A PET scan for cancer measures metabolic activity inside the body — not anatomy. Unlike CT or MRI, which produce detailed structural images, a PET scan uses a small amount of radioactive tracer to reveal which cells are consuming the most energy. Because cancer cells grow rapidly and consume glucose at much higher rates than most normal tissues, a PET scan for cancer can detect tumors, identify whether cancer has spread to lymph nodes or distant organs, and measure whether treatment is working — often before any size change appears on CT.
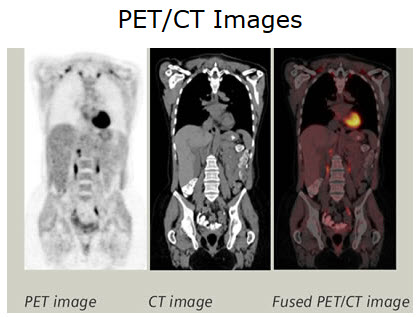
In clinical practice, PET scans are almost always combined with CT in a single session (PET-CT), fusing the metabolic map from PET with precise anatomic detail from CT. This combination is dramatically more accurate than either scan alone. For patients with lymphoma, lung cancer, esophageal cancer, melanoma, and many other cancers, PET-CT is the cornerstone of initial staging, treatment response assessment, and recurrence detection. For a broad overview of all imaging modalities in oncology, see our guide to imaging tests for cancer.
How a PET Scan for Cancer Works
The most common radiotracer is FDG (fluorodeoxyglucose) — a glucose molecule attached to fluorine-18 (F-18), a radioactive isotope with a half-life of 110 minutes. After IV injection, FDG travels through the bloodstream and is taken up by cells proportional to their glucose consumption. Cancer cells, which have dramatically elevated glucose metabolism (the Warburg effect), accumulate FDG at higher concentrations than most surrounding normal tissues.
When F-18 decays, it emits a positron that immediately collides with an electron — releasing two gamma rays traveling in opposite directions at 180 degrees. The PET scanner’s ring of detectors captures these paired signals, computing the precise origin point in 3D space. A full metabolic map is constructed from millions of these detected pairs.
Key measurement — SUVmax: Standardized uptake value (maximum) quantifies FDG uptake in a lesion normalized to body weight. Higher SUVmax = higher metabolic activity, typically correlating with more aggressive tumor biology. Serial SUVmax changes between scans guide treatment response decisions.
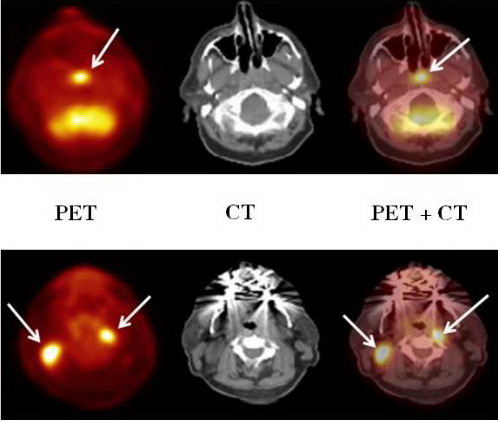
Why PET-CT? PET shows where metabolic activity is concentrated but with limited spatial resolution (~4–5 mm). Without anatomic context, a “hot spot” might be in a lymph node, muscle, bowel loop, or vessel. CT provides the anatomic roadmap. Fused PET-CT images allow precise localization — a mediastinal node, a liver lesion, an adrenal mass — enabling confident staging that neither scan achieves alone.
What Cancers a PET Scan for Cancer Is Best For
FDG-PET-CT is the standard of care for staging, response assessment, and recurrence detection in cancers where it provides information CT or MRI cannot.
| Cancer Type | Primary PET-CT Role |
|---|---|
| Hodgkin lymphoma (HL) | Gold standard for staging, interim response (Deauville), end-of-treatment — replaces CT + bone marrow biopsy |
| Diffuse large B-cell lymphoma (DLBCL) | Staging, interim and end-of-treatment response assessment |
| Non-small cell lung cancer (NSCLC) | Nodal (N) staging; identifies occult M1 disease; avoids futile surgery |
| Esophageal cancer | Detects M1 disease (celiac nodes, liver, bone) changing management in ~20% |
| Melanoma (stage III/IV) | Whole-body staging; occult nodal and visceral metastasis detection |
| Cervical cancer | Pelvic and para-aortic nodal staging; lymph node size criteria are unreliable |
| Head and neck cancer | Nodal staging; occult primary detection in cervical adenopathy |
| Colorectal cancer (recurrence) | CEA-guided recurrence localization when CT is negative or equivocal |
| Thyroid cancer (dedifferentiated) | FDG-avid recurrence when thyroglobulin elevated but I-131 scan negative |
PSMA-PET — The New Standard for Prostate Cancer Imaging
Prostate-specific membrane antigen (PSMA) is dramatically overexpressed on prostate cancer cells and underexpressed in most normal tissues — making it an ideal imaging target. PSMA-targeted PET radiotracers have transformed prostate cancer imaging since FDA approval.
The ProPSMA trial (Lancet 2020) — n=302 men with high-risk prostate cancer — directly compared PSMA-PET-CT vs. conventional imaging (CT + bone scan). PSMA-PET achieved 92% accuracy vs. 65% — a 27-percentage-point difference that fundamentally changed clinical guidelines. PSMA-PET also detected pelvic nodal metastases conventional imaging missed, and identified unexpected distant metastases that altered management in a meaningful proportion of patients.
- Initial staging: PSMA-PET replaced CT + bone scan for high-risk prostate cancer staging in major urology guidelines
- Biochemical recurrence: PSMA-PET detects recurrence site at PSA as low as 0.2 ng/mL — compared to PSA >10 ng/mL typically required for CT + bone scan to reliably localize disease
- PSMA theranostics: Lu-177 PSMA-617 (Pluvicto) — FDA approved March 2022 — delivers radiation to PSMA-expressing prostate cancer cells. VISION trial demonstrated improved OS and rPFS in mCRPC.
FDA-approved PSMA-PET agents: Ga-68 PSMA-11 (2020) and F-18 piflufolastat (2021). For men concerned about prostate cancer detection, see our guide to cancer blood tests including PSA — the trigger that leads to PSMA-PET workup.
PET Scan for Cancer Treatment Response — Before and After Chemotherapy
One of PET’s most powerful applications is measuring whether cancer is responding to treatment — often detecting metabolic response weeks before tumor shrinkage appears on CT.
Lymphoma — Deauville 5-point scale: The Deauville criteria provide a standardized framework for evaluating PET scans in lymphoma — comparing uptake in residual lesions to two reference points: the mediastinum (blood pool) and the liver.
| Deauville Score | Interpretation | Clinical Action |
|---|---|---|
| 1 | No uptake above background | Complete metabolic response |
| 2 | Uptake ≤ mediastinum | Complete metabolic response |
| 3 | Uptake > mediastinum but ≤ liver | Complete response in favorable-risk HL (per RATHL) |
| 4 | Uptake moderately > liver | Partial metabolic response — incomplete |
| 5 | Markedly increased uptake | Progressive disease / significant residual tumor |
Interim PET in Hodgkin lymphoma: After 2 cycles of ABVD chemotherapy, Deauville 1–2 = favorable → bleomycin can be dropped (reducing pulmonary toxicity risk). Deauville 4–5 = inadequate response → escalate to BEACOPP or consider clinical trial. A complete metabolic response (Deauville 1–2) at end of all treatment is a strong predictor of durable remission — and a residual CT mass that is PET-negative is treated as scar, not viable tumor.
Solid tumors — PERCIST criteria: PET Response Criteria In Solid Tumors uses SULpeak (lean body mass-normalized SUV) to quantify response. A >30% decrease = partial metabolic response; complete normalization = complete metabolic response. PERCIST detects response earlier than RECIST size criteria.
PET Scan False Positives — What Can Look Like Cancer
Because FDG is taken up by any metabolically active cell — not just cancer — meaningful false-positive rates exist. Understanding the most common causes helps interpret results correctly.
- Infection and inflammation: Activated macrophages and neutrophils are FDG-avid. Sarcoidosis, histoplasmosis, tuberculosis — and post-biopsy, surgical, or healing wounds — produce FDG uptake that can mimic lymphoma or nodal metastases for weeks to months after the event.
- Brown adipose tissue (BAT): Cold temperatures activate BAT in the neck and supraclavicular regions, producing symmetric FDG uptake. Warming patients before FDG injection reduces this artifact.
- Physiologic bowel uptake: Variable FDG activity throughout the bowel is normal and can obscure peritoneal metastases.
- Thyroid: Diffuse thyroid uptake = thyroiditis; focal thyroid uptake may prompt ultrasound evaluation.
What to Expect During a PET Scan for Cancer
Preparation — Critical for Image Quality
- Fast ≥6 hours before the scan; water is encouraged
- Blood glucose target <200 mg/dL at time of FDG injection — high blood glucose competes with FDG for tumor uptake, reducing scan sensitivity
- Avoid vigorous exercise 24–48 hours before: Recently active muscles accumulate FDG and can mask or mimic pathology
- Diabetic patients: Coordinate insulin timing with the nuclear medicine team — usually short-acting insulin is held until after the scan
- No IV glucose-containing fluids before or during uptake
Day of the PET Scan
- IV placement and FDG injection — tiny volume, no taste or sensation
- 60-minute uptake phase: Rest quietly in a warm, dim room — avoid reading, talking, or moving. Movement = muscle uptake. Cold = brown fat activation. This period determines image quality.
- Scanning: 15–30 minutes whole-body. CT acquired in the same session for anatomic fusion.
- Total department time: 2–3 hours
Radiation and After the Scan
Total PET-CT radiation is approximately 14–25 mSv (FDG decay plus CT component). The F-18 tracer fully decays within ~10 hours — no prolonged radiation risk to family members. Drink plenty of fluids afterward to help flush the radiotracer through the kidneys. Results are typically available within 24–72 hours. If PET raises concerns about a specific finding, see our guide to MRI for cancer — often the next step for lesion characterization.
Frequently Asked Questions
What does a PET scan show that CT or MRI doesn’t?
A PET scan for cancer shows metabolic activity — how intensely cells are consuming glucose — rather than anatomy. This means PET can identify cancer in lymph nodes that appear normal size on CT (but are metabolically active), detect cancer spread earlier than CT, and distinguish viable tumor from scar tissue after treatment. According to the National Cancer Institute, PET reveals “biological information” that anatomic imaging alone cannot provide. PET is particularly powerful for lymphoma response assessment — treatment decisions are now guided by interim PET after just 2 cycles of chemotherapy, long before any size change would appear on CT.
How long does a PET scan for cancer take?
Total time in the nuclear medicine department is typically 2–3 hours. Most of this is the 60-minute FDG uptake period after injection, during which the patient rests quietly. The actual PET-CT scanning takes 15–30 minutes for a whole-body scan. Patients should plan for a half-day commitment. Preparation also begins the evening before: avoid strenuous exercise for 24–48 hours and fast for at least 6 hours before arrival.
Can a PET scan miss cancer?
Yes. PET misses cancers with low glucose metabolism — including low-grade neuroendocrine tumors, low-grade prostate cancer, mucinous tumors, and lobular breast cancer. PET also has limited sensitivity for lesions smaller than 8–10 mm. A negative FDG-PET does not rule out cancer in these settings — alternative tracers (PSMA-PET for prostate, DOTATATE-PET for NETs) or tissue biopsy may be needed. Additionally, elevated blood glucose at scan time (>200 mg/dL) significantly reduces FDG tumor uptake and can produce false-negative results — which is why strict fasting and glucose control before PET are essential.
What is PSMA-PET and how is it different from FDG-PET?
PSMA-PET uses a radiotracer targeting prostate-specific membrane antigen — a protein overexpressed on prostate cancer cells — rather than FDG (glucose). This makes PSMA-PET far more sensitive than FDG-PET for detecting prostate cancer, including at very low PSA levels after treatment. The FDA has approved two PSMA-PET agents: Ga-68 PSMA-11 (2020) and F-18 piflufolastat (2021). The ProPSMA trial (Lancet 2020) demonstrated 92% accuracy vs. 65% for conventional CT + bone scan in prostate cancer staging. FDG-PET is generally not useful for prostate cancer. See the ACS nuclear medicine scan overview for additional radiotracer types.
Does a PET scan hurt?
No. The injection is a standard IV insertion — no more uncomfortable than a blood draw. The radiotracer produces no sensation. The scan itself involves lying still on a narrow table in the scanner — there is no claustrophobia challenge comparable to MRI, as the PET-CT ring is much shorter. Patients with back pain may find the 15–30 minutes of lying still uncomfortable; discuss positioning options with the nuclear medicine team before the scan.
How many PET scans are safe per year?
There is no strict maximum, but PET-CT delivers meaningful radiation (14–25 mSv per scan), so frequency is determined by clinical need. For lymphoma patients in active treatment, interim PET after 2 cycles and end-of-treatment PET is standard — 2 scans per treatment course. Long-term surveillance PET scans are generally reserved for situations where CT alone or tumor markers raise suspicion of recurrence but CT is negative. The ordering physician weighs diagnostic benefit against cumulative radiation exposure for each patient individually.
Sources & Further Reading
- NCI — Nuclear Medicine Scans for Cancer
- American Cancer Society — Nuclear Medicine Scans
- Hofman MS et al. — ProPSMA Trial (PSMA-PET vs. conventional imaging), Lancet 2020
- Barrington SF et al. — Deauville criteria; Lugano Classification 2014
- Johnson PW et al. — RATHL trial (interim PET Hodgkin lymphoma), NEJM 2016
- Sartor O et al. — VISION Trial (Lu-177 PSMA-617), NEJM 2021
- Wahl RL et al. — PERCIST criteria, Journal of Nuclear Medicine 2009
This article is for educational purposes only and does not constitute medical advice. PET scan recommendations, preparation, and results should be discussed with your oncologist and nuclear medicine physician.