What Is Cervical Cancer?
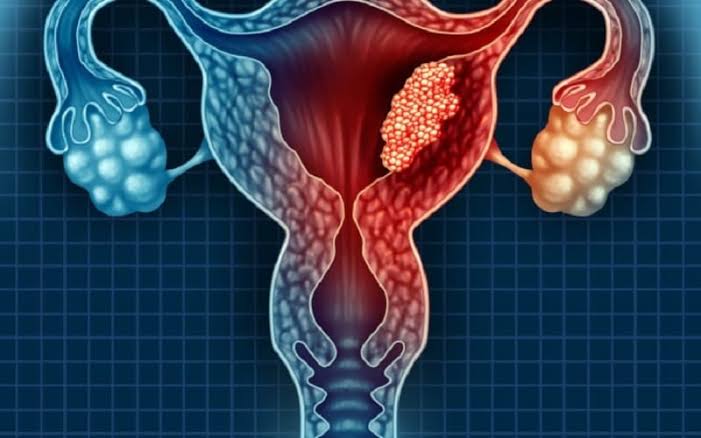
Cervical cancer is a malignancy originating in the cells of the cervix — the lower, narrow portion of the uterus that connects to the vagina. It is the fourth most common cancer in women worldwide, with approximately 660,000 new cases and 350,000 deaths annually according to WHO 2022 data. In the United States, approximately 13,820 new cases and 4,360 deaths occur each year (American Cancer Society, 2024 estimates).
What makes cervical cancer unusual among solid tumors is that it is one of the most preventable cancers in medicine. The combination of HPV vaccination and regular cervical screening can prevent the vast majority of cases — yet cervical cancer remains a significant cause of cancer death globally, primarily because screening and vaccination remain inaccessible in many parts of the world. Understanding the biology, risk factors, and prevention options for cervical cancer is essential for every woman.
For information on identifying warning signs, see our guide to cervical cancer symptoms. For guidance on screening schedules and what to expect, see our articles on cervical cancer screening and Pap smear testing.
Types of Cervical Cancer
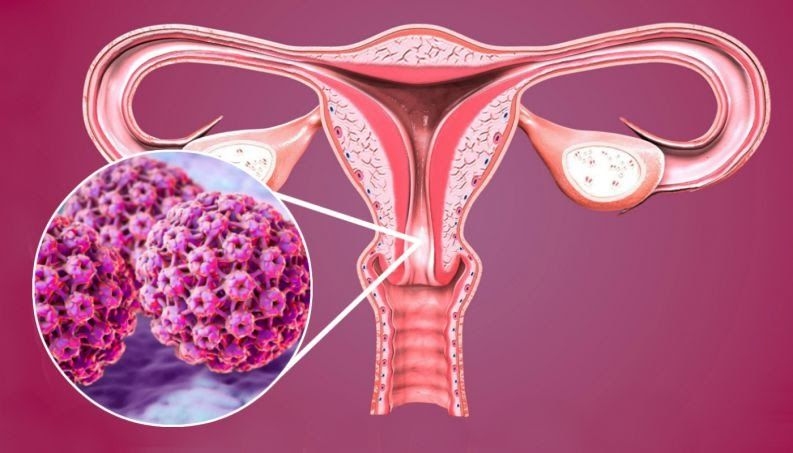
Most cervical cancers arise at the transformation zone — the area of the cervix where the squamous cells of the outer cervix (ectocervix) meet the glandular cells of the cervical canal (endocervix). This junction, called the squamocolumnar junction, is where HPV infections most commonly establish themselves and where pre-cancerous changes most frequently develop.
Squamous cell carcinoma (SCC) accounts for approximately 70–80% of cervical cancers. It arises from the squamous epithelial cells of the ectocervix and transformation zone and is most strongly associated with HPV types 16 and 31. SCC typically progresses through identifiable pre-cancerous stages (CIN 1, CIN 2, CIN 3) that can be detected and treated before invasive cancer develops.
Adenocarcinoma accounts for approximately 15–25% of cervical cancers and has been increasing in incidence over recent decades, even in countries with established Pap smear screening programs. It arises from the glandular cells of the endocervix (inside the cervical canal), is more strongly associated with HPV type 18, and is more difficult to detect with standard Pap cytology because the endocervical cells are less accessible to the brush used for cervical sampling. HPV testing and co-testing catch adenocarcinoma precursors more reliably than Pap alone.
Less common cervical cancer types include adenosquamous carcinoma (mixed type, 3–5%), small cell/neuroendocrine carcinoma (rare but highly aggressive), and clear cell carcinoma (rare; associated with in-utero DES exposure in daughters of women who took DES before 1971).
The Role of HPV in Cervical Cancer
Human papillomavirus (HPV) is a small, double-stranded DNA virus with more than 200 genotypes. The epidemiological association between HPV and cervical cancer — established by Harald zur Hausen, who received the Nobel Prize in Physiology or Medicine for this discovery in 2008 — is among the strongest cause-and-effect relationships in human oncology.
High-risk (oncogenic) HPV types include types 16, 18, 31, 33, 45, 52, and 58. HPV 16 and 18 together cause approximately 70% of all cervical cancers, with HPV 16 particularly prevalent in squamous cell carcinomas and HPV 18 particularly prevalent in adenocarcinomas. Types 31, 33, 45, 52, and 58 cause most of the remaining cases.
Low-risk HPV types (primarily types 6 and 11) cause genital warts but do not cause cervical cancer. These are included in the Gardasil 9 vaccine for prevention of condylomata acuminata, not for cancer prevention.
HPV infection is extremely common: approximately 80% of sexually active adults will acquire at least one HPV genotype during their lifetime. The vast majority of HPV infections — even with high-risk types — are cleared by the immune system within 1–2 years without causing any lasting harm. Persistent infection with high-risk HPV that is not cleared by the immune system is the prerequisite for cervical cancer development. Factors that impair HPV clearance — HIV infection, immunosuppressive medications, smoking, and possibly other cofactors — increase the risk that infection will persist and progress.
The molecular mechanism of HPV carcinogenesis involves two viral oncoproteins:
- HPV E6 protein: Binds to and degrades TP53, the key cellular tumor suppressor. Loss of TP53 function prevents damaged cells from undergoing apoptosis, allowing mutation accumulation.
- HPV E7 protein: Binds to and inactivates the retinoblastoma protein (Rb), releasing E2F transcription factors and driving uncontrolled cell proliferation. Loss of Rb function is a hallmark of many cancers, but in HPV-driven cervical cancer it is achieved consistently through this viral protein mechanism rather than mutation.
How Cervical Cancer Develops: The CIN Continuum
Cervical cancer does not typically arise suddenly — it develops over years to decades through identifiable pre-cancerous stages called cervical intraepithelial neoplasia (CIN). This predictable, slow progression through detectable pre-cancerous stages is what makes cervical cancer uniquely preventable with routine screening:
- CIN 1 (mild dysplasia): Abnormal cells limited to the lower one-third of the cervical epithelium. Approximately 60% regress spontaneously. Less than 1% progress to invasive cancer. Often managed with observation rather than treatment.
- CIN 2 (moderate dysplasia): Abnormal cells in the lower two-thirds. Approximately 40% regress; 5% progress to invasive cancer. Treatment (excision or ablation) is typically recommended, particularly in women over 25.
- CIN 3 (severe dysplasia / carcinoma in situ): Full-thickness epithelial involvement. Approximately 12% progress to invasive cancer without treatment; persistent CIN 3 does not reliably regress. Treatment is strongly recommended.
- Invasive carcinoma: Tumor cells breach the basement membrane and invade the cervical stroma. At this stage, cancer is no longer preventable with screening — only treatable.
The time from initial HPV infection to invasive cervical cancer typically spans 10–15 years. This extended window is precisely why Pap smear and HPV testing programs — performed every 3 to 5 years — are effective: there are multiple opportunities to catch and treat pre-invasive disease before it progresses.
Risk Factors for Cervical Cancer
HPV infection is the necessary cause of virtually all cervical cancers, but HPV infection alone is not sufficient — most HPV infections clear without consequence. Several cofactors influence whether HPV persists and whether CIN progresses to invasive cancer:
- Persistent high-risk HPV infection: The most important risk factor; determines who is at elevated risk of cervical cancer from the population of HPV-infected individuals
- Smoking: Doubles cervical cancer risk; tobacco carcinogens are detectable in cervical mucus and appear to impair the local immune response against HPV
- HIV infection / immunosuppression: Severely impairs HPV clearance; HIV-positive women have rates of CIN and cervical cancer 5–6 times higher than HIV-negative women; transplant recipients on immunosuppressive therapy similarly elevated
- Long-term oral contraceptive use: Modest increased risk for adenocarcinoma specifically, with >5 years of use; risk returns to baseline after stopping
- Multiple sexual partners / early sexual debut: Increases probability of high-risk HPV exposure, not a direct carcinogen
- High parity: Modest association; hypothesized to relate to hormonal effects and cervical trauma
- Lack of screening: Most cervical cancer deaths occur in women who have never been screened or who have not been screened in the prior 5 years; disparities in access to screening drive racial/ethnic and international inequalities in cervical cancer mortality
- Low socioeconomic status: Reduces access to vaccination, screening, and timely treatment of abnormal results
Symptoms of Cervical Cancer
Early-stage cervical cancer is frequently asymptomatic — a fact that underscores the critical importance of routine screening rather than waiting for symptoms to appear. When symptoms develop, they often indicate disease that has progressed beyond the earliest stages:
- Abnormal vaginal bleeding: The most common and clinically important symptom. Includes post-coital bleeding (after intercourse — the most specific symptom for cervical pathology), intermenstrual spotting or bleeding, and postmenopausal bleeding. Any unexplained vaginal bleeding warrants prompt gynecological evaluation.
- Abnormal vaginal discharge: Watery, mucoid, or blood-tinged discharge that may have an unusual odor; can reflect tumor necrosis or infection within the tumor
- Pelvic pain: May reflect locally advanced disease with parametrial or pelvic sidewall involvement
- Pain with intercourse (dyspareunia)
- Advanced disease symptoms: Leg swelling (lymphedema from pelvic lymph node involvement), back or flank pain, difficulty urinating (hydronephrosis from ureteral compression), fistula formation (abnormal connections between the vagina and bladder or rectum), unexplained weight loss
The presence of post-coital bleeding — even a single episode — should prompt cervical examination. While the majority of cases of post-coital bleeding are caused by benign conditions (cervical ectropion, polyp, infection), cervical cancer must be excluded in any woman with this symptom.
For a comprehensive review of warning signs and when to seek evaluation, see our detailed article on cervical cancer symptoms.
Diagnosis of Cervical Cancer
The diagnostic pathway for cervical cancer begins with screening — either Pap smear, HPV testing, or co-testing — and progresses to confirmatory tissue diagnosis:
Pap smear (cervical cytology): Collects cells from the cervix and transformation zone, examines them under microscopy for cellular abnormalities (ASCUS, LSIL, HSIL, AGC). Effective for detecting squamous cell precursors; less sensitive for adenocarcinoma. False-negative rate ~20–30% per test cycle; repeated testing over time substantially reduces cumulative false-negative rate.
HPV DNA testing: Detects high-risk HPV DNA in cervical samples. More sensitive than Pap cytology alone (sensitivity ~95% vs. ~70% for CIN 2+). Available as primary HPV testing (alone) or co-testing (combined with Pap).
Co-testing (Pap + HPV): The highest sensitivity approach; a normal co-test result provides reassurance extending 5 years rather than 3 years. USPSTF-recommended option for women 30–65.
Colposcopy: Performed when screening is abnormal. A colposcope provides 8–15× magnification of the cervix; acetic acid and Lugol’s iodine are applied to highlight abnormal areas (acetowhite lesions, mosaic patterns, punctation). Directed biopsies are taken from abnormal-appearing areas.
Cervical biopsy: Provides histological diagnosis of CIN grade or invasive carcinoma. Required to distinguish CIN 2/3 from invasive disease.
Cone biopsy (LEEP or cold-knife conization): Removes the transformation zone in a cone-shaped excision for diagnosis and definitive treatment of CIN 2/3. May be diagnostic of microinvasive cancer (Stage IA).
Cervical Cancer Stages (FIGO Classification)
Cervical cancer staging uses the FIGO (International Federation of Gynecology and Obstetrics) system, updated in 2018 to allow imaging and pathological nodal assessment. Staging determines treatment approach and prognosis:
- Stage I: Cancer confined entirely to the cervix
- IA1: Microscopic invasion ≤3mm depth
- IA2: Invasion 3–5mm depth
- IB1: Clinically visible tumor <2cm or microscopic >5mm
- IB2: Tumor 2–4cm
- IB3: Tumor ≥4cm
- Stage II: Extends beyond the cervix but not to the pelvic sidewall or lower third of vagina
- IIA: Upper vaginal involvement
- IIB: Parametrial involvement
- Stage III: Extends to pelvic sidewall or lower third of vagina; includes pelvic or para-aortic lymph node involvement; includes hydronephrosis
- Stage IV: Invades bladder/rectal mucosa (IVA) or has distant metastases (IVB)
Treatment of Cervical Cancer
Treatment strategy depends primarily on stage at diagnosis, with fertility preservation considerations playing an important role for young women with early-stage disease:
Early-stage disease (Stage IA1 – IB1):
- Fertility-preserving options: LEEP or cold-knife conization (microinvasive disease); radical trachelectomy (removes cervix but preserves uterus for selected IB1 tumors <2cm)
- Non-fertility-preserving: Simple hysterectomy (IA1) or radical hysterectomy ± sentinel lymph node biopsy/pelvic lymph node dissection (IB1); pelvic radiation as alternative for patients not suitable for surgery
Locally advanced disease (Stage IB3 – IVA):
- Standard: Concurrent cisplatin-based chemotherapy (cisplatin acts as a radiosensitizer) + external beam radiation therapy (EBRT) to the pelvis + brachytherapy (intracavitary or interstitial)
- Addition of bevacizumab (anti-VEGF) to chemoradiation showed survival benefit in the GOG 240 trial
Metastatic/recurrent disease (Stage IVB / recurrent):
- Systemic chemotherapy: cisplatin + paclitaxel ± bevacizumab (first-line)
- Pembrolizumab (anti-PD-1 immune checkpoint inhibitor): FDA-approved for PD-L1-positive advanced/metastatic cervical cancer based on the KEYNOTE-826 trial, which demonstrated improved overall survival compared to chemotherapy alone
- Tisotumab vedotin: antibody-drug conjugate targeting tissue factor; FDA-approved second-line for recurrent cervical cancer
- Clinical trials: multiple emerging targets including other checkpoint inhibitors, PARP inhibitors in homologous recombination-deficient tumors, and novel ADCs
HPV Vaccination: Preventing Cervical Cancer
HPV vaccination represents one of the most effective cancer prevention interventions ever developed. Gardasil 9, the currently available HPV vaccine in the US, protects against nine HPV types: the two low-risk types (6 and 11) causing genital warts, and seven high-risk types (16, 18, 31, 33, 45, 52, 58) that collectively cause approximately 90% of HPV-attributable cervical cancers.
Current ACIP/CDC recommendations for HPV vaccination:
- Routine vaccination: ages 11–12 (can start at age 9)
- Catch-up vaccination: through age 26 if not previously vaccinated
- Shared clinical decision-making: ages 27–45 (benefit decreases with prior HPV exposure)
- 2-dose schedule: if series started before age 15 (0 and 6–12 months)
- 3-dose schedule: if series started at age 15 or older, or for immunocompromised individuals (0, 1–2, and 6 months)
The clinical evidence for HPV vaccination is now substantial. Population-level studies from countries with high vaccination coverage (Australia, UK, Scotland) have demonstrated 85–90% reductions in CIN 2+ diagnoses in vaccinated cohorts, and Australia is projected to become the first country to virtually eliminate cervical cancer as a public health problem within this decade. The vaccine must be given before HPV exposure to be maximally effective — it does not treat existing HPV infection — which is why adolescent vaccination before sexual debut is strongly preferred.
Cervical cancer is one of the most preventable cancers. HPV vaccination protects against the virus types that cause ~90% of cervical cancers. Pap smear and HPV testing detect pre-cancerous changes over a 10–15-year window before they become invasive cancer. Together, vaccination + screening can prevent the overwhelming majority of cervical cancer cases. Women who have not been vaccinated still benefit from screening, and women who are vaccinated still need regular cervical screening because the vaccine does not protect against all high-risk HPV types.
Cervical Cancer Screening Guidelines
Current screening guidelines from major US organizations:
USPSTF (2018):
- Ages 21–29: Pap smear alone every 3 years
- Ages 30–65: Pap + HPV co-testing every 5 years, OR Pap alone every 3 years, OR primary HPV testing every 5 years
- Ages <21 and >65: Screening not recommended for average-risk women with adequate prior screening
ACS (2020 updated guidelines):
- Preferred: primary HPV testing every 5 years, starting at age 25
- Acceptable: co-testing every 5 years or Pap alone every 3 years
- Upper age limit: 65 with adequate prior screening and low risk
For detailed screening guidance including what to do if results are abnormal, see our comprehensive guide to cervical cancer screening and our article on Pap smear testing.
Survival Rates for Cervical Cancer
Cervical cancer survival depends strongly on stage at diagnosis — a pattern consistent with most solid tumors and one that reinforces the value of early detection through screening:
- Stage I (localized): ~92% 5-year relative survival
- Stage II (regional, limited): ~68% 5-year relative survival
- Stage III (regional, advanced): ~47% 5-year relative survival
- Stage IV (distant metastases): ~17% 5-year relative survival
- All stages combined: ~67% 5-year relative survival (US, SEER data)
The stark difference between stage I (~92%) and stage IV (~17%) survival rates illustrates why cervical cancer screening is so important: it finds disease at Stage I, when cure rates are excellent, rather than at Stage III or IV, when treatment is palliative for many patients.
Frequently Asked Questions
Does the HPV vaccine prevent all cervical cancers?
Gardasil 9 protects against nine HPV types that cause approximately 90% of cervical cancers. The remaining ~10% are caused by HPV types not covered by the vaccine, meaning that even vaccinated women require regular cervical screening. Additionally, the vaccine does not treat existing HPV infections, so women who receive it after HPV exposure receive partial protection. Both vaccination and screening are recommended.
Can you get cervical cancer without ever having had sex?
HPV — the cause of virtually all cervical cancers — is transmitted primarily through sexual contact, including skin-to-skin genital contact (not just intercourse). In extremely rare cases, HPV may be transmitted non-sexually (vertical transmission at birth, etc.), but cervical cancer in the absence of any sexual HPV exposure history is exceptionally uncommon. Women who have never been sexually active have very low cervical cancer risk and may not need routine cervical screening, but should discuss their individual situation with a healthcare provider.
Is cervical cancer hereditary?
Cervical cancer is not primarily a hereditary cancer — unlike breast/ovarian cancer (BRCA), colorectal cancer (Lynch syndrome), or other hereditary cancer syndromes. The primary cause is HPV infection, an environmental exposure. However, genetic factors that affect immune response may influence HPV clearance and therefore cervical cancer risk. Women with a family history of cervical cancer should maintain regular screening but do not require earlier-than-standard initiation or more frequent screening based on family history alone.
What happens after an abnormal Pap smear?
The follow-up path depends on what type of abnormality was found. Most low-grade abnormalities (ASCUS, LSIL) are managed with repeat testing in 1 year or HPV co-testing, not immediate colposcopy. High-grade results (HSIL, ASC-H) or persistent abnormalities typically prompt colposcopy with directed biopsy. If CIN 2 or CIN 3 is found on biopsy, excisional or ablative treatment is usually recommended. The large majority of abnormal Pap results do not represent cervical cancer — they represent pre-cancerous changes that can be monitored or treated. For a step-by-step guide, see our article on cervical cancer screening.
Sources
- World Health Organization. Cervical Cancer Fact Sheet. 2023.
- American Cancer Society. Key Statistics for Cervical Cancer. 2024.
- US Preventive Services Task Force. Cervical Cancer Screening Recommendation. 2018.
- National Cancer Institute. Cervical Cancer Treatment (PDQ).
- Arbyn M et al. Estimates of incidence and mortality of cervical cancer in 2018. Lancet Global Health. 2020.
Global Burden and Health Equity
One of the most striking features of the global cervical cancer landscape is the stark disparity between high-income and low-income countries. In countries with established Pap smear programs — the United States, United Kingdom, the Nordic countries, Australia — cervical cancer incidence has declined by 50–80% over the past half-century. In sub-Saharan Africa, parts of Southeast Asia, and other regions where screening infrastructure and HPV vaccination programs are limited or absent, cervical cancer remains a leading cause of cancer mortality in women.
This disparity is not driven by biology: women in low-income countries are not inherently at higher biological risk for cervical cancer than women in high-income countries. The disparity reflects access — access to HPV vaccination for adolescents, access to Pap smear or HPV testing and follow-up, and access to treatment for pre-cancerous lesions when they are found. Cervical cancer is therefore classified by WHO as an example of a cancer that is a problem of inequity rather than intractable biology.
The WHO global strategy to accelerate the elimination of cervical cancer, adopted in 2020, set three targets by 2030: 90% of girls fully vaccinated with the HPV vaccine by age 15, 70% of women screened with a high-performance test by ages 35 and 45, and 90% of women with identified cervical disease receiving treatment. Reaching these targets is projected to prevent more than 4 million deaths over the following 25 years, with the greatest impact in low-income countries.