: A Stage-Appropriate Overview
Very early (T1a): Endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD) — curative without surgery. Preserves esophageal anatomy and function.
Stage I–III (resectable): Neoadjuvant carboplatin + paclitaxel + radiation (CROSS protocol) followed by esophagectomy. The CheckMate 577 trial demonstrated adjuvant nivolumab after neoadjuvant CRT doubled disease-free survival in patients with residual pathological disease — a landmark result now standard of care.
Advanced/metastatic: First-line pembrolizumab or nivolumab combined with platinum-based chemotherapy. HER2-positive adenocarcinoma (~20% of cases) adds trastuzumab based on the ToGA trial.
Barrett’s with high-grade dysplasia: Radiofrequency ablation (RFA) eliminates Barrett’s epithelium in >80% of patients. Combined with EMR for visible nodular dysplasia, this is highly effective cancer prevention.
Benign Causes: When Dysphagia Is Not Cancer
Most dysphagia is not cancer. Understanding the benign differential provides important context:
- GERD with peptic stricture: Acid-induced scarring of the lower esophagus. Typically stable or very slowly worsening over years; responds to dilation and PPI therapy.
- Achalasia: LES failure to relax. Defining feature: both solids AND liquids cause difficulty from onset — the reverse of early esophageal cancer.
- Eosinophilic esophagitis (EoE): Allergic inflammation; common in young men; episodic food impaction over years — intermittent, not progressive.
- Schatzki ring: Mucosal ring at the GEJ causing episodic dysphagia with large boluses. Intermittent and food-size-specific.
- Zenker’s diverticulum: Pharyngeal pouch trapping food, regurgitated hours later. Elderly patients. Not malignant.
The pattern that distinguishes cancer from all these benign causes: relentless, week-by-week progression. Symptoms that come and go, or that have been the same for years, are far more likely benign.
Frequently Asked Questions
Is it normal for food to occasionally get stuck?
Occasional mild difficulty — with a particularly dense or dry piece of food, or when eating too quickly — is common and usually benign. What is not normal is difficulty with foods you could previously eat without any problem, or any symptom that keeps progressively worsening over weeks.
I’ve had acid reflux for years — do I need an endoscopy?
Endoscopy is recommended for patients with chronic GERD symptoms who are over 50 — especially white males with other risk factors — to screen for Barrett’s esophagus. If you have any dysphagia in addition to reflux, endoscopy is warranted regardless of age to exclude a peptic stricture or early cancer.
Does acid reflux directly cause esophageal cancer?
Not directly — GERD increases cancer risk through the Barrett’s esophagus pathway. Most people with GERD never develop Barrett’s. Most people with Barrett’s never develop cancer. But the cumulative risk is significantly elevated, which is why surveillance endoscopy matters for appropriate patients.
How long does it take for Barrett’s esophagus to become cancer?
Progression is slow in most patients — non-dysplastic Barrett’s advances at about 0.1–0.3% per year, meaning it typically takes decades if it ever progresses. High-grade dysplasia progresses much faster (6–19% per year), which is why it requires immediate treatment when found.
Can esophageal cancer be caught early?
Yes — but almost exclusively through surveillance endoscopy in high-risk patients. Early esophageal cancers (T1a lesions) cause no symptoms and are found incidentally during Barrett’s surveillance. A cancer caught at T1a can be cured endoscopically. A cancer found because the patient develops progressive dysphagia is almost certainly Stage II or beyond.
What is the difference between dysphagia and odynophagia?
Dysphagia means difficulty swallowing — food or liquid doesn’t pass easily. Odynophagia means painful swallowing — the act causes a burning or stabbing sensation. Both can occur together in esophageal cancer, and both are alarm symptoms that warrant prompt evaluation, especially when new or progressive.
The Bottom Line
Dysphagia that keeps getting worse — tracking a clear progression from solid foods to soft foods to liquids over weeks to months — is one of the most important alarm symptoms in medicine. It is the defining presentation of esophageal cancer, one of the most lethal and late-diagnosed malignancies we know.
Esophageal cancer kills approximately 16,000 Americans per year, not because it is untreatable when found early, but because it is almost never found early. By the time progressive dysphagia develops, most tumors are Stage II or beyond.
If your swallowing has been getting progressively worse — talk to a doctor. Ask about upper endoscopy. If you have chronic GERD and fit the Barrett’s screening criteria, discuss it. The conversation takes minutes. For esophageal cancer, early detection is not just better — it is the difference between cure and palliative care.
This article is for educational purposes only and does not constitute medical advice. Progressive difficulty swallowing is an alarm symptom requiring evaluation by a physician or gastroenterologist. Do not delay seeking medical care based on information in this article.
- American Cancer Society. Cancer Facts & Figures 2024.
- NCCN Guidelines: Esophageal and EGJ Cancers. Version 3.2024.
- Shaheen NJ, et al. ACG Clinical Guideline: Barrett’s Esophagus. Am J Gastroenterol. 2022.
- Lagergren J, Smyth EC, et al. Oesophageal cancer. Lancet. 2017.
- Van Hagen P, et al. (CROSS trial). Preoperative chemoradiotherapy for esophageal cancer. NEJM. 2012.
- Kato K, et al. (CheckMate 577). Nivolumab as adjuvant therapy after resection. NEJM. 2021.
- Bang YJ, et al. (ToGA). Trastuzumab in HER2-positive gastric cancer. Lancet. 2010.
- IARC Monographs Volume 116. Drinking very hot beverages. 2016.