Peripheral Artery Disease Symptoms and Diagnosis

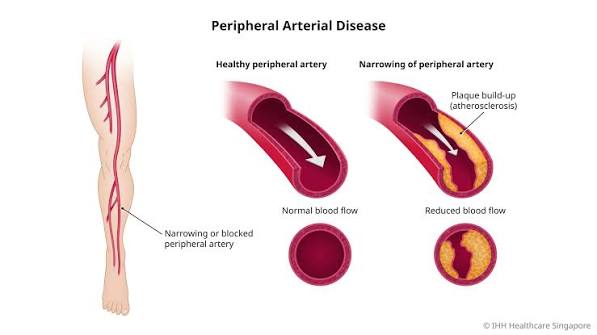
Peripheral artery disease symptoms are the clinical expression of progressive atherosclerotic narrowing in the arteries supplying the legs — a disease process that is often silent in its early stages, characteristically symptomatic with exercise as it progresses, and capable of producing limb-threatening ischemia in its advanced form. PAD affects approximately 8 to 10 million Americans, with prevalence rising steeply with age and risk factor burden, yet the majority of PAD patients are either undiagnosed or undertreated — partly because symptoms are absent or atypical in many patients, and partly because the symptoms that are present are frequently misattributed to musculoskeletal conditions, arthritis, or aging.
Recognizing the characteristic symptom patterns of PAD and distinguishing them from musculoskeletal and neurogenic mimics is the first step toward diagnosis, treatment, and — critically — the cardiovascular risk factor management that PAD necessitates. Patients with PAD have substantially elevated rates of heart attack, stroke, and cardiovascular death from the same atherosclerosis that obstructs their leg arteries — making PAD diagnosis a cardiovascular event in its own right that should trigger intensive secondary prevention.
Intermittent Claudication — The Hallmark Symptom of PAD
Intermittent claudication is the defining symptom of symptomatic PAD — a reproducible pattern of muscle pain, cramping, aching, or heaviness in the leg that occurs with walking and is completely relieved by rest. The word “claudication” derives from the Latin “claudicare” (to limp) — reflecting the behavioral consequence of the symptom. Several features distinguish true vascular claudication from musculoskeletal and other causes of leg pain with activity:
Reproducibility: True claudication occurs at a predictable walking distance — the same distance triggers symptoms reliably, walk by walk and day by day (though the distance may vary with speed, incline, and temperature — cold weather and uphill walking shorten the symptom-free distance because they increase metabolic demand). Musculoskeletal pain is less predictable in its relationship to distance walked.
Complete resolution with rest: Claudication resolves completely within 2 to 10 minutes of rest — without changing body position. The patient can simply stop walking and stand still; the pain gradually clears as accumulated metabolic products (lactic acid, adenosine) are washed out by the now-sufficient resting blood flow. Neurogenic claudication from lumbar spinal stenosis also occurs with walking but characteristically requires the patient to sit down or flex forward at the waist to achieve relief — the positional component distinguishes it from vascular claudication. Joint pain from arthritis may worsen with activity but does not have the same rapid, complete, position-independent relief pattern of vascular claudication.
Specific muscle group involvement: The location of claudication pain reflects the arterial anatomy — which segment is obstructed determines which muscle group becomes ischemic with exertion. Calf claudication (the most common location) indicates superficial femoral artery or popliteal artery disease — the most frequent locations for atherosclerotic PAD in the lower extremity. Thigh claudication indicates more proximal disease in the common femoral or profunda femoris artery. Buttock claudication (often with associated hip pain and erectile dysfunction in males — Leriche syndrome) indicates aortoiliac disease — obstruction of the distal aorta or common iliac arteries. This anatomical correlation between symptom location and disease location is useful in guiding vascular imaging to the appropriate arterial segment.
Pain character: Claudication is typically described as a cramping, aching, or tightening sensation — often compared to a severe muscle cramp or the feeling of muscles “giving out.” It rarely has a sharp, shooting, or electric character (more typical of neurogenic pain). The pain involves the belly of the affected muscles rather than the joints.
Rest Pain — When Ischemia Occurs Even Without Walking
Rest pain is a qualitatively different symptom from claudication and indicates a more severe degree of arterial insufficiency — the arterial supply is so restricted that it cannot maintain adequate tissue perfusion even without the increased metabolic demand of exercise. Rest pain in PAD has characteristic features that distinguish it from other causes of foot and leg pain at rest:
Location: Rest pain in PAD occurs in the foot and toes — not the calf (where claudication occurs). The most distal tissues, which are at the end of the arterial distribution and therefore most vulnerable to ischemia when perfusion pressure is severely reduced, suffer pain first. Characteristically, the pain involves the forefoot (ball of foot) and toes, and may be described as burning, aching, or a severe throbbing sensation.
Timing: Rest pain is typically worst at night and in the early morning hours — when the legs are horizontal (eliminating the gravitational assistance to perfusion that occurs when the legs are dependent), when cardiac output is lower during sleep, and when the vasoconstrictive effect of overnight temperature drop further reduces perfusion pressure. Patients often describe awakening at night with severe foot pain and finding relief only by hanging the foot over the side of the bed or briefly walking to the bathroom (both of which restore gravitational perfusion pressure).
Relief pattern: Hanging the leg in a dependent position (over the side of the bed) or walking briefly provides temporary relief from rest pain by increasing perfusion pressure to the foot — but the pain returns when the leg is elevated again. This is the opposite of venous pain (which worsens with dependency and improves with elevation). Many patients with rest pain sleep in a recliner or chair with their legs down to maintain the dependent position that provides some pain relief.
Rest pain indicates critical limb ischemia — a stage where the risk of progression to ulceration, gangrene, and limb loss becomes imminent without revascularization. Any patient with rest pain in the foot requires urgent vascular evaluation.
Critical Limb-Threatening Ischemia — The Most Severe PAD Presentation
Critical limb-threatening ischemia (CLTI) — previously called critical limb ischemia (CLI) — is the most severe stage of PAD and represents tissue loss or impending tissue loss from chronic, severe arterial insufficiency. CLTI is defined by the presence of any of: ischemic rest pain, non-healing ischemic ulcers, or gangrene attributable to arterial occlusive disease. The clinical implications of CLTI are profound:
Without revascularization, approximately 20 to 30 percent of CLTI patients undergo major amputation within 6 months. The 1-year mortality rate in CLTI patients is approximately 20 percent — higher than many malignancies — reflecting the severity of underlying cardiovascular disease in this population. CLTI patients are typically elderly with multiple comorbidities (diabetes, CKD, heart failure) that both increase CLTI risk and complicate revascularization planning.
Ischemic ulcers in PAD typically occur at pressure points and distal locations: the tips of toes, the heel, the lateral foot, and sometimes between the toes from minor trauma in an ischemic foot. They are characteristically pale or necrotic at the base, dry and punched-out in appearance, surrounded by pale or mottled skin rather than the erythema and exudate of infected wounds, and extremely painful (unless peripheral neuropathy from co-existing diabetes masks the pain sensation). The absence of bleeding when the wound edge is debrided (pallor on probing rather than bright red blood) confirms severe ischemia. Venous ulcers, by contrast, occur above the medial malleolus, have a red granulating base with exudate, and are surrounded by hyperpigmented skin from chronic venous hypertension.
Diagnosing PAD — From ABI to Angiography
The diagnostic evaluation of suspected PAD follows a hierarchical approach from non-invasive testing to invasive imaging:
Ankle-brachial index (ABI) is the first-line test for all suspected PAD — a simple bedside measurement of ankle systolic pressure divided by brachial systolic pressure. ABI below 0.9 confirms PAD with sensitivity of approximately 79 to 95 percent and specificity of 95 to 99 percent. ABI above 1.4 indicates arterial calcification (incompressible vessels) requiring the toe-brachial index (TBI) instead — the toe vessels are often spared calcification even when larger leg arteries are incompressible.
Segmental limb pressures and pulse volume recordings (PVRs) extend ABI testing by measuring pressures at multiple levels (high thigh, low thigh, calf, ankle) and recording arterial waveform morphology at each level. This localizes the obstructive disease to specific arterial segments — helping determine whether disease is predominantly aortoiliac, femoral-popliteal, or infrapopliteal — without imaging. PVR waveforms that are monophasic (single forward flow peak without dicrotic notch) indicate significant proximal arterial disease; triphasic waveforms (forward, reverse, and forward again) indicate normal or mildly affected arteries.
Duplex ultrasound provides anatomical and hemodynamic information simultaneously — identifying plaque location, stenosis severity, and collateral vessels — without radiation or contrast. It is the standard first imaging study after ABI in patients being evaluated for revascularization and is used for post-intervention surveillance after angioplasty or stenting.
CT angiography (CTA) of the peripheral arteries provides high-resolution anatomical imaging of the entire arterial tree from the aorta to the tibial vessels — essential for surgical bypass planning and for identifying complex multilevel disease patterns. Radiation and iodinated contrast exposure limit its use in patients with severe CKD (where contrast nephropathy risk is significant) or in very young patients requiring repeated imaging.
Magnetic resonance angiography (MRA) provides peripheral arterial imaging without radiation and with gadolinium contrast that has lower nephrotoxicity than iodinated CT contrast (though gadolinium can cause nephrogenic systemic fibrosis in patients with eGFR below 30 mL/min, limiting its use in severe CKD). MRA tends to overestimate stenosis severity compared to CTA and conventional angiography but provides good anatomical delineation for revascularization planning.
Digital subtraction angiography (DSA) — conventional catheter-based angiography — remains the gold standard for PAD imaging and is typically performed immediately before or during endovascular revascularization (angioplasty, stenting, atherectomy). It provides the highest spatial resolution for tibial and pedal vessel anatomy critical for CLTI revascularization planning, and allows simultaneous treatment of identified lesions.
The Society for Vascular Surgery PAD patient resource covers PAD symptoms, risk factors, and treatment options including supervised exercise therapy and revascularization. The NHLBI PAD symptoms guide explains the characteristic signs of peripheral artery disease and when to seek evaluation. The CDC peripheral artery disease information page reviews PAD epidemiology, risk factors, and clinical features for patient education.
Related reading: Poor Circulation in the Legs | High Blood Pressure and Stroke | Cholesterol and Stroke Risk | Diabetes and Stroke Risk | Smoking and Stroke Risk
Sources
- Gerhard-Herman MD, et al. 2016 AHA/ACC Guideline on the Management of Patients with Lower Extremity PAD. J Am Coll Cardiol. 2017;69(11):e71-e126.
- Norgren L, et al. Inter-Society Consensus for the Management of PAD (TASC II). J Vasc Surg. 2007;45(Suppl S):S5-S67.
- Rutherford RB, et al. Recommended Standards for Reports Dealing with Lower Extremity Ischemia. J Vasc Surg. 1997;26(3):517-538.
- Ankle Brachial Index Collaboration. Ankle Brachial Index Combined with Framingham Risk Score to Predict CVD Events. JAMA. 2008;300(2):197-208.
- Eikelboom JW, et al. Rivaroxaban with or without Aspirin in Stable Cardiovascular Disease (COMPASS). N Engl J Med. 2017;377(14):1319-1330.
Atypical and Asymptomatic PAD — When the Diagnosis Is Easy to Miss
The classic description of PAD — reproducible calf claudication relieved by rest — applies to only about 10 to 35 percent of PAD patients. The majority of patients with confirmed PAD on ABI testing either have no leg symptoms at all (asymptomatic PAD) or have atypical leg symptoms that do not fit the classic claudication pattern. This diagnostic heterogeneity is one of the main reasons PAD remains severely underdiagnosed and undertreated in clinical practice.
Asymptomatic PAD — defined as ABI below 0.9 without any claudication or other leg symptoms — accounts for approximately 20 to 50 percent of all PAD patients, depending on the population studied. These patients have the same or greater cardiovascular event risk as symptomatic PAD patients (because their systemic atherosclerosis burden is just as high), yet they are frequently not identified or treated with appropriate intensity because they never present with leg complaints. Asymptomatic PAD is often discovered incidentally during ABI screening of high-risk individuals (adults over 65, adults over 50 with diabetes or smoking history), during evaluation of other cardiovascular conditions, or through automated analysis of peripheral pulse waveforms in electronic health monitoring systems. The identification of asymptomatic PAD triggers a comprehensive cardiovascular risk reduction strategy even in the absence of leg symptoms.
Atypical leg symptoms — leg pain, aching, or fatigue with exertion that does not meet the strict criteria for classic claudication — are actually more common than typical claudication in PAD patients. These atypical symptoms include: leg pain that occurs at rest as well as with walking (not purely exertional), pain that takes longer than 10 minutes to resolve with rest (more typical of neurogenic or musculoskeletal causes), pain that is not reproducible at the same walking distance each time, and leg fatigue or heaviness rather than pain per se. The Walking Impairment Questionnaire (WIQ) and San Diego Claudication Questionnaire are validated tools for capturing the full spectrum of PAD-related walking symptoms beyond classic claudication.
Why do so many PAD patients have no symptoms? Several mechanisms explain asymptomatic PAD: (1) Extensive collateral arterial development that partially compensates for the flow-limiting stenosis — gradual disease progression allows collateral channels to develop over years, reducing the hemodynamic impact of the stenosis relative to sudden occlusion; (2) Physical inactivity — sedentary patients may never walk far enough to stress the ischemic muscle territory; (3) Peripheral neuropathy (common in diabetic PAD patients) blunting the ischemic pain signal; (4) Adaptive reduction in physical activity — patients unconsciously slow down or shorten their walks to avoid the symptom, never reaching the threshold that would produce claudication.
Distinguishing PAD from Other Causes of Leg Pain
The differential diagnosis of leg pain that might be confused with PAD is extensive. Understanding the distinguishing features of each mimic prevents both misdiagnosis of PAD (treating a non-vascular condition with vascular interventions) and missed PAD (failing to diagnose vascular disease because symptoms are attributed to a benign alternative):
Neurogenic claudication from lumbar spinal stenosis is the most commonly confused condition with vascular claudication. Neurogenic claudication causes leg pain, heaviness, and numbness with walking — but it is caused by neural compression in the narrowed spinal canal rather than vascular ischemia. Key distinguishing features: neurogenic claudication often involves both legs and the buttocks simultaneously; it characteristically requires the patient to sit down or flex forward at the waist to get relief (spinal flexion temporarily widens the spinal canal, decompressing the neural elements) — simply stopping walking while standing does not relieve neurogenic claudication as it does vascular claudication; neurogenic symptoms often begin while standing still and before walking has started; neurogenic claudication may involve sensory symptoms (numbness, tingling, burning paresthesias) more prominently than pure muscle pain. The ABI will be normal in isolated spinal stenosis without concomitant PAD. MRI of the lumbar spine and ABI testing together effectively distinguish the two conditions.
Diabetic peripheral neuropathy causes burning, tingling, or shooting pain in both feet — typically worse at night and improved (or unchanged) with walking. Unlike ischemic rest pain, which occurs only in the foot and is worsened by leg elevation, neuropathic pain is diffuse and not consistently altered by leg position. The ABI may be falsely elevated in diabetic patients due to medial arterial calcification (incompressible tibial arteries giving falsely high ankle pressures), requiring TBI for PAD assessment.
Musculoskeletal causes — osteoarthritis of the hip or knee, muscle strain, tendinopathy, bursitis — cause leg pain that is typically related to specific joint loading rather than a predictable walking distance, is often asymmetric in its relationship to exertion vs. rest, may be reproducible with specific movements (climbing stairs, pivoting) rather than straight-line walking distance, and does not have the consistent complete rest-relief pattern of claudication. Palpation of specific tender points, assessment of joint range of motion, and physical examination of gait and joint loading help distinguish musculoskeletal from vascular pain.
Chronic venous insufficiency causes heaviness, aching, and fatigue in the legs — typically worsened by prolonged standing or sitting (dependency) and improved by leg elevation. Unlike claudication, venous symptoms are not specifically triggered by walking a defined distance and are worse at the end of a day of standing rather than after a specific amount of exertion. Varicose veins, ankle pigmentation (hemosiderin deposition), and swelling above the ankle are characteristic physical findings of chronic venous disease not seen in pure arterial PAD. Duplex ultrasound of the venous system (evaluating for reflux and prior DVT) distinguishes venous from arterial causes.
Treatment Options for PAD — From Exercise to Revascularization
The treatment of symptomatic PAD addresses both the leg symptoms (claudication, critical limb ischemia) and the underlying systemic cardiovascular risk. Treatment is stratified by symptom severity:
For claudication: Supervised exercise therapy (SET) — structured treadmill walking programs under medical supervision — achieves 100 to 150 percent improvement in pain-free walking distance over 3 to 6 months of participation and is recommended as first-line treatment for claudication by ACC/AHA guidelines. The mechanism involves skeletal muscle metabolic adaptations, improved oxygen extraction efficiency, and collateral vessel development. Cilostazol (100 mg twice daily) adds approximately 35 to 50 percent improvement in walking distance on top of exercise therapy. Revascularization (angioplasty, stenting, or surgical bypass) is offered to claudication patients who have an inadequate response to exercise therapy and medications, whose symptoms significantly impair daily function, and whose anatomical disease pattern is amenable to revascularization.
For critical limb-threatening ischemia: Revascularization is the primary treatment — the goal is to restore adequate perfusion to the ischemic foot territory to heal ulcers, relieve rest pain, and prevent amputation. Endovascular revascularization (percutaneous transluminal angioplasty, drug-coated balloon angioplasty, nitinol stenting, atherectomy) is preferred over open surgical bypass when technically feasible, particularly for aortoiliac and femoral-popliteal disease. Surgical bypass (using autogenous vein or prosthetic graft) is preferred for complex multilevel disease, for tibial vessel reconstruction in diabetic CLTI, and when endovascular approaches have failed. Major amputation is reserved for patients where revascularization is not technically feasible or has failed, where the limb is not salvageable (extensive gangrene), or where the patient’s overall medical condition makes revascularization prohibitively risky.
PAD and Cardiovascular Risk — The Systemic Implications
Peripheral artery disease is not simply a disease of the legs — it is a systemic marker of advanced atherosclerosis affecting the entire arterial tree. Patients with diagnosed PAD have approximately 20 to 30 percent five-year mortality from cardiovascular events — a mortality rate comparable to having established coronary artery disease. This elevated systemic risk exists regardless of the leg symptom severity: a patient with asymptomatic PAD carries the same cardiovascular event rate as one with severe claudication, because the ABI reflects systemic atherosclerosis burden rather than local leg ischemia severity.
The connection between PAD and stroke risk is particularly relevant: patients with PAD have a 2 to 3-fold increased risk of ischemic stroke compared to those without PAD, reflecting concurrent carotid and intracranial atherosclerosis. High-intensity statin therapy, blood pressure control below 130/80 mmHg, and antiplatelet therapy are therefore standard of care for all PAD patients regardless of revascularization plan. Learn more about how these shared risk factors contribute across multiple vascular territories in our related articles on poor circulation in the legs and deep vein thrombosis symptoms and prevention.