
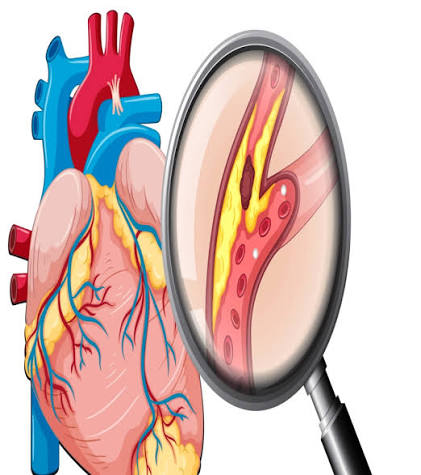
Atherosclerosis is the disease that most people are actually describing when they talk about “heart disease” — and yet most people could not define it precisely. It is not simply high cholesterol. It is not simply “hardening of the arteries.” It is a specific, chronic inflammatory disease of the arterial wall in which plaques — deposits of lipids, immune cells, smooth muscle cells, connective tissue, and calcium — form within the inner layer of arteries over decades, silently narrowing vessels and creating structures that, if they rupture, trigger the blood clots responsible for most heart attacks and strokes.
What is atherosclerosis in terms of its clinical consequences? It is the underlying cause of coronary artery disease, most ischemic strokes, peripheral artery disease, and abdominal aortic aneurysm — together accounting for more deaths annually, worldwide, than any other single pathological process. Understanding what atherosclerosis is, how it develops, and what accelerates or slows it is foundational to understanding cardiovascular risk.
What Is Atherosclerosis? A Precise Definition
The word comes from Greek: “athere” means porridge or gruel — a reference to the soft, lipid-rich material at the core of an atherosclerotic plaque — and “sclerosis” means hardening, referring to the fibrous, calcified structure that surrounds it. Together, they describe the two characteristic features of the disease: a soft, cholesterol-rich center enclosed in a harder shell.
Atherosclerosis is distinct from the broader term arteriosclerosis, which refers to any thickening or stiffening of artery walls that occurs with aging. Atherosclerosis is the most clinically significant specific type of arteriosclerosis — characterized not just by stiffening but by the inflammatory plaque-building process described above.
A mature atherosclerotic plaque consists of:
- A necrotic lipid core: dead foam cells (cholesterol-engorged macrophages), cholesterol crystals, extracellular lipid, and inflammatory cells
- A fibrous cap: smooth muscle cells embedded in a collagen matrix, physically separating the thrombogenic core from flowing blood
- Calcification: calcium deposits that develop particularly in older plaques and are measurable non-invasively by CT (as the Coronary Artery Calcium score)
The diseases that atherosclerosis directly causes depend on which arteries are affected. In the coronary arteries, it produces coronary artery disease (CAD) — responsible for angina and myocardial infarction. In the carotid and cerebral arteries, it underlies most ischemic strokes and TIAs. In the peripheral arteries of the legs, it causes peripheral artery disease (PAD). In the aorta, it contributes to abdominal aortic aneurysm risk. These are not separate diseases with different causes — they are different anatomical expressions of the same underlying pathological process.
What Causes Atherosclerosis?
Atherosclerosis begins with endothelial injury — disruption of the single layer of cells lining the inside of arteries. The triggers for this injury are the modifiable and non-modifiable risk factors for cardiovascular disease, and understanding them helps explain why the standard risk factor checklist (cholesterol, blood pressure, smoking, diabetes, family history) is not arbitrary — each factor maps to a specific mechanism in the disease process.
Elevated LDL cholesterol is the primary driver of plaque initiation and progression. LDL particles cross the injured endothelium into the artery wall, where they become oxidized. Oxidized LDL is recognized by macrophage scavenger receptors, taken up voraciously, and begins the foam cell cascade that forms the structural foundation of plaque. More LDL particles in the blood means more crossing the endothelium, more oxidation, and faster plaque growth. This is why lowering LDL reduces cardiovascular events — not by improving symptoms, but by reducing the substrate for the process that causes the disease.
Hypertension damages the endothelium directly through the mechanical force of elevated blood pressure — particularly at arterial branch points and curves where flow is turbulent. High blood pressure also increases the permeability of endothelial cells, making it easier for LDL particles to penetrate the arterial wall. Sustained hypertension dramatically accelerates atherosclerotic plaque development.
Cigarette smoking is one of the most powerful individual modifiable risk factors for atherosclerosis. Tobacco smoke contains thousands of compounds that are directly toxic to endothelial cells, promote oxidative modification of LDL, activate platelets, and increase the thrombogenicity of blood. Smokers develop atherosclerosis at a faster rate and at younger ages than non-smokers.
Diabetes mellitus and insulin resistance accelerate atherosclerosis through multiple mechanisms. Elevated blood glucose leads to glycation of LDL particles and endothelial proteins, making both more susceptible to oxidative damage. Insulin resistance promotes a dyslipidemia characterized by elevated triglycerides, low HDL, and an excess of small, dense LDL particles — each of which contributes to plaque formation. Diabetes approximately doubles the cardiovascular risk attributable to the same LDL level compared to non-diabetic individuals.
Obesity — particularly abdominal obesity — promotes atherosclerosis primarily through its association with metabolic syndrome: insulin resistance, elevated triglycerides, low HDL, hypertension, and a pro-inflammatory state. Adipose tissue (particularly visceral fat) secretes pro-inflammatory cytokines that promote endothelial dysfunction and accelerate the atherosclerotic process.
Age is the most fundamental non-modifiable risk factor. Atherosclerosis is a cumulative process — the longer the arterial wall is exposed to elevated LDL, hypertension, and oxidative stress, the more plaque accumulates. Men face elevated risk at age 45 and older; women at age 55 and older (when estrogen’s protective effects on LDL receptor expression are lost after menopause).
Family history and genetics matter because approximately 40 to 60 percent of LDL variation is genetically determined. Familial hypercholesterolemia — a genetic condition causing severely elevated LDL from birth — affects 1 in 250 people and is one of the most important causes of premature atherosclerosis and heart attack in people under 50. Elevated lipoprotein(a) — Lp(a), a genetically determined modified LDL variant — also significantly increases atherosclerosis risk independently of LDL-C.
Additional emerging risk factors include chronic kidney disease (an independent cardiovascular risk accelerant), inflammatory diseases such as rheumatoid arthritis, lupus, and psoriasis, obstructive sleep apnea, and certain HIV antiretroviral medications. For a comprehensive overview of factors that raise LDL and drive cholesterol-related risk, see our guide to causes of high cholesterol.
Atherosclerosis Symptoms — Why the Disease Is So Dangerous
The most important clinical fact about atherosclerosis is also one of the least intuitive: it typically produces no symptoms for decades. The process begins in adolescence and young adulthood — fatty streaks are present in the coronary arteries of virtually all young Americans by their twenties. Fibrous plaques develop through the thirties and forties. And yet most people have no idea this is happening.
Symptoms appear only when one of two things occurs: the plaque has grown large enough to significantly narrow the artery (causing flow-limiting stenosis), or a plaque ruptures and triggers a blood clot that acutely obstructs flow. In approximately half of people who have a heart attack, the MI is the first clinical sign that they had coronary artery disease at all. There was no preceding angina, no warning, and no opportunity to intervene based on symptoms alone.
The symptoms that do eventually appear depend entirely on which arteries are involved:
- Coronary arteries — stable angina: predictable chest pressure or tightness triggered by exertion and relieved within minutes by rest or nitroglycerin; or acute MI (heart attack) when a plaque ruptures
- Carotid and cerebral arteries — TIA (brief, reversible neurological symptoms: sudden weakness, speech difficulty, vision loss) or ischemic stroke with permanent neurological damage; approximately 87% of all strokes are ischemic
- Peripheral arteries (legs) — intermittent claudication: cramping or aching pain in the calf, thigh, or buttock during walking, relieved by rest; in advanced PAD, rest pain and non-healing ulcers or gangrene
- Renal arteries — resistant hypertension and progressive chronic kidney disease
- Aorta — abdominal aortic aneurysm, typically silent until rupture produces sudden severe back or abdominal pain — a surgical emergency
Because symptoms are so often absent until a serious event occurs, proactive screening — particularly cholesterol testing and cardiovascular risk assessment — is the primary tool for identifying people at risk before they experience an event. For more on why symptoms are unreliable for detecting high cholesterol and atherosclerosis risk, see high cholesterol symptoms and why testing matters.
How Atherosclerosis Is Diagnosed
Because atherosclerosis is silent for most of its course, diagnosis must be proactive — pursued through testing in people at risk rather than waiting for symptoms to prompt investigation.
Blood tests provide the primary risk assessment framework. The standard lipid panel (LDL-C, HDL-C, triglycerides, total cholesterol) is the first tool for assessing atherogenic lipid burden. ApoB is a more direct measure of atherogenic particle number than LDL-C and identifies patients with high particle burden despite seemingly acceptable LDL-C. Lp(a) — at least one lifetime measurement is now recommended by many guidelines for all adults; elevated Lp(a) (above 50 mg/dL or 125 nmol/L) identifies patients at substantially higher cardiovascular risk than LDL-C alone would suggest. hs-CRP (high-sensitivity C-reactive protein) adds risk information beyond the lipid panel and is useful in intermediate-risk patients to guide statin decisions. Fasting glucose or HbA1c is essential for detecting diabetes or prediabetes as risk-accelerating conditions. For a full overview of what lipid testing involves, see what is a lipid panel.
Non-invasive imaging can detect atherosclerosis directly:
- Coronary Artery Calcium (CAC) Score — a low-radiation CT scan that detects and quantifies calcified plaque in the coronary arteries; no contrast needed; CAC = 0 indicates very low 10-year risk; CAC ≥ 100 indicates established plaque requiring treatment; now guideline-recommended for intermediate-risk patients where the statin decision is uncertain
- Carotid Intima-Media Thickness (CIMT) — ultrasound measure of carotid artery wall thickness; correlates with cardiovascular risk; used in research and selected clinical settings
- CT Coronary Angiography (CTCA) — contrast-enhanced CT that visualizes coronary arteries directly; detects both calcified and soft (non-calcified) plaque; increasingly used for stable chest pain evaluation
- Ankle-Brachial Index (ABI) — compares blood pressure in the ankle to the arm; ABI below 0.9 is diagnostic of peripheral artery disease; simple, inexpensive, non-invasive
Functional and invasive testing is used when atherosclerosis is already suspected or when symptoms need evaluation. Exercise stress testing detects ischemia caused by flow-limiting stenosis. Stress echocardiography and nuclear stress testing are more sensitive imaging-based functional alternatives. Coronary angiography (cardiac catheterization with contrast dye) remains the gold standard for definitive stenosis assessment and allows simultaneous percutaneous coronary intervention (PCI) if indicated.
How Atherosclerosis Is Treated
Treatment of atherosclerosis falls into three broad categories: lifestyle modification, pharmacological therapy, and invasive procedures to restore blood flow in critically narrowed arteries.
Lifestyle modification addresses the modifiable risk factors that drive the disease. A Mediterranean-style dietary pattern reduces LDL, lowers inflammation, and reduces cardiovascular event rates in clinical trials. Aerobic exercise (at least 150 minutes per week of moderate-intensity activity) improves endothelial function, reduces LDL and triglycerides, raises HDL, lowers blood pressure, and reduces insulin resistance. Smoking cessation produces rapid and significant cardiovascular benefit — measurable within weeks and clinically meaningful within one to two years.
Pharmacological therapy forms the cornerstone of atherosclerosis treatment for most patients with elevated risk:
Statins are the most widely prescribed and most evidence-based lipid-lowering medications. They inhibit HMG-CoA reductase — the rate-limiting enzyme in cholesterol synthesis — reducing hepatic cholesterol production and upregulating LDL receptors. Beyond LDL lowering, statins have anti-inflammatory and plaque-stabilizing effects: they reduce macrophage activity in plaques, increase collagen synthesis in the fibrous cap, and decrease the inflammatory signals that thin fibrous caps and increase rupture risk. Every 1 mmol/L reduction in LDL-C with statin therapy is associated with roughly a 22 percent relative reduction in major cardiovascular events.
Ezetimibe inhibits cholesterol absorption from the gut; when added to a statin, it reduces LDL-C by an additional 15 to 25 percent. The IMPROVE-IT trial demonstrated that adding ezetimibe to simvastatin in post-ACS patients further reduced cardiovascular events — confirming that additional LDL lowering beyond statins produces additional clinical benefit.
PCSK9 inhibitors (evolocumab, alirocumab) — injectable monoclonal antibodies that block the PCSK9 protein — dramatically increase LDL receptor density in the liver, reducing LDL-C by 50 to 60 percent on top of statin therapy. Large trials (FOURIER, ODYSSEY OUTCOMES) have demonstrated significant reductions in cardiovascular events in very high-risk patients.
Antiplatelet therapy — low-dose aspirin or P2Y12 inhibitors (clopidogrel, ticagrelor) — reduces the risk of thrombosis at the site of a ruptured or eroded plaque. Antiplatelet therapy is standard for secondary prevention but is more carefully weighed against bleeding risk in primary prevention settings.
Colchicine — low-dose colchicine, an anti-inflammatory agent traditionally used for gout — was shown in the COLCOT (2019) and LoDoCo2 (2020) trials to reduce recurrent cardiovascular events in patients with coronary artery disease, independent of LDL effects. This directly supports the inflammatory hypothesis of atherosclerosis.
Interventional and surgical procedures restore blood flow in arteries significantly narrowed by plaque. Percutaneous coronary intervention (PCI) uses a catheter-based balloon and stent to open a narrowed coronary artery. Coronary artery bypass grafting (CABG) surgically bypasses blocked coronary arteries using graft vessels. Carotid endarterectomy or carotid artery stenting addresses significant symptomatic carotid stenosis. Peripheral vascular interventions (angioplasty, stenting, bypass surgery) treat significant peripheral artery disease.
Can Atherosclerosis Be Prevented?
Atherosclerosis cannot be cured — the lifetime of accumulated plaque cannot be fully removed. But the disease process can be dramatically slowed, stabilized, and partially reversed with early and sustained risk factor control.
Primary prevention — reducing risk before the first cardiovascular event — is the highest-value intervention precisely because atherosclerosis is a cumulative process. Decades of lower LDL, better blood pressure control, and not smoking translate into dramatically less plaque burden at the age when cardiovascular events become most likely. A person who keeps LDL at 70 mg/dL throughout their forties and fifties accumulates substantially less plaque than someone whose LDL averages 140 mg/dL over the same period, even if their measured 10-year risk at any given moment appears similar.
This is why lifetime risk framing is increasingly important — particularly for younger adults. A 45-year-old with moderately elevated LDL and mild hypertension may have a low 10-year calculated cardiovascular risk, but a very high lifetime risk. The window in which prevention is most effective is before significant plaque accumulates — which means earlier intervention, not waiting until 10-year risk crosses a threshold.
Secondary prevention — after a first cardiovascular event — requires more aggressive intervention. Dual antiplatelet therapy, high-intensity statins targeting LDL below 55 mg/dL, and additional agents (ezetimibe, PCSK9 inhibitors if needed) are standard in this context. The goal is to prevent the second event, which carries high probability without treatment.
For more on the mechanism by which cholesterol contributes to plaque formation, see cholesterol and plaque buildup in arteries. To understand your LDL and HDL numbers in the context of atherosclerosis risk, see LDL vs HDL cholesterol.
Sources: American Heart Association — Atherosclerosis (heart.org) | National Heart, Lung, and Blood Institute — Atherosclerosis (nhlbi.nih.gov) | Centers for Disease Control and Prevention — Heart Disease Facts (cdc.gov)
Atherosclerosis in Different Arteries: How the Disease Varies by Location
Although the underlying cellular process is the same — LDL oxidation, foam cell formation, fibrous plaque development — the clinical consequences of atherosclerosis vary dramatically depending on which arterial territory is most affected. Understanding these location-specific manifestations helps explain why the same disease can present so differently in different patients.
Coronary artery disease is the most studied and most common manifestation. The coronary arteries supply oxygenated blood to the heart muscle itself. When atherosclerotic narrowing limits coronary blood flow, the result is ischemia — insufficient oxygen delivery to myocardial cells. Mild-to-moderate stenosis (40–70% narrowing) may produce no symptoms at rest but cause exertional angina when increased cardiac workload demands more blood flow than the narrowed vessel can supply. Severe stenosis (above 70–80%) may cause angina even at rest. Plaque rupture in any coronary artery, regardless of the degree of stenosis, can trigger sudden complete occlusion and heart attack.
Carotid artery disease poses a different kind of threat. The carotid arteries supply the brain, and atherosclerosis at the carotid bifurcation — where the common carotid artery divides into the internal and external carotid — is the most common source of cardioembolic stroke. Unlike coronary atherosclerosis, where the primary event mechanism is usually plaque rupture with local thrombosis, carotid atherosclerosis often causes stroke through embolism: fragments of plaque or thrombus that break off from the carotid and travel upstream into smaller cerebral arteries, where they lodge and block flow to brain tissue. This is why asymptomatic carotid disease discovered incidentally can represent significant stroke risk even if the patient has never experienced symptoms.
Peripheral artery disease — atherosclerosis of the arteries supplying the legs — deserves particular attention because it is both under-diagnosed and under-treated. PAD affects approximately 6.5 to 12 million Americans, yet many patients attribute their claudication symptoms (leg cramping with walking) to aging, arthritis, or “being out of shape” rather than arterial disease. The Ankle-Brachial Index (ABI) — a simple, inexpensive measurement — can diagnose PAD in an office setting. People with PAD have substantially elevated cardiovascular risk: their concurrent coronary and cerebrovascular atherosclerosis means that the diagnosis of PAD is itself a marker for high cardiac and stroke event risk, regardless of whether they have had coronary symptoms.
Aortic atherosclerosis affects the body’s largest artery and contributes to cardiovascular risk in two ways: as a source of emboli (plaques in the aorta can shed material into downstream arterial territories) and as a substrate for aneurysm development. Abdominal aortic aneurysm (AAA) — a pathological dilation of the aorta below the renal arteries — is strongly associated with atherosclerosis and shares most of its risk factors (smoking, male sex, age, hypertension). AAA is typically asymptomatic until rupture, which carries a mortality rate of 80 to 90 percent. One-time ultrasound screening for AAA is recommended for men aged 65 to 75 who have ever smoked.
Atherosclerosis and Systemic Inflammation: The Emerging Picture
The inflammatory nature of atherosclerosis has become increasingly central to how cardiologists think about both risk assessment and treatment. For decades, the lipid hypothesis — that LDL is the necessary substrate for plaque formation — was the dominant framework. While that remains true, the recognition that plaque development and, especially, plaque destabilization are driven by inflammatory processes has opened new avenues for both diagnosis and treatment.
The clearest clinical evidence came from the JUPITER trial, which demonstrated that statin therapy reduced cardiovascular events in patients with low LDL cholesterol but elevated hs-CRP — a marker of systemic inflammation. This suggested that statin benefit was partly anti-inflammatory rather than solely due to LDL lowering. The CANTOS trial, which tested an anti-inflammatory monoclonal antibody (canakinumab) against IL-1β in patients with prior MI and elevated hs-CRP, demonstrated reduced recurrent cardiovascular events without any change in LDL. The most recent addition to this evidence base is low-dose colchicine, shown in COLCOT and LoDoCo2 to reduce cardiac events in CAD patients — again, without lipid-lowering effects.
Practically, this means that measuring hs-CRP alongside LDL can provide a more complete picture of cardiovascular risk — particularly in intermediate-risk patients where the statin decision is uncertain. A patient with LDL of 120 mg/dL and hs-CRP of 4 mg/L has a different risk profile than one with the same LDL and hs-CRP below 1 mg/L. The combination of lipid burden and inflammatory activation together drive both plaque development and vulnerability to rupture.
It also means that risk-reduction strategies with anti-inflammatory properties beyond LDL lowering — including Mediterranean dietary patterns, regular physical activity, smoking cessation (which dramatically reduces vascular inflammation), and weight loss in obesity — contribute to atherosclerosis management through mechanisms that complement LDL lowering rather than duplicating it.