What Does an Abnormal Pap Smear Mean?
Receiving a notification that your Pap smear result is abnormal can be alarming — but in the vast majority of cases, an abnormal Pap smear does not mean that you have cancer. What it means is that some cells in your cervical sample appeared different from normal under microscopic examination, and that further evaluation is recommended to determine the significance of this finding. Approximately 3.5 million women in the United States receive an abnormal Pap smear result each year. Most of these results reflect minor cellular changes caused by a transient HPV infection, and many resolve without any treatment. Even the more concerning results — those suggesting moderate to severe pre-cancerous changes — represent pre-cancerous conditions that can be treated successfully, not established cancer.
Understanding the terminology used to report Pap smear results — and what each category means for your follow-up care — is the most important step in responding constructively to an abnormal result. The Bethesda System, the standardized terminology used for reporting cervical cytology in the United States and internationally, provides a structured framework that allows clinicians and patients to communicate about cervical findings consistently. Knowing what “ASC-US” or “HSIL” means, and what the recommended next step is for your specific result, transforms an abstract and anxiety-producing letter into actionable clinical information.
Abnormal Pap smear ≠ cervical cancer. The purpose of the Pap smear is to find cervical cell changes before cancer develops. An abnormal result means the screening is working — it has identified something that needs evaluation, not necessarily treatment. Most abnormal Pap smears are caused by HPV infections that produce minor cellular changes; these often clear on their own. Even HSIL (high-grade squamous intraepithelial lesion), the most concerning non-cancer Pap result, describes pre-cancerous changes that are highly treatable when caught at this stage.
The Bethesda System: How Pap Smear Results Are Reported
Pap smear results in the United States are reported using the Bethesda System (TBS), a standardized terminology first developed in 1988 at a National Cancer Institute conference in Bethesda, Maryland, and subsequently updated in 2001 and 2014. The Bethesda System ensures that clinicians across the country receive Pap smear reports using consistent terminology that clearly communicates the type and degree of any cellular abnormality found.
NILM — Negative for Intraepithelial Lesion or Malignancy
NILM is the normal Pap smear result. It means no pre-cancerous or cancerous cells were identified in the sample. NILM does not mean HPV-negative — a woman can have an HPV infection and still receive a NILM Pap result if the infection has not yet caused visible cellular changes. NILM simply means the Pap smear found no abnormal cells. The recommended next step is to continue routine screening at the appropriate interval for your age and screening approach (3 years for Pap alone, 5 years for co-testing or primary HPV testing).
Unsatisfactory/Inadequate Sample
An unsatisfactory result means the sample did not contain enough well-preserved cervical cells to be analyzed reliably. This is not an abnormal result — it provides no information about whether abnormal cells are or are not present. The Pap smear must be repeated, usually in 2–4 months. Common causes include insufficient cells on the sample, heavy inflammation or blood obscuring cells, air-drying artifact (less common with liquid-based cytology), or inadequate transformation zone sampling.
ASC-US — Atypical Squamous Cells of Undetermined Significance
ASC-US is the most common abnormal Pap smear result, accounting for approximately 40–50% of all abnormal cervical cytology findings. Squamous cells from the cervix show minor abnormalities that are more than could be attributed to normal variation, but not definitively characteristic of a specific lesion. ASC-US can represent: early HPV cytopathic effect, low-grade pre-cancerous change, reactive changes from inflammation or infection, hormonal effects (particularly in perimenopausal and postmenopausal women), or technical artifact.
Because ASC-US represents a borderline finding, the standard management approach is HPV reflex testing — testing the same liquid-based cytology specimen for high-risk HPV DNA. This reflex test is typically performed by the laboratory automatically when an ASC-US result is found:
- If HPV reflex testing is negative: the abnormal cells were unlikely caused by oncogenic HPV; return to routine screening (no colposcopy needed).
- If HPV reflex testing is positive: the abnormal cells may reflect an HPV-related change; colposcopy is recommended.
ASC-H — Atypical Squamous Cells, Cannot Exclude High-Grade SIL
ASC-H describes squamous cells with atypia that have features raising concern for a high-grade lesion, even though the full diagnostic criteria for HSIL are not met. ASC-H results carry a higher probability of finding CIN 2 or CIN 3 on subsequent colposcopy and biopsy than ASC-US. Colposcopy is recommended regardless of HPV status — a negative HPV test does not adequately reassure in this setting.
LSIL — Low-Grade Squamous Intraepithelial Lesion
LSIL describes cellular changes consistent with mild cervical dysplasia (CIN 1) or direct HPV cytopathic effect (koilocytosis — the characteristic appearance of cells productively infected with HPV). LSIL is strongly associated with active HPV infection, and most LSIL findings reflect a current or very recent HPV infection rather than a lesion that will necessarily progress to cancer.
Most LSIL resolves spontaneously, particularly in younger women. For women ages 25 and older, colposcopy or a repeat co-test in 1 year is recommended. For women ages 21–24, observation (repeat co-testing at 1 year) is preferred over immediate colposcopy because LSIL in this age group has an extremely high rate of spontaneous resolution and colposcopy with potential treatment could cause unnecessary cervical changes in young women who may not yet have completed their families.
HSIL — High-Grade Squamous Intraepithelial Lesion
HSIL describes cellular changes consistent with moderate to severe cervical dysplasia (CIN 2 or CIN 3). HSIL is the most significant abnormal squamous cell Pap smear result and carries the highest probability of finding true high-grade cervical pre-cancer on colposcopy and biopsy. Colposcopy with directed biopsy is required for all women with HSIL results. Some guidelines allow for expedited treatment — direct LEEP without waiting for biopsy confirmation first — in non-pregnant women with HSIL who are deemed high-risk for underlying CIN 3.
AGC — Atypical Glandular Cells
AGC describes glandular cells (endocervical or endometrial in origin) that appear abnormal. Glandular cell abnormalities are less common than squamous cell abnormalities on Pap smears and require a more comprehensive evaluation because they can reflect pre-cancerous conditions of either the endocervix (cervical canal) or the endometrium (uterine lining). Management includes colposcopy with endocervical sampling for all women, and endometrial biopsy for women aged 35 or older or any woman with abnormal uterine bleeding.
The ASCCP 2019 Risk-Based Management Guidelines
Before 2019, Pap smear abnormality categories were managed according to fixed algorithms — a given Pap result triggered a specific management step regardless of the individual’s history. The ASCCP 2019 Risk-Based Management Consensus Guidelines introduced a paradigm shift: management is now based on an individual’s estimated 5-year risk of having CIN 3 or cervical cancer, calculated from both the current test result and the individual’s prior screening history. This personalized approach means that:
- Two women with the same current Pap result may have different recommended management if their prior histories differ
- A woman with a history of previously normal tests may be managed more conservatively with a new mildly abnormal result
- A woman with prior abnormal results faces a lower threshold for colposcopy for the same current result
The clinical action thresholds in the ASCCP system are: ≥4% 5-year CIN 3+ risk → colposcopy; ≥60% → expedited treatment; <0.15% → return to 5-year screening. Most mildly abnormal Pap results in women with previously normal screening histories fall below the colposcopy threshold and qualify for 1-year surveillance. For comprehensive information on the screening context for these results, see our guide to cervical cancer screening.
What Is a Colposcopy?
Colposcopy is the procedure performed to evaluate most abnormal Pap smear results. It is typically performed by a gynecologist or gynecological specialist in an office setting and takes approximately 10–20 minutes. Understanding the procedure reduces anxiety for women referred for colposcopy:
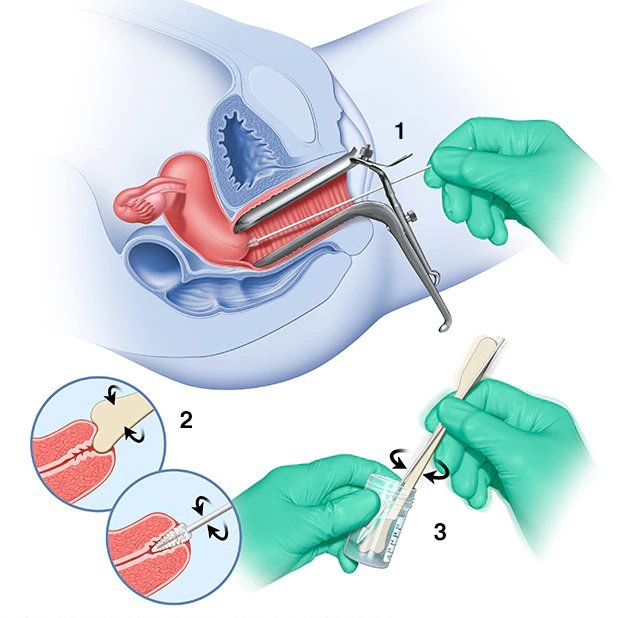
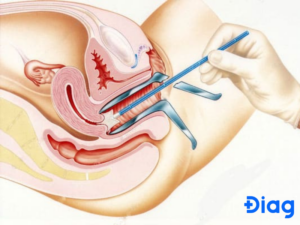
- Speculum insertion: A speculum is inserted to expose the cervix, just as during a Pap smear.
- Colposcope positioning: The colposcope — a lighted magnifying instrument positioned outside the vagina, not inserted — is focused on the cervix. It magnifies the cervical surface 7.5–40 times, allowing detailed visual examination of the transformation zone and any abnormal areas.
- Acetic acid application: Dilute acetic acid (similar to white vinegar, 3–5% concentration) is applied to the cervix with a cotton swab. Areas of CIN (pre-cancer) turn white (acetowhite) due to the increased protein density of abnormal cells reacting with the acid. The degree of acetowhitening and its characteristics (sharp or diffuse borders, density, vascular patterns) help the colposcopist identify which areas to biopsy.
- Lugol’s iodine (optional): Iodine solution may be applied to further delineate abnormal areas — normal squamous cells stain dark brown due to glycogen content; abnormal cells that lack glycogen remain unstained (iodine-negative).
- Biopsy: Any acetowhite areas are sampled with a cervical punch biopsy forceps — a small, sharp instrument that takes a 3–4mm piece of cervical tissue. Most women experience brief cramping during biopsy; the procedure does not require anesthesia.
- Endocervical curettage (ECC): In most cases, the endocervical canal is also sampled using a small curette to collect cells and tissue from the canal above the transformation zone (since the colposcope cannot visualize inside the canal).
After colposcopy, light spotting and mild cramping lasting 1–2 days are normal. Women should avoid intercourse, tampons, and vaginal products for 1 week following biopsy to allow the biopsy sites to heal.
What Biopsy Results Mean
The biopsy tissue from colposcopy is analyzed by a pathologist, who reports the histological diagnosis using the CIN (cervical intraepithelial neoplasia) grading system or the newer LAST (Lower Anogenital Squamous Terminology) classification:
- Normal / negative for CIN: No pre-cancerous changes found; return to surveillance (repeat co-test in 1–3 years depending on clinical context).
- CIN 1 (or LSIL histologically): Mild dysplasia; most resolves spontaneously. Treatment is not routinely recommended. Observation with repeat testing is standard.
- CIN 2 (or HSIL histologically, moderate dysplasia): Treatment is recommended for women ages 25 and older. For women ages 21–24 or pregnant women, observation may be offered because of the substantial regression rate in these groups.
- CIN 3 (or HSIL histologically, severe dysplasia / carcinoma in situ): Treatment is always recommended. CIN 3 has a 30–50% lifetime risk of progressing to invasive cancer without treatment and does not spontaneously regress at the same rate as lower-grade lesions.
Treatment of CIN 2 and CIN 3: LEEP and Other Options
When colposcopy confirms CIN 2 or CIN 3, treatment involves either excisional or ablative removal of the transformation zone and the pre-cancerous tissue.
LEEP (Loop Electrosurgical Excision Procedure): The most commonly performed cervical excision procedure in the United States. A thin wire loop carrying electrical current is used to excise the transformation zone and any visible lesion in a single pass. The excised tissue is sent for pathological examination, confirming the diagnosis and ensuring the lesion was completely removed (negative margins). LEEP is performed in a physician’s office under local anesthesia (cervical block). Recovery involves light spotting and discharge for 2–4 weeks; intercourse and tampon use should be avoided for 4 weeks.
Cold knife cone biopsy: A surgical procedure performed in the operating room under general or regional anesthesia, using a scalpel to excise a cone-shaped portion of the cervix containing the transformation zone. Cold knife cone biopsy provides the highest-quality specimen for pathological examination and is preferred when: glandular cell abnormalities (AIS) are suspected, the entire lesion cannot be visualized colposcopically, or prior LEEP did not achieve clear margins.
Ablative procedures (cryotherapy, laser ablation): These destroy (rather than excise) the transformation zone and are therefore less commonly used today because they do not provide a specimen for pathological confirmation of diagnosis and completeness of treatment. Cryotherapy — freezing the transformation zone with nitrous oxide or carbon dioxide — is still used in resource-limited settings. Laser ablation allows more precise control of the treatment area. Both are appropriate for select patients with fully visualized lesions and negative ECC.
Surveillance After Treatment
Treatment of CIN 2 or CIN 3 significantly reduces but does not eliminate the risk of recurrence or residual disease. Post-treatment surveillance is therefore essential for an extended period. Per ASCCP 2019 guidelines, after treatment for CIN 2 or CIN 3:
- Co-testing (HPV + Pap smear) at 6 months after treatment
- If the 6-month co-test is negative: annual co-testing for the subsequent 2 years, then every 3 years for up to 25 years total from the time of treatment
- Any positive result during this extended surveillance period triggers prompt re-evaluation with colposcopy
This long surveillance period reflects the fact that treated CIN 3 has a residual lifetime risk of cervical cancer that is several times higher than the general population risk, even after successful treatment with negative margins. Women who have had CIN 2 or CIN 3 should not assume that surveillance can be discontinued after a few normal results — the ASCCP guidelines are very specific about the duration and intensity of post-treatment follow-up.
Frequently Asked Questions
I have had multiple normal Pap smears and now have an abnormal result. Does this mean something changed?
Yes — it likely means a new HPV infection has occurred or a previously undetected one has now caused visible cellular changes. Having prior normal Pap smears is reassuring but does not prevent future HPV infection. Most new abnormal Pap smear results in women with previously normal screening histories represent new HPV infections that may resolve spontaneously — this context (prior normal results) is explicitly incorporated into the ASCCP 2019 risk calculator, which often results in more conservative management for women with previously normal screening compared to those with prior abnormalities.
My Pap smear was abnormal but my HPV test was negative. What does this mean?
An abnormal Pap (such as ASC-US) with a negative HPV test is a reassuring combination. High-risk HPV causes the overwhelming majority of significant cervical pre-cancer. An ASC-US or LSIL finding with a negative HPV test most likely reflects a benign reactive change, hormonal effect, or very minor non-HPV-related cytological variation. The recommended next step in this scenario is typically a return to routine screening at the appropriate interval, rather than colposcopy. This is one advantage of co-testing: the HPV result significantly refines the risk interpretation of a mildly abnormal Pap result.
Will I need a hysterectomy for an abnormal Pap smear?
No. An abnormal Pap smear — even one that leads to a diagnosis of CIN 3 — is almost never an indication for hysterectomy. CIN 2 and CIN 3 are successfully treated with LEEP or cold knife cone biopsy, which are outpatient or minor surgical procedures that preserve the uterus and cervix. Hysterectomy is only considered in the rare situation where CIN 3 recurs after multiple excisional procedures, the margins cannot be cleared, or there is concurrent uterine pathology requiring hysterectomy for separate reasons.
Can I get pregnant after LEEP?
Most women can conceive normally after LEEP. However, LEEP removes a portion of the cervix, which may slightly increase the risk of cervical incompetence and preterm birth in subsequent pregnancies, particularly if a large amount of cervical tissue was removed or if multiple LEEP procedures have been performed. Women who have had LEEP and wish to conceive should inform their obstetrician about their treatment history so that appropriate cervical length monitoring can be performed during pregnancy. For more information about cervical cancer and its symptoms, see our guide to cervical cancer symptoms.
Sources
- Perkins RB, et al. 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors. J Low Genit Tract Dis. 2020;24(2):102–131.
- American Cancer Society. The American Cancer Society Guidelines for Cervical Cancer Screening.
- American College of Obstetricians and Gynecologists. Cervical Cancer Screening (ACOG FAQ).
- National Cancer Institute. Cervical Cancer Screening.
- Nayar R, Wilbur DC (eds). The Bethesda System for Reporting Cervical Cytology, 3rd ed. Springer, 2015.
Psychological Impact and Coping with an Abnormal Pap Smear
Receiving an abnormal Pap smear result can be a source of significant anxiety, fear, and even shame for many women — particularly those who are unfamiliar with the Bethesda System terminology, the distinction between pre-cancerous and cancerous findings, or the common prevalence of HPV-related cervical changes in the general population. Research consistently documents that women who receive abnormal Pap smear results report elevated anxiety, distress about HPV stigma, concern about the impact on their relationships, and worry about their future fertility and cancer risk — even when the clinical finding is relatively minor (such as ASC-US or LSIL).
Several strategies can help manage the anxiety associated with an abnormal Pap smear result:
- Get accurate information: Understanding your specific result category, what it means, and what the recommended next step is transforms an abstract fear into a manageable clinical situation. The most important action after receiving an abnormal result is to contact your healthcare provider to clarify the specific category, the recommended follow-up, and the timeline for that follow-up.
- Put it in perspective: Approximately 3.5 million American women receive abnormal Pap smears each year, and the vast majority do not develop cervical cancer. The screening system is working when an abnormal result is found — it has identified a finding that warrants evaluation before cancer can develop.
- Follow through on recommended evaluation: The single most important response to an abnormal Pap smear result is to complete the recommended follow-up — whether that is a repeat co-test in one year, a colposcopy, or surveillance after treatment. Avoidance of follow-up is the most significant risk factor for an early-stage finding progressing to invasive cancer that could have been prevented.
- Seek support: Many gynecology clinics have nurse navigators or patient advocates who can explain results and guide women through the colposcopy process. Asking questions at each step — what was found, what does it mean, what happens next — is appropriate and encouraged.
The abnormal Pap smear, despite the anxiety it produces, is not a crisis — it is the system working as designed, identifying a potential issue at the stage when it can most effectively be addressed. Completing the recommended evaluation is the appropriate and effective response to any abnormal cervical cancer screening result.