Approximately 40% of breast cancers are found by women themselves — as a new lump, a skin change, or another breast change noticed before any scheduled mammogram or clinical exam. The ability to recognize what to look for and act on it promptly is directly connected to outcomes: research consistently shows that women with greater breast cancer symptom awareness are more likely to present with earlier-stage disease (Forbes LJL et al., Lancet Oncol 2011 — the ABC study). Earlier stage at presentation means more treatment options and substantially better survival.
But most discussions of breast cancer symptoms start and end with “check for lumps” — leaving out most of the picture. Breast cancer symptoms are considerably more varied than a lump alone. Skin dimpling, nipple inversion, persistent unilateral breast pain, or a red, swollen breast without any palpable mass can all be breast cancer. One of the most dangerous breast cancer subtypes — inflammatory breast cancer — almost never presents as a palpable lump at all.
This guide covers all breast cancer symptoms — including the less-recognized ones — explains which breast changes are usually benign and which require prompt evaluation, and provides clear guidance on when to see a healthcare provider and how urgently.
The 8 Breast Cancer Warning Signs
Breast cancer symptoms extend well beyond a palpable lump. The following eight warning signs — recognized by the American Cancer Society, National Cancer Institute, and clinical oncology guidelines — each warrant prompt evaluation by a healthcare provider when new or persistent:
In the breast or underarm; hard, irregular, or fixed; painful or painless
New asymmetry or unilateral swelling of all or part of the breast
Visible pucker on breast skin; often easier to see with arms raised
Thick, pitted skin texture; caused by lymphatic obstruction
New inversion, spontaneous discharge (bloody or clear), or eczema-like scaling (Paget’s)
Rapid onset redness and warmth — cardinal sign of inflammatory breast cancer
Non-cyclic, focal, unilateral; does not change with the menstrual cycle
New lump or swelling in the underarm or collarbone area
Breast Lump — The Most Common Symptom
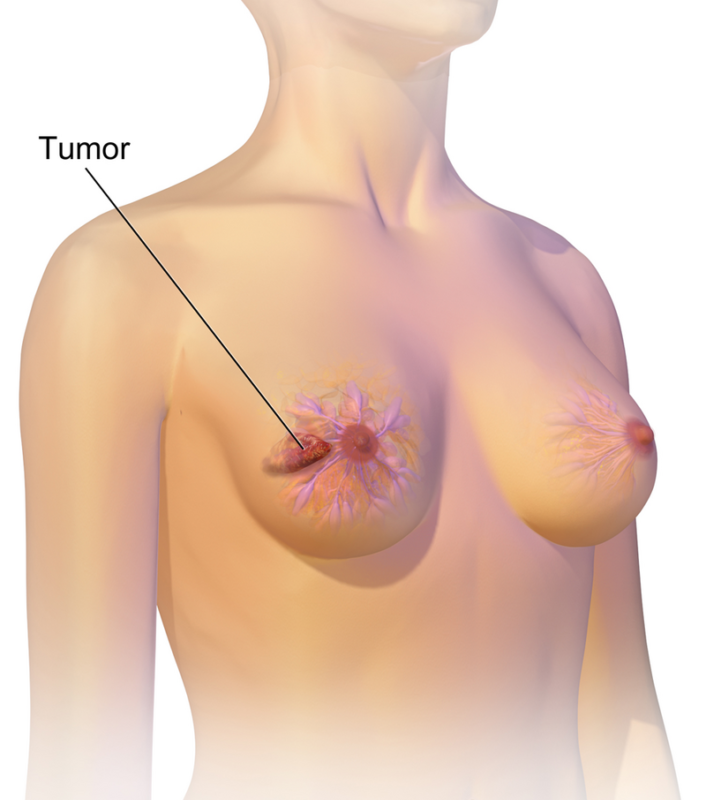
A new lump or mass in the breast or underarm is the most commonly recognized breast cancer symptom and the most common presenting finding of invasive breast cancer. Most breast cancers occur in the upper outer quadrant of the breast — the area closest to the armpit — though a cancer can develop anywhere in the breast.
What Distinguishes a Concerning Lump
Characteristics that raise clinical concern for malignancy include: hard or firm consistency; irregular, rough, or indistinct edges; fixed to surrounding tissue rather than freely mobile; does not change in size with the menstrual cycle. Benign lumps — such as fibroadenomas or cysts — tend to be smooth, round, mobile, and may be tender. However, no feature is definitive: the single most important principle is that no breast lump should be evaluated by feel at home and then dismissed. Any new breast lump requires professional evaluation with imaging.
A common misunderstanding: painful breast lumps are often assumed to be benign. Breast pain is more common with benign conditions, but breast cancer can present with a painful lump — approximately 10–20% of breast cancers are painful at presentation. A painful lump still requires evaluation.
Underarm lumps can represent enlarged lymph nodes from breast cancer spread — even without a palpable breast mass. Male breast cancer most commonly presents as a firm, painless lump under or near the nipple and is frequently diagnosed at a later stage because it is not commonly anticipated.
Nipple Symptoms — Discharge, Inversion, and Paget’s Disease
Nipple symptoms are among the breast cancer symptoms most likely to be overlooked or attributed to benign causes. Understanding which nipple changes are genuinely concerning helps prompt appropriate evaluation without unnecessary alarm about normal variation.
Nipple Discharge
Nipple discharge is common and most often benign. The characteristics that make discharge more likely to require evaluation for cancer:
- Unilateral: from one breast only
- Spontaneous: occurs without squeezing the nipple
- Bloody or clear/watery: as opposed to milky, green, or multi-colored
- From a single duct opening: rather than from multiple ducts across the nipple
- Persistent: does not resolve
- Not related to pregnancy or breastfeeding
Bloody nipple discharge always warrants evaluation — even though its most common cause (intraductal papilloma) is benign — because DCIS and intraductal carcinoma must be excluded. Milky bilateral discharge (galactorrhea) is almost always prolactin-related, not cancer.
Nipple Inversion
A nipple that was previously outwardly directed and has recently turned inward — particularly in one breast only — is clinically significant. Nipple retraction occurs when a cancer or its associated fibrosis tethers the underlying duct. Bilateral nipple inversion present since puberty that resolves with stimulation is almost always benign. The concerning pattern: unilateral, recently onset nipple inversion.
Paget’s Disease of the Nipple
Paget’s disease is a rare but frequently misdiagnosed form of breast cancer presenting as a persistent, sometimes itchy or burning eczema-like rash on the nipple and/or areola that may scale, crust, or ooze. It is commonly mistaken for eczema or contact dermatitis and sometimes treated with topical steroids for months before the correct diagnosis is made. The key distinguishing features: it is almost always unilateral, persistent, and does not respond to topical treatments as eczema does. Any eczema-like condition of the nipple that does not respond promptly to standard treatment or is unilateral and persistent should be biopsied. Paget’s disease is associated with underlying DCIS or invasive cancer in more than 90% of cases.
Skin Changes — Dimpling, Redness, and Orange-Peel Texture
Skin Dimpling
Skin dimpling — a visible pucker or depression on the breast surface — occurs when a tumor grows into and tethers Cooper’s ligaments, the fibrous bands anchoring breast tissue to the skin. It is most easily seen with the arms raised, which stretches the skin — a maneuver used in clinical breast examination. Dimpling can be present without a palpable lump; in some cases it is the first visible sign of a cancer too small to feel.
Orange-Peel Skin (Peau d’Orange)
Peau d’orange describes skin thickening with small pits at hair follicle openings — caused by cancer cells obstructing the superficial lymphatic channels under the skin. It is a cardinal sign of inflammatory breast cancer, but can also occur with locally advanced non-inflammatory cancer.
Swollen Lymph Nodes and Other Less-Known Signs
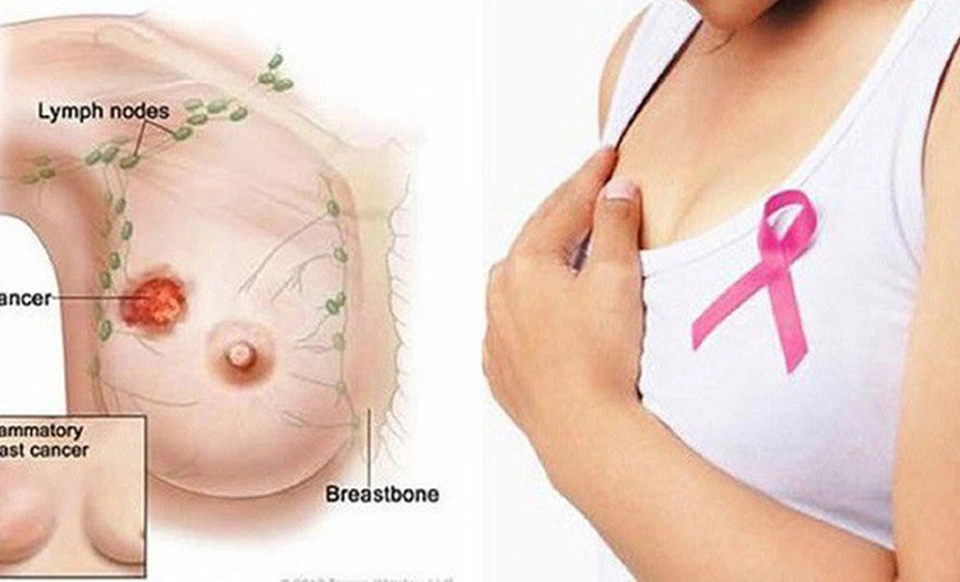
Swelling or a hard lump in the underarm can represent lymph node enlargement from breast cancer — even without any palpable breast mass. In some patients, axillary node involvement is the first clinical finding, with the primary tumor detected only on imaging. Lymph node swelling above the collarbone (supraclavicular) or below the collarbone (infraclavicular) is a concerning finding that may indicate Stage III or metastatic disease. Both invasive and inflammatory breast cancer can also cause general unilateral breast swelling without a distinct palpable mass.
Breast Changes That Are Usually NOT Breast Cancer
- Cyclic breast tenderness and swelling: before the menstrual period; improves afterward; bilateral; classic fibrocystic change — not cancer
- Bilateral diffuse lumpiness or ropiness: fibrocystic change; more prominent the week before menstruation
- Milky discharge from both breasts: galactorrhea; almost always benign and prolactin-related
- Cyclic breast pain: pain that clearly follows the menstrual cycle; almost always benign
- Soft, mobile, round cysts: benign fluid-filled sacs; diagnosed and monitored on ultrasound
Symptoms of Advanced Breast Cancer
When breast cancer has spread to distant organs, symptoms reflect the site of metastasis:
- Bone: persistent bone pain (back, hip, ribs, thigh); worsens progressively; may worsen at night; risk of pathologic fracture
- Liver: right upper abdominal pain; fatigue; nausea; jaundice; abdominal distension
- Lung: shortness of breath; persistent dry cough; chest pain
- Brain: persistent headache; visual changes; cognitive or personality changes; weakness; new-onset seizures
- Chest wall recurrence: new skin nodules along a mastectomy scar; worsening lymphedema
When to See a Doctor — and How Urgently
For any of the following, see a healthcare provider within days — not at the next scheduled annual appointment:
- A new lump, mass, or thickening in the breast or underarm
- New nipple discharge (unilateral, spontaneous, bloody, or clear/watery)
- A nipple that has recently changed from outward to inward
- Skin dimpling, puckering, or persistent skin changes
- Skin redness or warmth involving part or all of one breast
- Orange-peel skin texture (peau d’orange)
- Persistent eczema-like changes on the nipple or areola
- A new underarm lump or collarbone swelling
- Unexplained unilateral breast swelling or heaviness
None of these symptoms confirms a cancer diagnosis — many will have benign explanations. But they all require professional evaluation, not watchful waiting at home. For guidance on what to ask at your first appointment, see the cancer questions for doctor article. For a complete guide to breast cancer diagnosis and treatment, see the breast cancer overview article. For guidance on mammography and screening recommendations, see the breast cancer screening article.
Frequently Asked Questions
- Forbes LJL et al. — Differences in cancer awareness and beliefs between ethnic groups in the UK (ABC study); Lancet Oncol 2011
- Thomas DB et al. — Randomized trial of breast self-examination in Shanghai; J Natl Cancer Inst 2002
- Hance KW et al. — Trends in inflammatory breast carcinoma; J Natl Cancer Inst 2005
- American Cancer Society — cancer.org
- National Cancer Institute — cancer.gov/types/breast
This article is for educational purposes only and does not constitute medical advice. Any new or concerning breast symptom should be evaluated by a qualified healthcare provider promptly.
Breast Cancer Treatment: Key Advances and Approaches
Breast cancer treatment has become increasingly personalized over the past two decades, driven by advances in tumor biology characterization that distinguish meaningfully different breast cancer subtypes with different biological behaviors and optimal treatment approaches. The four major molecular subtypes of breast cancer — Luminal A (hormone receptor-positive, HER2-negative, low-grade), Luminal B (hormone receptor-positive, HER2-negative, high-grade or HER2-positive), HER2-enriched (HER2-positive, hormone receptor-negative), and triple-negative (estrogen receptor-negative, progesterone receptor-negative, HER2-negative) — each have distinct prognoses, responses to systemic therapy, and optimal treatment sequencing.
Hormone receptor-positive (HR+) breast cancer: HR+ breast cancer, which accounts for approximately 70% of cases, is treated with endocrine therapy (hormone-blocking treatment) as the cornerstone of systemic therapy. For premenopausal women, tamoxifen (5–10 years) or ovarian suppression plus an aromatase inhibitor is standard. For postmenopausal women, aromatase inhibitors (anastrozole, letrozole, exemestane) have superseded tamoxifen as the preferred endocrine therapy due to superior efficacy. In metastatic HR+ breast cancer, the CDK4/6 inhibitors (palbociclib, ribociclib, abemaciclib) combined with an aromatase inhibitor or fulvestrant have transformed outcomes: the MONARCH, PALOMA, and MONALEESA trials established this combination as first-line standard of care, substantially improving progression-free and overall survival compared to endocrine therapy alone.
HER2-positive breast cancer: HER2-positive breast cancer, which accounts for approximately 15–20% of cases, was once associated with a poor prognosis but is now one of the most treatable breast cancer subtypes due to the development of HER2-targeted therapies. Trastuzumab (Herceptin) was the first anti-HER2 agent and remains a cornerstone of treatment. For early-stage HER2-positive breast cancer, neoadjuvant pertuzumab + trastuzumab + chemotherapy followed by adjuvant T-DM1 (if residual disease) is standard, based on the APHINITY and KATHERINE trials. In metastatic HER2-positive disease, trastuzumab deruxtecan (T-DXd / Enhertu) has demonstrated remarkable efficacy even in patients who have progressed through multiple prior lines of HER2-directed therapy, with response rates exceeding 60% in heavily pretreated patients (DESTINY-Breast01/02/03 trials).
Triple-negative breast cancer (TNBC): TNBC — which accounts for approximately 10–15% of breast cancers and is disproportionately common in younger women and Black women — was historically treated with cytotoxic chemotherapy alone. Several advances have improved outcomes: pembrolizumab (Keytruda) added to neoadjuvant chemotherapy for early-stage, high-risk TNBC improved event-free survival in the KEYNOTE-522 trial and is now standard for eligible patients. Olaparib (for BRCA1/2 germline mutation carriers) and sacituzumab govitecan (Trodelvy, an antibody-drug conjugate targeting Trop-2) have improved outcomes in metastatic TNBC.
For authoritative information on breast cancer, the American Cancer Society’s breast cancer resource provides patient-friendly comprehensive guides. The National Cancer Institute’s breast cancer PDQ offers evidence-based clinical summaries. The NCCN Breast Cancer Guidelines are the most widely used clinical practice standards among U.S. oncologists. For information about breast cancer symptoms that often lead to initial evaluation, see our guide to breast cancer symptoms. For information about recommended breast cancer screening approaches — including mammography and supplemental MRI for high-risk women — see our comprehensive guide to breast cancer screening. For information about what a breast lump means and how it is evaluated, see our article on breast lumps.
Breast cancer survivorship — the period after completion of primary treatment — brings its own set of considerations. Long-term follow-up with an oncology team, adherence to prescribed adjuvant endocrine therapy (which may continue for 5–10 years for hormone receptor-positive breast cancer), monitoring for late effects of treatment (including bone loss from aromatase inhibitors, cardiac effects from anthracyclines or trastuzumab, and lymphedema from axillary surgery), and attention to lifestyle factors associated with reduced recurrence risk (physical activity, healthy weight maintenance, limiting alcohol) are all important components of survivorship care. Women with a personal history of breast cancer should continue annual mammography and, if high-risk, annual breast MRI. Discussing a personalized survivorship care plan with your oncology team helps ensure that surveillance, screening, and ongoing health needs are clearly defined after active treatment is complete.
Breast cancer is the most commonly diagnosed cancer in women in the United States (excluding skin cancers) and the second leading cause of cancer death in women, after lung cancer. Approximately 310,000 women and 2,800 men are diagnosed with invasive breast cancer each year in the United States. An additional 56,000 cases of ductal carcinoma in situ (DCIS), a non-invasive precursor, are diagnosed annually. Despite its frequency, breast cancer outcomes have improved substantially over the past three decades due to advances in early detection through mammography and improvements in systemic therapy. With early detection and appropriate treatment, the prognosis for breast cancer — particularly for hormone receptor-positive subtypes diagnosed at localized or regional stages — is excellent. The five-year relative survival for all stages combined exceeds 90%, and for localized disease approaches 100%. Continued investment in screening adherence, access to multidisciplinary oncology care, and clinical trial participation for eligible patients are the highest-priority strategies for further improving breast cancer outcomes at the population level.
Pingback: Nipple Discharge: Causes, When It Signals Cancer, and What to Do - Horizon Health Guide
Pingback: Breast Lump: Causes, When to Worry, and Next Steps - Horizon Health Guide