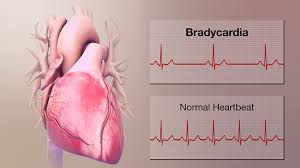
A slow heart rate — medically called bradycardia — is defined as a resting heart rate below 60 beats per minute. For many people, discovering a slow pulse triggers immediate concern about heart disease. Yet the clinical significance of bradycardia depends almost entirely on context: a resting heart rate of 48 beats per minute in a distance runner is a sign of excellent cardiovascular fitness, while the same rate in a 70-year-old experiencing dizziness and fatigue may indicate a failing conduction system. Understanding the range of causes — from normal physiologic variation to serious cardiac conditions — helps clarify when a slow heart rate warrants attention and when it can be safely ignored.
What Is a Slow Heart Rate?
The normal resting heart rate ranges from 60 to 100 beats per minute. Bradycardia is defined as any resting rate below 60 bpm. However, this threshold is a statistical convention, not a biological absolute. Many healthy individuals — particularly those who exercise regularly — have resting heart rates in the 50s or even the 40s without any underlying disease.
Clinically significant bradycardia typically refers to rates below 40 beats per minute, or any rate that is producing symptoms. Asymptomatic bradycardia in a healthy person almost never requires treatment. Symptomatic bradycardia — bradycardia that causes dizziness, fatigue, exercise intolerance, or syncope — requires evaluation regardless of the exact heart rate.
When a Slow Heart Rate Is Normal
The most common cause of a resting heart rate below 60 beats per minute is regular aerobic exercise. Trained athletes — runners, cyclists, swimmers, and other endurance athletes — develop what is called physiologic bradycardia through two complementary adaptations: increased vagal tone, which slows the sinoatrial (SA) node’s firing rate, and increased stroke volume, which means each heartbeat ejects more blood. Because the heart moves more blood per beat, it can maintain adequate cardiac output at a lower rate. Elite endurance athletes may have resting heart rates in the 30s to 40s — rates that in a non-athlete would represent serious cardiac disease.
During sleep, the heart rate naturally falls by 10 to 30 percent below the waking resting rate. Nocturnal bradycardia is entirely normal, even in non-athletes, and is driven by the parasympathetic nervous system’s dominance during sleep. Heart rates in the 40s during deep sleep are common and require no intervention.
Medications are a frequent and often intentional cause of bradycardia. Beta-blockers, non-dihydropyridine calcium channel blockers (diltiazem, verapamil), digoxin, ivabradine, and antiarrhythmic agents all lower heart rate as part of their therapeutic mechanism. A resting heart rate of 52 bpm in a patient on metoprolol for heart failure or hypertension is expected and appropriate — not a sign of drug toxicity or cardiac disease.
Sick Sinus Syndrome
Sick sinus syndrome (SSS) — also called sinoatrial node dysfunction — occurs when the SA node fails to generate impulses at an adequate rate or does so erratically. It is one of the most common causes of pathologic bradycardia in older adults, resulting from age-related fibrosis and degeneration of the SA node and surrounding atrial tissue.
SSS manifests in several ways: persistent inappropriate bradycardia, prolonged pauses between beats, and in some cases tachy-brady syndrome — alternating episodes of inappropriate tachycardia (often atrial fibrillation) and then abrupt bradycardia when the tachycardia terminates. Patients with SSS often describe episodes of palpitations followed by dizziness or near-fainting, as the heart pauses briefly after the fast rhythm stops. When SSS causes symptoms, permanent pacemaker implantation is the treatment of choice.
AV Block: Heart Block
Atrioventricular (AV) block refers to impaired conduction of electrical impulses from the atria to the ventricles through the AV node and His-Purkinje system. There are three degrees of AV block, each with different clinical significance.
First-degree AV block is characterized by a prolonged PR interval (greater than 200 milliseconds) on ECG, reflecting slowed but uninterrupted conduction. Every atrial impulse still reaches the ventricles. First-degree AV block is common, often found in athletes and elderly individuals, and is generally benign. It requires no treatment.
Second-degree AV block involves intermittent failure of AV conduction. Mobitz Type I (Wenckebach) shows progressively lengthening PR intervals until a beat is dropped, then the cycle repeats — this pattern reflects disease within the AV node and is generally benign, common in athletes and during sleep. Mobitz Type II shows sudden dropped beats without progressive PR prolongation, indicating disease below the AV node in the bundle of His or its branches. Mobitz II carries a significant risk of progression to complete heart block and usually requires permanent pacemaker implantation.
Third-degree (complete) AV block means no conduction whatsoever between atria and ventricles — they beat completely independently. The ventricles rely on a slow escape rhythm of only 20 to 40 beats per minute from below the block. Complete AV block causes significant hemodynamic compromise and requires permanent pacemaker implantation regardless of whether symptoms are present.
Medical Causes: Hypothyroidism, Electrolytes, and Other Conditions
Several systemic conditions cause bradycardia through non-structural mechanisms.
Hypothyroidism — deficiency of thyroid hormone — reduces the heart rate by decreasing the chronotropic effect of thyroid hormone on the SA node. Bradycardia in hypothyroidism is typically accompanied by other signs: fatigue, weight gain, cold intolerance, constipation, and dry skin. The diagnosis is confirmed by an elevated TSH and low free T4. Bradycardia resolves with appropriate thyroid hormone replacement.
Hyperkalemia — elevated serum potassium — impairs cardiac conduction by reducing the resting membrane potential in cardiac myocytes. Mild hyperkalemia produces peaked T waves on ECG; severe hyperkalemia causes widened QRS, AV block, bradycardia, and ultimately ventricular fibrillation or asystole. Hyperkalemia-induced bradycardia is a medical emergency.
Lyme carditis, caused by Borrelia burgdorferi infection, can cause AV block of any degree, typically presenting days to weeks after tick exposure. Heart block from Lyme carditis is usually reversible with appropriate antibiotic therapy; temporary pacemakers are occasionally required for high-degree block during treatment.
Obstructive sleep apnea causes nocturnal bradycardia and pauses during apneic episodes, driven by hypoxia-induced vagal activation. The bradycardia is typically intermittent and resolves with CPAP therapy. Elevated intracranial pressure can trigger the Cushing triad: bradycardia, hypertension, and irregular respirations — a neurosurgical emergency requiring immediate intervention.
Symptoms That Suggest Bradycardia Is Causing Problems
Symptomatic bradycardia may cause fatigue and exercise intolerance (reduced cardiac output at low heart rate limits oxygen delivery), dizziness or lightheadedness particularly with exertion or standing, syncope or presyncope, shortness of breath on exertion, chest discomfort, and cognitive slowing. The key distinguishing feature is whether symptoms correlate temporally with the slow heart rate. A Holter monitor that shows bradycardia at the same time the patient documents symptom episodes provides compelling evidence that the slow rate is causally responsible.
When Bradycardia Requires Treatment
The treatment decision for bradycardia is driven primarily by symptoms and by the specific conduction diagnosis. Asymptomatic bradycardia in athletes or young healthy individuals requires no treatment. Symptomatic bradycardia at any rate — any bradycardia causing syncope, presyncope, significant fatigue, or limiting daily activities — requires evaluation and typically treatment.
Drug-induced symptomatic bradycardia is managed by reducing the dose, switching to an alternative medication, or discontinuing the offending drug if clinically appropriate. Certain conduction diagnoses trigger treatment recommendations regardless of symptoms: Mobitz Type II AV block and third-degree AV block carry sufficient risk of hemodynamic deterioration that permanent pacemaker implantation is recommended for essentially all patients with these diagnoses.
Pacemaker Therapy for Bradycardia
When bradycardia requires treatment and reversible causes have been excluded or addressed, permanent pacemaker implantation is the definitive therapy. A pacemaker senses the heart’s native electrical activity and delivers a pacing impulse when the rate falls below the programmed minimum rate. Modern pacemakers are small devices implanted subcutaneously below the collarbone under local anesthesia — typically an outpatient procedure or requiring one night of observation.
Dual-chamber devices (DDD mode) pace both the right atrium and right ventricle, maintaining the normal sequence of atrial followed by ventricular activation. Rate-responsive pacemakers adjust the pacing rate based on physical activity, allowing appropriate heart rate acceleration during exercise. Newer leadless pacemakers — including the Micra device — are implanted directly into the right ventricle via a catheter through the femoral vein, eliminating the need for a traditional subcutaneous pocket and transvenous leads.
How Bradycardia Is Evaluated
The evaluation of a slow heart rate begins with a 12-lead ECG, which identifies the rhythm, PR interval length, and AV block type. When bradycardia is intermittent, ambulatory Holter monitoring (24 to 48 hours) or event recording (30 days) is used to capture the rhythm during symptom episodes. Blood tests — TSH for thyroid function, a basic metabolic panel for potassium — screen for reversible metabolic causes. An exercise stress test assesses for chronotropic incompetence — failure of the heart rate to increase appropriately with exercise, a hallmark of SSS. When pacemaker implantation is being considered, electrophysiology (EP) study can precisely characterize the level and severity of conduction disease.
For understanding normal heart rate ranges and what your resting rate means, see our article on what resting heart rate is. For the broader set of cardiovascular numbers worth tracking, see heart health numbers every adult should know. For palpitations that may accompany the fast episodes in tachy-brady syndrome, see our article on heart palpitations: common causes and warning signs.
The American Heart Association provides patient guidance on bradycardia and its management. The NIH National Heart, Lung, and Blood Institute explains the causes and treatment of slow heart rate. The CDC provides epidemiological information on arrhythmia as a cardiovascular condition.
A slow heart rate is not inherently dangerous. In athletes and during sleep, it reflects normal physiology. In older adults with symptoms or high-degree AV block, it may require definitive treatment with a pacemaker. The challenge is matching the clinical finding to its correct cause — and for that, a systematic evaluation is far more informative than the number on a pulse oximeter alone.
Vasovagal Syncope and Neurally Mediated Bradycardia
Not all bradycardia originates in the heart’s conduction system. Vasovagal syncope — the common faint — is caused by a reflex that briefly slows the heart rate (bradycardia) and dilates peripheral blood vessels (hypotension) simultaneously, temporarily reducing blood flow to the brain. Triggers include prolonged standing, heat exposure, pain, blood draws, emotional stress, and dehydration. The prodromal symptoms are well recognized: pallor, diaphoresis, nausea, and visual graying or tunneling that precede brief loss of consciousness.
Vasovagal syncope is benign — it causes no permanent cardiac damage and resolves spontaneously when the person lies flat. However, it can cause injuries from falls, and recurrent episodes significantly impact quality of life. Management includes identifying and avoiding triggers, increasing salt and fluid intake, performing physical counterpressure maneuvers (leg crossing, squatting, tensing the arms) at the onset of prodromal symptoms, and in refractory cases, medications such as fludrocortisone or midodrine. Pacemaker therapy is rarely used for vasovagal syncope because the mechanism involves both bradycardia and vasodilation — pacing alone does not fully address the hypotension component.
Carotid sinus hypersensitivity — an exaggerated reflex response to pressure on the carotid sinus in the neck — can cause abrupt bradycardia and syncope in older adults, sometimes triggered by collar pressure, head turning, or shaving. When diagnosed by carotid sinus massage during tilt table testing, dual-chamber pacemaker implantation substantially reduces syncope recurrence in those with a predominant cardioinhibitory (bradycardia-predominant) response.
Living With a Slow Heart Rate
For the majority of people who discover they have a slow heart rate — particularly those who are physically active and asymptomatic — no lifestyle modifications are required. A resting heart rate in the 50s is compatible with a long and healthy life and is simply a marker of cardiovascular conditioning. Annual monitoring with periodic ECG and evaluation of any new symptoms is appropriate for asymptomatic bradycardia.
For patients with pacemakers, activity restrictions are minimal. Most patients can return to their full range of activities within a few weeks of implantation. Contact sports that carry a risk of direct impact to the device pocket are generally restricted, but swimming, running, cycling, and most other activities are permitted. Modern pacemakers are designed to be MRI-conditional (most now carry formal MRI-conditional labeling), meaning MRI scans can be performed safely with appropriate programming precautions. The pacemaker battery lasts 8 to 15 years depending on how frequently it is used, and battery replacement is a simple outpatient procedure.
Frequently Asked Questions About Slow Heart Rate
Is a resting heart rate of 50 bpm dangerous?
In most cases, no. A resting heart rate of 50 bpm in an active adult is within the normal physiologic range and may simply reflect good cardiovascular fitness. It becomes concerning if it is accompanied by symptoms — dizziness, fatigue, near-fainting, or exercise intolerance — or if it occurs in a sedentary individual with no explanation. An ECG will quickly clarify whether the rate reflects sinus bradycardia (benign) or an AV block or SSS (potentially requiring treatment).
Can a slow heart rate cause a stroke?
Bradycardia itself does not directly cause stroke. However, tachy-brady syndrome associated with sick sinus syndrome includes periods of atrial fibrillation, which does carry stroke risk. Additionally, profound bradycardia can reduce cerebral perfusion and cause syncope. The key risk is whether AF is part of the picture — if so, anticoagulation considerations apply independent of the bradycardia management.
What heart rate is too slow to be safe?
There is no universal threshold, because individual tolerance varies considerably. Heart rates below 40 bpm in a symptomatic non-athlete represent significant hemodynamic compromise and generally require evaluation. The escape rate in complete AV block (20-40 bpm) is reliably symptomatic and dangerous. For athletes, rates well below 40 bpm may be asymptomatic and well-tolerated during sleep or rest.
Do I need a pacemaker for a slow heart rate?
A pacemaker is needed only for symptomatic bradycardia that cannot be corrected by addressing the underlying cause, or for specific high-risk conduction diagnoses (Mobitz II, complete AV block) even in the absence of symptoms. Most people with mildly slow heart rates — particularly athletes or patients on rate-lowering medications who are feeling well — do not need pacemakers. The decision is always individualized based on symptoms, rate, and the specific underlying mechanism.
Bradycardia in Special Populations
The significance of bradycardia varies considerably by age and clinical context. In children and adolescents, the normal resting heart rate is higher than in adults — neonates average 120 to 160 bpm, school-age children 70 to 110 bpm — so a rate below 60 bpm in a child who is not a trained athlete is more likely to represent pathology and should prompt evaluation. Congenital complete AV block, while rare, can present in childhood and requires pacemaker therapy.
In older adults over 70, the conduction system naturally undergoes fibrosis and slowing with age. First-degree AV block and right bundle branch block are increasingly common incidental ECG findings. SSS is predominantly a disease of older adults. The threshold for evaluation of new bradycardia is lower in this population because the risk of serious underlying conduction disease is higher, and the hemodynamic consequences of episodes of bradycardia (falls, syncope, injury) are more severe due to age-related impairment in blood pressure autoregulation.
In pregnancy, the normal resting heart rate actually increases by 10 to 20 bpm during the second and third trimesters due to increased blood volume and cardiac output demands. Bradycardia during pregnancy is unusual and should prompt evaluation of thyroid function, electrolytes, and fetal monitoring for any evidence of fetal heart rate abnormalities. Medication-induced bradycardia in pregnant patients may require switching to alternative agents that carry better pregnancy safety profiles.
In patients with heart failure, heart rate is a critical determinant of cardiac output. Unlike healthy individuals where stroke volume can increase to compensate for a slow heart rate, patients with severely impaired LV function have a fixed or near-fixed stroke volume — meaning cardiac output is more directly dependent on heart rate. Bradycardia in heart failure patients can precipitate decompensation, worsening congestion, and pulmonary edema. Rate-responsive pacemakers in this population help maintain appropriate heart rate during exertion, improving exercise capacity and quality of life.
For understanding what normal heart rates look like across different resting conditions, see our article on resting heart rate norms. For the full set of cardiovascular health numbers, see heart health numbers every adult should know. For the overlap between bradycardia and palpitation symptoms in tachy-brady syndrome, see heart palpitations: common causes and warning signs.
Understanding the Conduction System and Why It Slows
The heart’s electrical conduction system — from the sinoatrial node through the AV node, bundle of His, bundle branches, and Purkinje fibers — coordinates the orderly, top-to-bottom sequence of cardiac activation that makes the heart an efficient pump. Bradycardia arises when any part of this system generates impulses too slowly or fails to conduct them reliably to the ventricles.
Age-related changes are the most common underlying factor. The SA node and AV node accumulate fibrosis with age, and conduction velocity slows progressively over decades. This is why SSS and AV block are predominantly diseases of older adults. Ischemic heart disease — particularly inferior myocardial infarction, which involves the right coronary artery that supplies the AV node in the majority of individuals — can acutely damage the conduction system and produce temporary or permanent AV block. Infiltrative diseases such as cardiac sarcoidosis, amyloidosis, and hemochromatosis can deposit material in the conduction system, causing complete heart block even in younger patients.
This is why evaluation of bradycardia in younger patients, or bradycardia that develops abruptly without medication changes, warrants a broader workup that includes inflammatory markers, cardiac imaging, and sometimes cardiac MRI — not just the basic ECG and metabolic panel that would be appropriate for age-related conduction slowing in an older adult. Identifying a treatable cause like sarcoidosis or Lyme disease before pacemaker implantation is always preferable, as treatment of the underlying condition may resolve the bradycardia without the need for a permanent device.
The trajectory of conduction disease also matters for long-term planning. A patient with asymptomatic first-degree AV block at age 50 has a modestly elevated risk of developing higher-degree block over the following decades. Periodic ECG monitoring — every one to two years — allows detection of progression before a symptomatic event occurs. Patients who develop new Mobitz I block in the context of inferior MI often recover normal conduction as the ischemia resolves; temporary pacing is available if the block produces hemodynamic compromise during the recovery period. These nuances — the trajectory, the context, the underlying mechanism — are why the management of bradycardia is always individualized rather than applied by a simple rule based on the heart rate number alone.