The most common assumption about high cholesterol is that it is caused by eating too much fat. This assumption is partially correct and substantially incomplete. Diet is one of several significant contributors to elevated LDL cholesterol — but genetics, physical inactivity, body weight, medical conditions, medications, and hormonal changes all play roles that can dominate diet entirely in many people.
Understanding the causes of high cholesterol matters for two practical reasons. First, identifying the primary driver helps determine which interventions are most likely to work. Someone whose elevated LDL is largely genetic will not be adequately managed by dietary changes alone. Second, recognizing the multifactorial nature of the condition helps people avoid the self-blame that sometimes follows a diagnosis — which can paradoxically reduce motivation to engage with the aspects that are genuinely modifiable.
Genetics — The Most Underestimated Cause
Research consistently shows that approximately 50 percent of the variation in LDL cholesterol between individuals is determined by genetic factors. Two people eating identical diets and maintaining identical lifestyles can have substantially different LDL levels — and in many cases, the person with the higher level is not doing anything wrong.
Familial hypercholesterolemia (FH) is the most clinically significant single-gene cause. FH is caused by mutations in genes involved in LDL receptor function — primarily the LDL receptor gene itself (LDLR) in 85 to 90 percent of cases, or the ApoB gene, or PCSK9. These mutations reduce the liver’s ability to clear LDL from the blood, producing persistently elevated LDL regardless of diet.
Heterozygous FH — inheriting one mutated copy — affects approximately 1 in 250 people, producing LDL levels of 190 to 400 mg/dL. Without treatment, men with heterozygous FH have approximately a 50 percent probability of a coronary event by age 50; women have approximately 30 percent by age 60. Homozygous FH — inheriting two mutated copies — is rarer (1 in 300,000 to 1,000,000) and produces LDL above 400 to 600 mg/dL, often causing cardiovascular events in childhood.
Familial combined hyperlipidemia (FCH), affecting approximately 1 in 100 people, produces varying combinations of elevated LDL and elevated triglycerides. Polygenic hypercholesterolemia — LDL elevated by the cumulative effect of many common genetic variants — accounts for the majority of elevated LDL in people without identified single-gene disorders. Anyone with LDL persistently above 190 mg/dL, particularly with family history of early cardiovascular disease, should be evaluated for FH. For more on what cholesterol is and how LDL works, see our article on what is cholesterol.
Dietary Causes of High Cholesterol
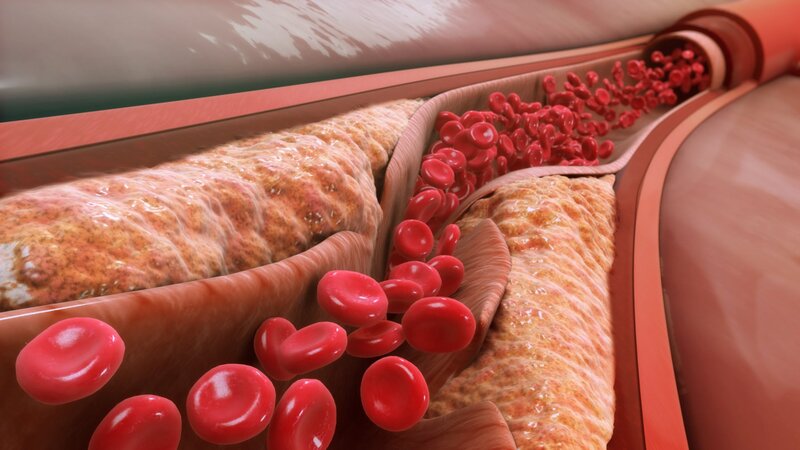
Saturated fat is the most powerful dietary driver of elevated LDL. Saturated fatty acids — found in fatty meat, butter, cheese, coconut oil, and palm oil — reduce LDL receptor expression in liver cells, causing LDL to accumulate in the blood. Replacing saturated fat with unsaturated fat (olive oil, nuts, fatty fish) consistently lowers LDL; replacing it with refined carbohydrates produces a more mixed outcome.
Trans fat is particularly harmful — it raises LDL and simultaneously lowers HDL. Industrial trans fats (partially hydrogenated oils) were largely eliminated from the US food supply after June 2018, though trace amounts remain.
Dietary cholesterol — in eggs, shellfish, organ meats — plays a secondary role for most people. The liver compensates for increased dietary cholesterol by reducing its own production. The 2015–2020 Dietary Guidelines for Americans removed the previous 300 mg/day limit, citing insufficient supporting evidence. Approximately 25 percent of people are dietary “hyper-responders” who show more pronounced LDL changes in response to dietary fat and cholesterol.
Refined carbohydrates and added sugars primarily raise triglycerides and VLDL, indirectly shifting LDL toward the smaller, denser, more atherogenic particle pattern. This explains why diets high in sugary beverages and processed grains can worsen lipid profiles even when saturated fat intake appears modest. For more on triglycerides’ role, see our article on triglycerides and heart health.
Physical Inactivity and High Cholesterol
Regular aerobic exercise raises HDL by 5 to 10 percent, reduces triglycerides, and modestly lowers LDL through multiple mechanisms: activating lipoprotein lipase (which clears triglyceride-rich lipoproteins), increasing LDL receptor expression in the liver, and improving overall metabolic function. Physical inactivity reverses these benefits — sedentary individuals have lower LPL activity, lower HDL, and tend toward a more atherogenic lipid pattern.
The minimum effective dose for lipid benefit appears to be approximately 30 minutes of moderate-intensity aerobic exercise most days of the week. Even walking at a brisk pace for 30 minutes daily produces measurable improvements in triglycerides and HDL.
Obesity and Insulin Resistance
Excess body weight — particularly abdominal adiposity — impairs lipid metabolism through several simultaneous pathways. Visceral fat releases large amounts of free fatty acids directly into the portal circulation, stimulating the liver to increase VLDL production and raising both triglycerides and LDL. Insulin resistance, which accompanies obesity in a large proportion of affected individuals, impairs lipoprotein lipase activity (reducing triglyceride clearance), increases hepatic VLDL secretion, lowers HDL, and shifts LDL composition toward the more atherogenic small dense particle pattern.
This cluster — high triglycerides, low HDL, small dense LDL — is the characteristic lipid pattern of metabolic syndrome and type 2 diabetes, sometimes called “atherogenic dyslipidemia.” Weight loss of 5 to 10 percent of body weight reliably improves the entire lipid profile simultaneously.
Medical Conditions That Cause High Cholesterol
Several medical conditions affect lipid metabolism and can produce significantly elevated cholesterol independently of diet or lifestyle. Identifying these secondary causes is important because treating the underlying condition often normalizes cholesterol without specific lipid-lowering therapy.
Hypothyroidism is the most important secondary cause of elevated LDL. Thyroid hormone regulates LDL receptor expression in liver cells — when thyroid levels are low, LDL receptor activity decreases and LDL accumulates. Even subclinical hypothyroidism (elevated TSH with normal T4) can raise LDL measurably. Treating hypothyroidism with levothyroxine often normalizes cholesterol. This is why thyroid testing is appropriate in anyone with newly identified elevated cholesterol, particularly with other hypothyroid symptoms.
Type 2 diabetes and prediabetes are closely linked to atherogenic dyslipidemia. Elevated blood glucose glycates LDL particles making them more atherogenic, insulin resistance increases hepatic VLDL production, and the overall pattern — elevated triglycerides, low HDL, increased small dense LDL — raises cardiovascular risk beyond what standard LDL measurement captures.
Chronic kidney disease impairs multiple aspects of lipoprotein metabolism. Nephrotic syndrome — characterized by heavy protein loss in the urine — causes profound LDL elevation as the liver dramatically increases lipoprotein production to compensate for lost plasma oncotic pressure. Cushing syndrome (excess cortisol) raises both LDL and triglycerides. Polycystic ovary syndrome (PCOS), affecting 8 to 13 percent of women of reproductive age, is commonly accompanied by insulin resistance and the atherogenic dyslipidemia pattern.
Medications That Raise Cholesterol
Corticosteroids — prednisone, dexamethasone — raise LDL and triglycerides in a dose-dependent manner. Some beta-blockers — particularly older, non-selective agents like propranolol and atenolol — raise triglycerides and lower HDL; newer vasodilatory agents (carvedilol, nebivolol) have more favorable lipid profiles. Thiazide diuretics at higher doses can modestly raise LDL and triglycerides. Oral contraceptives — the lipid effect varies by progestin type; levonorgestrel-containing formulations tend to lower HDL more than desogestrel or norgestimate. Isotretinoin frequently raises triglycerides and can significantly raise LDL; lipid monitoring is required during treatment. Some antipsychotics (clozapine, olanzapine) cause weight gain and raise triglycerides. Some antiretroviral medications (older HIV protease inhibitors) raise triglycerides and LDL.
When a physician suspects medication is contributing to elevated cholesterol, reviewing alternatives where clinically feasible is worthwhile before initiating lipid-lowering therapy.
Age, Sex, and Hormonal Changes
LDL cholesterol rises gradually with age in both sexes. Before menopause, women typically have lower LDL and higher HDL than men of the same age — estrogen promotes LDL receptor expression and supports HDL production. After menopause, estrogen levels fall significantly, and LDL rises — typically by 10 to 15 mg/dL or more — while HDL may decline modestly. By their mid-sixties, women’s LDL levels often equal or exceed those of men of the same age. This post-menopausal LDL surge explains why women who had consistently normal cholesterol for decades may find borderline or high results at their next screening test, having had no change in diet or lifestyle.
Smoking and Alcohol
Smoking lowers HDL by approximately 5 mg/dL and appears to promote LDL oxidation, making LDL particles more atherogenic even at the same cholesterol concentration. Quitting smoking improves HDL within weeks. Heavy alcohol consumption substantially raises triglycerides through its effects on hepatic metabolism. Moderate alcohol modestly raises HDL (5 to 10 mg/dL), but this is not sufficient justification to recommend drinking for cardiovascular benefit given alcohol’s other health risks.
The Multifactorial Nature of High Cholesterol
In clinical practice, most people with elevated LDL have a multifactorial cause — some combination of genetic predisposition, dietary patterns, physical activity level, body weight, and possibly a secondary condition or medication. Two people can eat identical diets and have LDL levels differing by 60 to 80 mg/dL, entirely due to genetic differences in LDL receptor activity. Two people with identical genetics can differ by 30 to 40 mg/dL based purely on lifestyle differences.
A thorough evaluation of elevated cholesterol includes not just the lipid panel but also family history, current medications, thyroid function, blood glucose, kidney function, and lifestyle factors. The causes of high cholesterol that are identified shape the treatment approach — which interventions are most effective and most important to address. For a guide to understanding your results, see our articles on LDL vs HDL cholesterol and what is a lipid panel.
High cholesterol has no single cause. It emerges from the intersection of genetics, diet, activity, body composition, underlying conditions, medications, and hormonal lifecycle. This complexity is clarifying: it identifies multiple points of intervention. For lifestyle-driven elevation, dietary modification and exercise can produce meaningful improvement. For significant genetic contributions, medication may be necessary. For secondary causes, treating the underlying condition should come first. High cholesterol is discoverable through testing and treatable through multiple pathways — see our article on high cholesterol symptoms: why testing matters for the case for early screening.
How to Identify the Primary Cause in Your Own Case
When a physician evaluates elevated cholesterol, the goal is not just to document the number but to understand its origin — because the cause shapes the treatment. A systematic evaluation typically considers the following elements.
Family history. The single most informative non-laboratory indicator of genetic hypercholesterolemia is a detailed family history. Questions to address: Has any first-degree relative (parent, sibling, child) been diagnosed with high cholesterol or started on statin therapy at an early age? Has any family member had a heart attack, stroke, or coronary artery bypass surgery before age 55 (in men) or 65 (in women)? Does any family member have a known diagnosis of familial hypercholesterolemia? A positive family history in the context of LDL above 190 mg/dL should prompt FH evaluation, including possible genetic testing and cascade screening of first-degree relatives.
Medication review. A complete list of current medications — including over-the-counter supplements, hormonal contraceptives, and recently stopped medications — should be reviewed for cholesterol-raising agents. This step is frequently overlooked but can be consequential. Corticosteroids, isotretinoin, some antipsychotics, anabolic steroids (including non-prescribed performance-enhancing use), and certain HIV medications all raise LDL or triglycerides substantially and should be identified before attributing elevation to primary dyslipidemia.
Secondary condition screening. A basic metabolic panel that includes thyroid-stimulating hormone (TSH), fasting blood glucose or hemoglobin A1c (HbA1c), kidney function tests (creatinine, GFR, urine protein), and liver enzymes provides the most important secondary cause screen. Hypothyroidism — the most correctable secondary cause — is detectable with a simple TSH test. Diabetes and prediabetes require glucose or HbA1c. Kidney disease requires creatinine and urinalysis. These tests are typically ordered alongside a lipid panel as part of a comprehensive cardiovascular risk workup.
Dietary assessment. A brief dietary history focusing on saturated fat sources (frequency of red meat, butter, full-fat dairy, coconut oil, processed foods) and refined carbohydrate intake (sugary beverages, white bread, sweets) provides context for how much dietary modification might lower LDL. Rough quantification — rather than exhaustive dietary recall — is usually sufficient to identify people with high saturated fat intake versus those whose diet appears already appropriate and whose elevation is primarily genetic or secondary.
Physical activity assessment. Exercise history — type, frequency, duration — helps identify whether increasing physical activity is likely to produce meaningful lipid benefit. Sedentary individuals who increase to 150 minutes of moderate-intensity aerobic activity per week often see HDL increases of 5 to 10 percent and triglyceride reductions of 20 to 30 percent, which is clinically significant.
Body composition assessment. Waist circumference is more informative than weight or BMI for predicting the atherogenic dyslipidemia associated with metabolic syndrome. Waist circumference above 40 inches in men or 35 inches in women, combined with elevated triglycerides and low HDL, identifies metabolic syndrome regardless of total cholesterol level.
When Genetic Testing for High Cholesterol Is Appropriate
Genetic testing for cholesterol disorders is not appropriate for everyone with elevated cholesterol, but it is increasingly valuable in specific clinical scenarios.
Suspected familial hypercholesterolemia. When a patient has LDL above 190 mg/dL, tendon xanthomas, corneal arcus under age 45, a family history of premature cardiovascular disease, or a family member with known FH, genetic testing can confirm the diagnosis by identifying a pathogenic variant in LDLR, ApoB, or PCSK9. A confirmed genetic diagnosis: (1) supports the clinical diagnosis if LDL alone is ambiguous; (2) enables cascade testing of first-degree relatives using a targeted panel for the identified variant, which is far more efficient than full sequencing; and (3) qualifies patients for PCSK9 inhibitor therapy under insurance criteria that may require a genetic diagnosis.
Cascade screening after FH diagnosis. When one family member is confirmed to have an FH-causing mutation, genetic testing of first-degree relatives (parents, siblings, and children over age 2) is recommended. This approach is significantly more efficient than cholesterol testing alone in young relatives — children of an FH parent may not yet have LDL levels that clearly exceed age-adjusted thresholds, but genetic testing can definitively identify whether they inherited the pathogenic variant.
Ambiguous cases in young people. A young adult with LDL of 165 mg/dL may or may not have FH — polygenic hypercholesterolemia, dietary factors, and early secondary causes can all produce LDL in this range. A polygenic risk score or FH genetic panel can provide clarifying information about whether the elevation reflects high genetic risk (warranting more aggressive and earlier treatment) or moderate polygenic plus lifestyle risk (where lifestyle optimization has more potential to normalize levels).
Very high triglycerides. Triglycerides above 1000 mg/dL, particularly in younger patients or those without obvious secondary causes, may reflect familial hypertriglyceridemia or familial chylomicronemia syndrome — conditions caused by mutations in genes like LPL, APOC2, APOA5, and others. Genetic testing in this context helps guide treatment selection, since the genetic cause determines which therapies are most likely to be effective.
The Cholesterol-Raising Effect of Specific Dietary Patterns
While individual macronutrients — saturated fat, trans fat, dietary cholesterol — are the most studied dietary drivers of elevated LDL, real-world eating patterns interact with these components in ways that are important to understand.
Western dietary pattern. Characterized by high intake of red and processed meat, butter, full-fat dairy, refined grains, sugary beverages, and processed snacks, the Western pattern consistently raises both LDL and triglycerides in observational and intervention studies. It is the dietary pattern most strongly associated with elevated cardiovascular risk in epidemiological research.
Mediterranean dietary pattern. Characterized by high intake of vegetables, legumes, whole grains, fruits, nuts, olive oil, and fish, with moderate poultry and dairy and low red meat and processed food intake, the Mediterranean pattern consistently lowers LDL, raises HDL, reduces triglycerides, and lowers cardiovascular event rates. The PREDIMED trial demonstrated a 30 percent relative risk reduction in major cardiovascular events in high-risk participants randomized to a Mediterranean diet supplemented with olive oil or nuts compared to a low-fat control diet.
Low-carbohydrate dietary patterns. Very low-carbohydrate (ketogenic) diets reduce triglycerides and often raise HDL substantially — effects driven by the dramatic reduction in refined carbohydrate intake. The LDL response varies: some individuals see LDL decrease (particularly when saturated fat intake is moderate), while others — particularly those on very high saturated fat ketogenic diets — see significant LDL increases. The “lean mass hyper-responder” phenomenon — marked LDL elevation on low-carbohydrate diets in lean, active individuals — is an active area of research with unclear long-term cardiovascular implications.
Plant-based dietary patterns. Diets that replace animal proteins and fats with plant proteins (legumes, tofu, nuts) and unsaturated plant fats consistently lower LDL. The Portfolio Diet — a plant-based dietary approach specifically designed to lower cholesterol through combinations of soluble fiber, plant sterols, soy protein, and nuts — achieves LDL reductions comparable to low-dose statin therapy in some studies.
The practical takeaway: dietary patterns that lower LDL work through reducing saturated fat, increasing unsaturated fat and soluble fiber, and reducing refined carbohydrate load — regardless of which specific dietary label they carry. The specific foods consumed matter less than whether they shift the pattern in those directions.
The Role of Stress in Cholesterol Levels
Psychological stress has a recognized but often overlooked effect on lipid levels. Acute psychological stress triggers the release of cortisol and catecholamines (adrenaline, noradrenaline), which can transiently elevate LDL and triglycerides through hormonal effects on hepatic lipid metabolism and adipose tissue lipolysis. A high-stress test day or a particularly difficult period in the weeks before a cholesterol test may contribute to a higher-than-typical reading.
Chronic psychological stress has more sustained effects. Chronically elevated cortisol — from persistent work pressure, relationship difficulties, bereavement, financial stress, or post-traumatic stress — has been associated in longitudinal studies with higher LDL, lower HDL, and higher cardiovascular event rates. The mechanisms likely involve both direct hormonal effects on lipid metabolism and indirect effects through stress-related behaviors: poorer diet choices, reduced exercise, increased alcohol consumption, and disrupted sleep, all of which independently worsen lipid profiles.
This does not mean that stress is a primary cause of high cholesterol in the way that genetics or saturated fat intake are — but it does mean that cholesterol testing during periods of acute life stress may produce temporarily elevated results, and that stress management is a legitimate (if often underutilized) component of comprehensive cardiovascular risk reduction.