Lung cancer is the leading cause of cancer death in the United States, responsible for more deaths each year than breast, colorectal, and prostate cancer combined. What makes this particularly tragic is that lung cancer, when caught early, is often curable — the five-year survival rate for localized disease is approximately 61%, compared to just 6% for distant-stage disease. The problem is that only about 26% of lung cancers are diagnosed at a localized stage, because early-stage lung cancer causes no symptoms and most cases are found only after the disease has spread.
Lung cancer screening with low-dose computed tomography (LDCT) is the most effective intervention available for changing that statistic. Two landmark randomized controlled trials — the U.S. National Lung Screening Trial (NLST, 2011) and the European NELSON trial (2020) — demonstrated that annual LDCT lung cancer screening reduces lung cancer mortality by 20 to 33% in high-risk individuals. In 2021, the U.S. Preventive Services Task Force updated its lung cancer screening recommendation to expand eligibility to more current and former smokers.
This guide explains who qualifies for lung cancer screening, what the LDCT scan involves, how to understand Lung-RADS results, what happens when a nodule is found, and the full picture of benefits and harms.
Who Should Get Lung Cancer Screening?
Lung cancer screening with LDCT is recommended for individuals who are at high risk of developing the disease — primarily heavy current and former smokers within a specific age range. Three major organizations have published eligibility criteria; all share the same core requirements but differ slightly in age limits and additional factors.
USPSTF 2021 (U.S. Standard)
- Age 50–80 years
- ≥20 pack-years of smoking (1 pack/day × 20 years, or 2 packs/day × 10 years, etc.)
- Currently smoking OR quit within the past 15 years
- Annual LDCT recommended
Medicare / CMS (2022)
- Age 50–77 years
- ≥20 pack-years of smoking history
- Currently smoking or quit within 15 years
- Requires counseling visit before first screening
NCCN — Additional Risk Factors
- Age ≥50 + ≥20 pack-years PLUS any of:
- Radon or occupational carcinogen exposure
- Personal history of lung, lymphoma, or head/neck cancer
- Family history of lung cancer (first-degree relative)
- COPD or pulmonary fibrosis
Who Should NOT Be Screened
- Never-smokers or fewer than 20 pack-years
- Quit more than 15 years ago
- Under age 50
- Over 80 (USPSTF) or 77 (CMS)
- Serious comorbidities limiting life expectancy
- Would decline surgical treatment if cancer found
Why Chest X-Ray Doesn’t Work for Lung Cancer Screening
Two large trials — the PLCO Cancer Screening Trial and the Mayo Lung Project — found that annual chest X-ray did not reduce lung cancer mortality compared to usual care. The fundamental problem is sensitivity: chest X-ray misses approximately 50 to 75% of stage I lung cancers that are visible on CT. The U.S. Preventive Services Task Force explicitly recommends against lung cancer screening with chest X-ray. Only LDCT is recommended for eligible individuals.
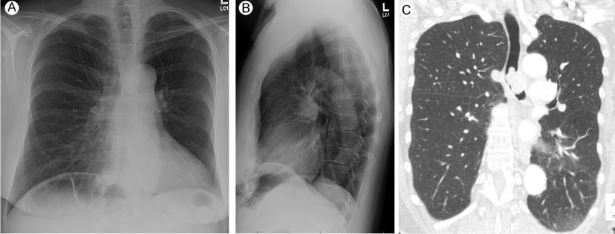
What the LDCT Scan Involves
Low-dose CT (LDCT) is a specific type of CT scan optimized to minimize radiation exposure while maintaining sufficient image quality to detect lung nodules. It is fast, non-invasive, and requires no preparation.
Radiation dose: An LDCT screening scan delivers approximately 1 to 1.5 millisieverts (mSv) — roughly equivalent to six months of natural background radiation from the environment. Standard diagnostic CT of the chest delivers approximately 7 mSv. The low dose is achievable because detecting lung nodules (which appear as bright spots against dark lung air) does not require the high image quality needed for other diagnostic purposes.
- 1 No preparation needed — no fasting, no contrast dye, no IV line is required before the scan.
- 2 Arrival and positioning — you lie on the CT table; a gown may be provided. The process is completely non-invasive.
- 3 The scan — the entire visit takes about 10 minutes. The actual image acquisition takes less than 30 seconds; you hold your breath briefly during this phase.
- 4 No discomfort — there is no injection, no noise beyond the CT machine hum, and no recovery period.
- 5 Results — a radiologist interprets the scan within a few days and sends results to your ordering clinician, who contacts you with findings and next steps.
LDCT lung cancer screening should be performed at an accredited lung cancer screening center. The American College of Radiology (ACR) accredits programs that use Lung-RADS reporting and maintain multidisciplinary teams to manage abnormal results — ask your provider for an ACR-accredited facility.
Understanding Your Lung-RADS Results
Lung-RADS (Lung Imaging Reporting and Data System) is the standardized reporting system developed by the American College of Radiology for LDCT lung cancer screening. Every accredited screening program uses Lung-RADS to categorize findings and assign a management recommendation. A result of 1 or 2 means your scan is essentially negative — you continue annual screening. A result of 3 or higher means follow-up is needed, but this is far more common than a cancer diagnosis.
| Category | Finding | Management |
|---|---|---|
| 1 — Negative | No nodules, or nodules with clearly benign calcification pattern | Annual LDCT in 12 months |
| 2 — Benign | Solid nodule <6mm; subsolid nodule with specific benign features | Annual LDCT in 12 months |
| 3 — Probably Benign | Solid nodule 6–7.9mm; partly solid or ground-glass nodule with specific features | 6-month follow-up LDCT |
| 4A — Suspicious | Solid nodule 8–14mm; partly solid nodule ≥8mm with solid component <8mm | 3-month follow-up LDCT or PET/CT |
| 4B — Very Suspicious | Solid nodule ≥15mm; partly solid nodule with solid component ≥8mm | PET/CT and/or tissue biopsy |
| 4X — Additional Concern | 4A or 4B nodule with additional suspicious features: spiculation, growth, upper lobe | PET/CT + tissue sampling |
Pulmonary Nodules — What Happens When Something Is Found
A pulmonary nodule is a small, round or oval spot in the lung. The vast majority of pulmonary nodules found on LDCT screening are benign — they represent old healed infections (histoplasmosis, tuberculosis), scars, lymph nodes, or areas of fibrosis. In the NLST, approximately 96% of positive screens were ultimately not cancer. With the Lung-RADS system (which uses larger size thresholds), the false positive rate drops to approximately 10 to 12%.
Size
The most important factor. Nodules under 6mm (solid) are almost always benign. The concern threshold begins at 6mm for solid nodules.
Density (Solid vs. Subsolid)
Solid nodules are more concerning than ground-glass or part-solid nodules. Ground-glass opacities grow very slowly and often represent early lepidic adenocarcinoma.
Shape and Edges
Spiculated (irregular, spiky) edges are more concerning than smooth round edges. Central, laminar, or “popcorn” calcification patterns are strongly benign.
Growth Rate
A nodule that doubles in volume in 20 to 400 days is concerning for malignancy. Very fast growth suggests infection; no growth over two years strongly suggests benign.
Location
Upper lobe nodules carry a higher malignancy rate than lower lobe nodules — a factor built into Lung-RADS 4X classification.
For most people, even a Lung-RADS 3 or 4A result leads to additional imaging — not biopsy. Only Lung-RADS 4B and 4X typically result in tissue sampling. Even among 4A findings, only about 5 to 15% ultimately prove to be cancer. A follow-up scan recommendation is not a cancer diagnosis. See our article on low dose CT lung cancer screening for more detail on what the scan involves and how nodules are managed.
Benefits and Harms of Lung Cancer Screening — The Full Picture
Lung cancer screening saves lives — the evidence from NLST and NELSON is clear. But like all cancer screening tests, it also carries harms. Truly informed decision-making requires understanding both sides. This is precisely why shared decision-making counseling is required before initiating screening.
Mortality Reduction
20% relative reduction in lung cancer deaths (NLST); up to 33% in women (NELSON). The most important benefit of screening.
Earlier-Stage Detection
Approximately 60–70% of screen-detected cancers are found at stage I, compared to ~26% without screening. Earlier stage = more treatment options.
Smoking Cessation Opportunity
The screening visit is a powerful moment for cessation counseling. Studies show screening programs improve quit rates — a secondary benefit with major long-term impact.
False Positives
96% of NLST positive screens were not cancer. With Lung-RADS, ~10–12% of individuals receive follow-up recommendations for benign findings. These cause anxiety and additional testing.
Invasive Procedures for Benign Findings
Approximately 1–2% of screened individuals undergo biopsy or surgery for a finding that ultimately proves benign. These procedures carry small but real complication risks.
Overdiagnosis
An estimated 3–18% of screen-detected cancers may never have caused symptoms in the patient’s lifetime. These patients receive treatment — surgery, radiation — that may not have been necessary.
When to Stop Lung Cancer Screening
Lung cancer screening should not continue indefinitely. Knowing when to stop is as important as knowing when to start. Continuing screening past appropriate stopping points adds radiation exposure and false positive risk without meaningful benefit.
- Quit more than 15 years ago — benefit from screening is substantially diminished for long-term former smokers
- Age over 80 (USPSTF) or 78 (CMS) — upper age limits where evidence of benefit is insufficient
- Significant comorbidities that limit life expectancy or make surgical treatment unsafe or unacceptable
- Would decline treatment even if cancer were found — screening provides no benefit if findings would not be acted upon
- Personal preference — after re-evaluation of preferences at any screening visit, patients may choose to stop
Frequently Asked Questions
Does lung cancer screening require a doctor’s referral?
Yes. A physician, nurse practitioner, or physician assistant order is required for insurance coverage. Medicare also requires a shared decision-making counseling visit before the first screening. This is not a test you can self-refer to and receive proper screening follow-up — the counseling, Lung-RADS reporting, and structured follow-up pathway are all part of what makes screening effective.
Will my health insurance cover lung cancer screening?
If you meet the USPSTF 2021 criteria (age 50–80, ≥20 pack-years, currently smoking or quit within 15 years), the Affordable Care Act requires most private insurance plans to cover annual LDCT screening with no cost-sharing. Medicare covers under the CMS 2022 criteria (age 50–77). Medicaid coverage varies by state. Contact your insurer directly to confirm coverage before scheduling.
What if my LDCT finds a nodule — does that mean I have lung cancer?
Almost certainly not. The vast majority of pulmonary nodules are benign. Even a Lung-RADS 4A result — considered suspicious — leads to a cancer diagnosis in only about 5 to 15% of cases. A follow-up scan recommendation is not a cancer diagnosis; it means the radiologist wants to watch a nodule over the next few months to see if it changes.
Should I still get screened if I’ve already quit smoking?
Yes, if you quit within the past 15 years and meet the age and pack-year criteria. Former smokers retain elevated lung cancer risk for years after quitting. The USPSTF specifically includes former smokers who quit within the past 15 years. Understanding how lung cancer and smoking are connected can help clarify why residual risk persists even after cessation.
Is there any preparation needed before the LDCT scan?
No. Unlike many other CT scans, LDCT for lung cancer screening requires no fasting, no contrast dye, and no IV line. You can eat, drink, and take your regular medications normally before the appointment. Just arrive at your scheduled time and wear comfortable clothing.
Sources
- NLST Research Team — Reduced lung-cancer mortality with low-dose computed tomographic screening; NEJM 2011;365:395–409
- de Koning HJ et al. — Reduced lung-cancer mortality with volume CT screening in a randomized trial (NELSON); NEJM 2020;382:503–513
- USPSTF — Lung cancer screening: recommendation statement; JAMA 2021;325(10):962–970
- CMS — Decision memo for screening for lung cancer with LDCT; 2022
- American College of Radiology — Lung-RADS Version 2022
- NCI SEER Program — Lung and bronchus cancer survival statistics
For information on what lung cancer symptoms look like before a screening diagnosis, see our related guide. If you are already undergoing screening, learn what low dose CT lung cancer screening involves in greater depth.