Sleep Apnea and Heart Disease

You stop breathing hundreds of times per night — and you don’t know it. This is the fundamental reality of obstructive sleep apnea (OSA): a condition in which the airway collapses repeatedly during sleep, producing episodic cessation of breathing that triggers a cascade of cardiovascular stress responses, then resolves as breathing briefly resumes, then recurs — dozens to hundreds of times per night, every night, for years before most patients are diagnosed.
The connection between sleep apnea and heart disease has moved from clinical observation to one of the most important emerging areas in cardiovascular medicine. OSA is estimated to affect 26 to 34 percent of middle-aged men and 17 to 28 percent of middle-aged women — making it one of the most prevalent medical conditions in adults. Yet approximately 80 percent of those affected remain undiagnosed, making untreated sleep apnea one of the largest unaddressed cardiovascular risk burdens in the healthcare system.
What Happens Cardiovascularly During an Apneic Episode
Each obstructive apnea follows a predictable physiological sequence that amounts to a brief but intense cardiovascular stress event. Understanding this sequence explains why untreated OSA causes the specific cardiovascular complications it does.
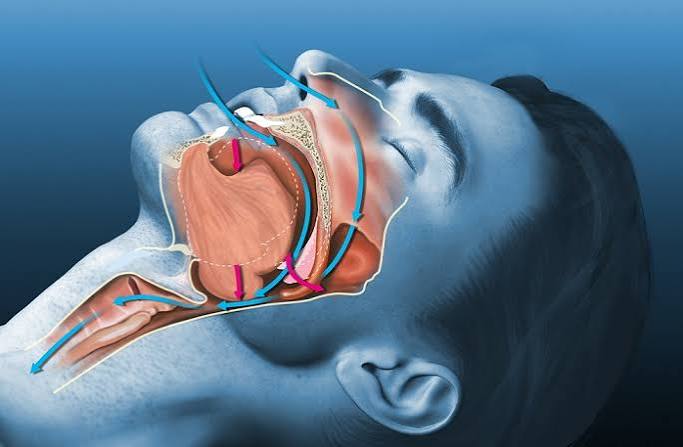
The episode begins when the upper airway musculature relaxes during sleep, allowing the tongue, soft palate, and pharyngeal walls to collapse against each other, obstructing airflow. Breathing effort against the closed airway continues — the chest and diaphragm strain against obstruction — but no air moves. Oxygen saturation in the blood begins to fall. Carbon dioxide accumulates.
As hypoxia worsens and CO₂ rises, chemoreceptors in the carotid bodies and brainstem detect the disruption and activate a powerful sympathetic response. Epinephrine and norepinephrine surge. Heart rate spikes. Blood pressure rises acutely — often to 200/110 mmHg or higher during severe apneic episodes, even in patients who have normal daytime blood pressure. This nocturnal blood pressure surge represents the endothelium experiencing repeated hypertensive stress that persists throughout the sleeping hours.
The sympathetic surge also arouses the sleeper — typically not to full wakefulness but to a brief lightening of sleep that restores airway muscle tone, terminates the apnea, allows breathing to resume, and then permits the patient to fall back asleep before repeating the cycle. This arousal is typically not remembered, explaining why many OSA patients are unaware of their breathing disruptions despite experiencing hundreds per night.
The cumulative cardiovascular effect of these repeated events — each producing acute hypertension, hypoxia, oxidative stress, sympathetic activation, and inflammatory signaling — is substantial and well-documented. The heart, arteries, and autonomic nervous system experience a compressed version of every cardiovascular stressor simultaneously, hundreds of times nightly, for years.
OSA as the Most Common Cause of Treatment-Resistant Hypertension
Hypertension is classified as treatment-resistant when blood pressure remains above goal despite the concurrent use of three or more antihypertensive medications at optimal doses, including a diuretic. Treatment-resistant hypertension affects approximately 10 to 15 percent of hypertensive adults and carries substantially higher cardiovascular event rates than controlled hypertension.
Obstructive sleep apnea is the single most common identifiable cause of treatment-resistant hypertension, present in 50 to 80 percent of patients with treatment-resistant hypertension in clinical series. The mechanism is straightforward: each nocturnal sympathetic surge from OSA elevates vascular tone and activates the renin-angiotensin-aldosterone system, causing sodium retention and volume expansion. Antihypertensive medications that work through sympatholytic or vasodilatory mechanisms face continuous reactivation of these pressure-raising systems every night — making it biologically predictable that pharmacotherapy alone would be insufficient without addressing the underlying sleep-disordered breathing.
The diagnostic implication: any patient with hypertension that is poorly controlled despite adequate medication compliance should be systematically evaluated for obstructive sleep apnea. The absence of classic symptoms (witnessed apneas, excessive daytime sleepiness, loud snoring) does not exclude OSA — particularly in women, who frequently present with atypical symptoms including morning headaches, insomnia, and mood disturbance rather than the classic presentation more common in men.
Sleep Apnea and Atrial Fibrillation — A Bidirectional Relationship
The relationship between obstructive sleep apnea and atrial fibrillation (AFib) is one of the most clinically important associations in cardiovascular sleep medicine, with evidence of causation in both directions and substantial implications for AFib management.
OSA raises atrial fibrillation risk through multiple mechanisms. The acute surges in intrathoracic pressure during obstructive apneas (as the chest strains against a closed airway) stretch the atrial walls, promoting atrial enlargement and electrical remodeling. Nocturnal hypoxia and the associated sympathetic surges create the electrophysiological environment for abnormal impulse generation and re-entry — the substrates for AFib initiation. Inflammatory markers elevated by OSA promote atrial fibrosis, which provides the anatomical substrate for sustained AFib. Multiple large studies show OSA is associated with 2 to 4 times the risk of AFib development.
The bidirectional aspect: AFib itself worsens sleep apnea. The fluid redistribution caused by atrial enlargement and elevated cardiac filling pressures in AFib causes fluid to accumulate in the neck and pharyngeal tissues during sleep, narrowing the upper airway and predisposing to obstruction. This creates a vicious cycle in which OSA promotes AFib, and AFib worsens the nocturnal obstruction that drives further AFib risk.
Critically, untreated OSA substantially reduces the effectiveness of AFib treatment. AFib recurrence after catheter ablation — the most effective rhythm control strategy — is significantly higher in patients with untreated OSA compared to those on CPAP therapy. Multiple studies show CPAP therapy reduces AFib recurrence risk after ablation by 40 to 60 percent. The Heart Rhythm Society now recommends OSA evaluation and treatment as part of comprehensive AFib management — not as ancillary background care but as a direct modifier of arrhythmia burden and treatment response.
Sleep Apnea, Heart Failure, and Coronary Artery Disease
OSA is associated with elevated risks of both heart failure and coronary artery disease, through mechanisms that extend beyond its hypertension and atrial fibrillation effects.
In coronary artery disease, the nocturnal hypoxia of OSA creates a demanding myocardial oxygen environment at precisely the time when the cardiovascular system should be recovering. Healthy sleep — particularly non-REM deep sleep — is associated with the lowest heart rates, blood pressures, and sympathetic tone of the 24-hour cycle, allowing the heart to “rest” and recover from daytime cardiovascular demands. OSA disrupts this recovery window, replacing it with repeated hypoxic and hemodynamic stress. Ischemic events, silent MI, and sudden cardiac death show nocturnal peaks that are particularly pronounced in OSA patients, consistent with nighttime cardiovascular stress rather than normal circadian rest.
Heart failure and OSA interact through both obstructive and central sleep apnea mechanisms. In obstructive sleep apnea, the cardiovascular consequences described above — hypertension, AFib, systemic inflammation — all accelerate heart failure development and worsen existing heart failure. Once heart failure is established, a distinct form of sleep-disordered breathing — central sleep apnea with Cheyne-Stokes respiration — often emerges. Central sleep apnea in heart failure reflects the oscillating drive to breathe produced by periodic fluid redistribution and chemoreceptor hyperresponsiveness, and is associated with worse heart failure prognosis. Adaptive servo-ventilation (ASV) — a more advanced form of positive airway pressure therapy — has been evaluated for central sleep apnea in heart failure, though results have been mixed (the SERVE-HF trial found increased mortality with ASV in heart failure with reduced ejection fraction, making patient selection critical).
Diagnosing Sleep Apnea — Who Should Be Evaluated and How
Diagnosis of obstructive sleep apnea requires objective sleep testing — clinical symptoms alone cannot reliably identify or exclude OSA. The two main diagnostic approaches are:
In-laboratory polysomnography (PSG) is the gold standard: a comprehensive overnight sleep study measuring airflow, respiratory effort, oxygen saturation, EEG brain activity, EMG muscle activity, and cardiac rhythm simultaneously. PSG provides the most complete characterization of sleep architecture and respiratory events and is preferred when the clinical picture is complex, when central sleep apnea is suspected, or when prior home testing has been inconclusive.
Home sleep apnea testing (HSAT) uses a simplified portable device to measure airflow, respiratory effort, and oxygen saturation during sleep at home. HSAT is appropriate for patients with a moderate to high pre-test probability of moderate to severe OSA without significant comorbidities. It is less sensitive than PSG and may miss mild OSA or central sleep apnea, but it is substantially more convenient and accessible, reducing the barrier to diagnosis for many patients.
Validated screening questionnaires — including the STOP-BANG questionnaire (Snoring, Tiredness, Observed apnea, Pressure/hypertension, BMI, Age, Neck circumference, Gender) — can identify patients at high pre-test probability who should proceed to formal sleep testing. A STOP-BANG score of 5 to 8 indicates high risk with a sensitivity of approximately 90 percent for moderate to severe OSA. Referral for sleep evaluation is appropriate for patients with treatment-resistant hypertension, atrial fibrillation, unexplained right heart disease, excessive daytime sleepiness, or typical symptoms (loud snoring, witnessed apneas, morning headaches) regardless of STOP-BANG score.
CPAP and Cardiovascular Outcomes — What the Evidence Shows
Continuous positive airway pressure (CPAP) therapy — which splints the upper airway open during sleep by delivering a stream of air at a pressure sufficient to prevent collapse — is the first-line treatment for moderate to severe OSA and definitively eliminates the apneic events and their acute cardiovascular consequences.
CPAP therapy reliably improves cardiovascular surrogate endpoints: daytime blood pressure is reduced by 2 to 4 mmHg on average in unselected OSA patients and by 6 to 8 mmHg in those with treatment-resistant hypertension. Nighttime blood pressure surges are dramatically reduced. Atrial fibrillation recurrence after ablation is substantially lower in CPAP-adherent patients. Inflammatory markers and oxidative stress markers decline. Heart rate variability improves.
However, the two largest randomized controlled trials of CPAP for cardiovascular event prevention in OSA — the SAVE trial and the ISAACC trial — did not demonstrate statistically significant reductions in major cardiovascular events with CPAP in patients with established cardiovascular disease. This finding has been attributed primarily to the low CPAP adherence achieved in these trials (average 3 to 4 hours per night, versus the 6+ hours associated with benefit in observational studies) and to the relatively high baseline treatment these patients were already receiving. Observational data from adherent CPAP users consistently show cardiovascular mortality benefits, and the mechanistic evidence for cardiovascular harm from untreated OSA is unambiguous.
The American Heart Association provides information on sleep disorders and cardiovascular health. The Centers for Disease Control and Prevention maintains sleep health data and resources. The National Heart, Lung, and Blood Institute offers patient education on sleep apnea, diagnosis, and treatment.
Related reading: What Causes Heart Disease? | Major Risk Factors for Heart Disease | Chronic Stress and Heart Disease | Obesity and Heart Health | Heart Attack Prevention
Sources
- Peppard PE, et al. Prospective Study of the Association between Sleep-Disordered Breathing and Hypertension. N Engl J Med. 2000;342(19):1378-1384.
- Gami AS, et al. Association of atrial fibrillation and obstructive sleep apnea. Circulation. 2004;110(4):364-367.
- McEvoy RD, et al. CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea (SAVE Trial). N Engl J Med. 2016;375(10):919-931.
- Abe H, et al. Effect of CPAP on Atrial Fibrillation Recurrence After Ablation. Eur Heart J. 2010;31(24):2977-2985.
- Drager LF, et al. Obstructive Sleep Apnea and Cardiovascular Disease: Lessons from Recent Trials and Need for Team Science. Circulation. 2017;136(19):1840-1850.
- Cowie MR, et al. Adaptive Servo-Ventilation for Central Sleep Apnea in Systolic Heart Failure (SERVE-HF). N Engl J Med. 2015;373(12):1095-1105.
OSA Severity Classification and Corresponding Cardiovascular Risk
Obstructive sleep apnea severity is classified by the apnea-hypopnea index (AHI) — the number of complete apneas plus partial flow reductions (hypopneas) per hour of sleep. This classification system, while imperfect, provides a clinically useful framework for understanding cardiovascular risk gradients in OSA.
Mild OSA is defined as an AHI of 5 to 14 events per hour. At this level, cardiovascular risk is modestly elevated, particularly for hypertension, but the absolute risk increase is relatively small. Daytime symptoms (sleepiness, impaired cognition) are often minimal or absent in mild OSA, which contributes to underdiagnosis and undertreated cases. Treatment decisions in mild OSA depend primarily on symptom burden: highly symptomatic patients typically benefit from CPAP, while asymptomatic patients may be managed with lifestyle interventions (weight loss, positional therapy, alcohol avoidance before sleep) and monitoring.
Moderate OSA is defined as an AHI of 15 to 29 events per hour. Cardiovascular consequences become substantially more apparent at this level. Blood pressure is significantly affected, hypertension is common, and the risk of atrial fibrillation and nocturnal cardiac events is clearly elevated above population baselines. CPAP therapy is generally recommended for moderate OSA regardless of symptom level when cardiovascular risk factors are present, and is particularly important in patients with established cardiovascular disease, treatment-resistant hypertension, or atrial fibrillation.
Severe OSA is defined as an AHI of 30 or more events per hour — with some patients experiencing 60 to 100 or more apneic events per hour. At this severity level, the cumulative nightly cardiovascular stress is enormous: a patient with an AHI of 60 experiences over 400 complete or near-complete airway obstructions per 7-hour sleep period, each producing hypoxia, blood pressure surges, and sympathetic activation. Severe OSA is strongly and independently associated with hypertension, atrial fibrillation, coronary artery disease, heart failure, stroke, and cardiovascular mortality. CPAP therapy is unequivocally indicated. Severe OSA that goes untreated for years represents one of the most significant modifiable cardiovascular risk burdens that patients and clinicians overlook.
The AHI alone, however, incompletely characterizes OSA cardiovascular risk. The oxygen desaturation index (ODI) — how far and how often oxygen saturation drops during sleep — and sleep architecture disruption (loss of restorative slow-wave sleep and REM sleep) contribute independently to cardiovascular consequences. Patients with the same AHI but deeper or longer desaturations face greater hypoxic cardiac stress. This is why sleep study interpretation should consider multiple parameters beyond AHI alone, and why severe oxygen desaturation on sleep testing deserves particularly aggressive treatment.
Treatment Options Beyond CPAP — When Patients Cannot Tolerate Positive Airway Pressure
While CPAP therapy is the most effective available treatment for moderate to severe obstructive sleep apnea, adherence remains a significant clinical challenge. Approximately 30 to 50 percent of CPAP-prescribed patients are non-adherent at 12 months, using the device fewer than 4 hours per night on fewer than 5 nights per week — the threshold typically used in clinical trials to define adequate adherence. Claustrophobia, mask discomfort, pressure intolerance, nasal dryness, and partner disturbance all contribute to non-adherence. For patients who genuinely cannot tolerate CPAP, several alternative therapies offer meaningful cardiovascular protection:
Mandibular advancement devices (MADs) are custom-fitted oral appliances worn during sleep that advance the lower jaw forward, increasing the posterior airway space and reducing upper airway collapsibility. MADs are less effective than CPAP in reducing AHI — typically producing 50 to 60 percent AHI reduction versus 90 to 95 percent with CPAP — but in patients who cannot tolerate CPAP, the cardiovascular benefit from MAD use is real. Studies comparing CPAP and MAD in mild to moderate OSA suggest similar blood pressure reductions when both are used consistently, because adherence to MADs is typically higher than adherence to CPAP. MADs are most effective in mild to moderate OSA and in patients with positional OSA (predominantly supine-dependent).
Hypoglossal nerve stimulation (HNS) — marketed as Inspire therapy in the United States — is an implanted device approved by the FDA for moderate to severe OSA in patients who cannot tolerate CPAP and meet specific anatomical criteria. The device stimulates the hypoglossal nerve (which controls tongue movement) in synchrony with breathing, preventing the tongue from falling back during sleep. Clinical trial data from the STAR trial and its extended follow-up showed substantial AHI reductions (from approximately 29 to 9 events per hour) sustained over 5 years, with high patient satisfaction and CPAP-comparable cardiovascular improvements. HNS is appropriate for carefully selected patients (BMI under 32, specific airway anatomy confirmed on drug-induced sleep endoscopy, no complete concentric collapse at the velum).
Positional therapy is effective for patients whose OSA is predominantly or exclusively positional — occurring primarily in the supine (back-sleeping) position. Approximately 50 to 60 percent of OSA patients have a supine AHI more than double their non-supine AHI, qualifying as positional OSA. Avoiding supine sleep using positional devices (vibrating alarm sensors, positional pillows, or backpack-mounted foam that makes supine sleeping uncomfortable) can normalize or dramatically reduce AHI in these patients. While evidence for long-term cardiovascular outcomes is more limited than for CPAP, positional therapy is an important adjunctive or alternative treatment for appropriately selected positional OSA patients.
Upper airway surgery — including uvulopalatopharyngoplasty (UPPP), tongue base reduction, and multi-level palatal procedures — has a role in select patients, though success rates are lower than CPAP and patient selection is demanding. The best surgical outcomes occur in younger patients with moderate rather than severe OSA, specific anatomical findings (large tonsils, redundant palatal tissue), and an absence of obesity. Emerging surgical techniques including transoral robotic surgery (TORS) for tongue base reduction show promise in carefully selected patients.
Sleep Apnea in Special Populations — Women, Older Adults, and Established Cardiovascular Disease
OSA in women is systematically underdiagnosed because women with OSA present differently from the classic male phenotype that drove early OSA characterization. Men with OSA typically present with loud snoring, witnessed apneas, excessive daytime sleepiness, and obesity — features that prompted the development of screening tools like STOP-BANG. Women with OSA more frequently present with insomnia, fatigue, morning headaches, mood disturbance, and depression, without classical snoring or witnessed apneas. They also tend to have lower AHI values for equivalent symptom burden. The consequence is that women are significantly less likely to be referred for sleep testing and less likely to receive an OSA diagnosis — despite the fact that postmenopausal women have nearly the same OSA prevalence as men. The cardiovascular implication is substantial: women with undiagnosed OSA are carrying cardiovascular risk from untreated sleep-disordered breathing while their symptoms are attributed to anxiety, depression, thyroid disease, or menopausal transition.
OSA in older adults occurs at much higher prevalence than in younger populations — estimated to affect 40 to 70 percent of adults over age 65 when assessed by standard polysomnography. Complicating the clinical picture is that older adults typically have lower baseline levels of daytime sleepiness than younger OSA patients despite equivalent AHI, partly due to reduced sleep drive and partly due to comorbid conditions that may independently cause fatigue. The cardiovascular consequences of OSA in older adults are compounded by the independently higher cardiovascular baseline risk in this age group. CPAP therapy is effective and beneficial in older adults who can adhere to it. Adherence may be affected by cognitive impairment, arthritis limiting mask manipulation, and caregiver availability — making therapy initiation and support particularly important in this population.
OSA in patients with established cardiovascular disease requires integrated management across cardiology and sleep medicine. In patients who have already experienced a myocardial infarction, stroke, or AFib, OSA is both a contributor to recurrence risk and a target for reducing that risk. Cardiology guidelines from the American Heart Association and European Society of Cardiology increasingly include OSA screening as part of secondary cardiovascular prevention, recognizing that treating a 50 to 80 percent AHI contributor in a treatment-resistant hypertensive patient with prior MI is as important as optimizing beta-blocker dosing. Collaborative cardiac-sleep care models — in which sleep study referral and CPAP follow-up are integrated into cardiac rehabilitation and secondary prevention programs — represent the emerging standard for comprehensive cardiovascular risk reduction in this population.