Atrial Fibrillation: Symptoms and Risks
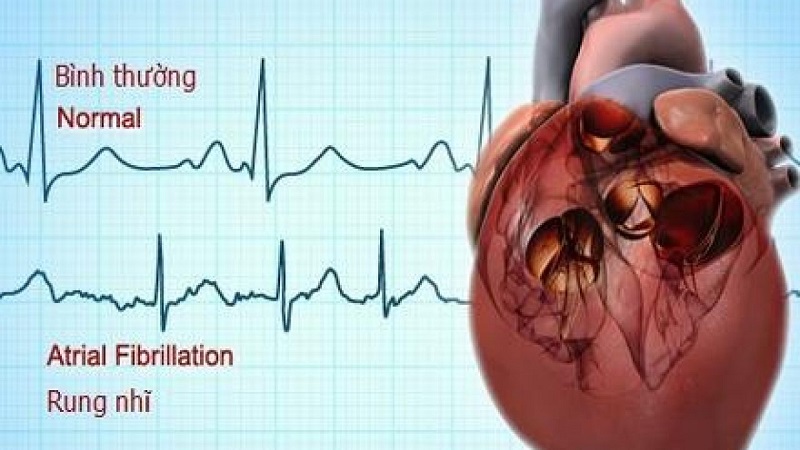
Atrial fibrillation (AFib) is the most common sustained cardiac arrhythmia, affecting approximately 33 to 40 million people worldwide and 6 to 7 million Americans. It is a condition in which the heart’s upper chambers — the atria — fire electrical impulses chaotically and rapidly (300 to 600 impulses per minute) rather than in the coordinated, rhythmic fashion that drives normal sinus rhythm. Instead of contracting efficiently to push blood into the ventricles, the fibrillating atria quiver uselessly, while the ventricles respond irregularly as they receive only a fraction of the atrial impulses conducted through the atrioventricular (AV) node. The result is the defining characteristic of AFib: an irregularly irregular heartbeat with no predictable pattern to the interval between beats.
Atrial fibrillation is important not primarily because of the irregularity itself — many patients tolerate the rhythm with minimal symptoms — but because of two serious consequences it produces: hemodynamic impairment from the loss of effective atrial contraction and the rapid, irregular ventricular rate (which can produce or worsen heart failure), and stroke. AFib increases the risk of stroke fivefold compared to individuals in normal sinus rhythm, and AFib-related strokes are typically larger, more disabling, and carry higher short-term mortality than strokes from other causes. These risks make AFib a major cardiovascular priority and the driver of one of the most consequential treatment decisions in cardiology: anticoagulation therapy to prevent thrombus formation and cardioembolic stroke.
Types of Atrial Fibrillation — The Clinical Patterns
Atrial fibrillation is classified by its temporal pattern, which reflects underlying atrial pathology and guides treatment decisions:
Paroxysmal AFib — episodes that start spontaneously and terminate on their own, typically within 7 days (usually within 24 to 48 hours). Between episodes, the patient is in normal sinus rhythm. Paroxysmal AFib can range from rare, brief episodes (lasting minutes) to frequent, longer episodes (lasting hours to days). Even brief paroxysmal episodes carry stroke risk proportional to overall AFib burden, and the paroxysmal pattern does not reduce anticoagulation indications in high-risk patients.
Persistent AFib — episodes lasting more than 7 days that do not terminate spontaneously. Persistent AFib requires either pharmacological cardioversion (IV antiarrhythmic drugs) or electrical cardioversion (a synchronized DC shock delivered under sedation) to restore normal sinus rhythm. Restoration of sinus rhythm in persistent AFib is followed by antiarrhythmic drug therapy and/or catheter ablation to maintain sinus rhythm and prevent recurrence.
Long-standing persistent AFib — continuous AFib lasting more than 12 months. At this stage, atrial remodeling (progressive fibrosis, enlargement, and electrical changes) has advanced substantially, reducing the likelihood of durable sinus rhythm restoration with cardioversion or ablation alone.
Permanent AFib — AFib in which the physician and patient have jointly decided not to pursue further rhythm restoration attempts, accepting AFib as the ongoing rhythm and focusing management on rate control and anticoagulation rather than rhythm control. “Permanent” is a treatment strategy decision, not a description of atrial anatomy — it can be revised if circumstances or patient preferences change.
Symptoms of Atrial Fibrillation — What AFib Feels Like
Atrial fibrillation symptoms vary dramatically among patients — from completely asymptomatic (discovered incidentally on ECG or cardiac monitoring) to severely symptomatic with significantly impaired quality of life. The wide symptom range reflects differences in ventricular rate during AFib (faster rates produce more symptoms), the presence and severity of underlying heart disease, and individual sensitivity to rhythm irregularity.
Palpitations — the sensation of an irregular, rapid, or pounding heartbeat — are the most common AFib symptom, reported by 50 to 70 percent of symptomatic patients. Patients describe feeling their heart “flutter,” “race,” “skip beats,” or beat “erratically.” Palpitations may be continuous during AFib episodes or intermittent within episodes, and their presence correlates poorly with AFib severity or stroke risk — some patients with dangerous AFib are symptom-free while others with paroxysmal AFib have disabling palpitation symptoms with each brief episode.
Dyspnea (shortness of breath) occurs because the loss of effective atrial contraction (“atrial kick”) reduces cardiac output by 15 to 30 percent, and the rapid ventricular rate further limits diastolic filling time, reducing stroke volume. In patients with underlying cardiac disease (hypertension, coronary artery disease, heart failure, valve disease), the hemodynamic impact of AFib onset can be severe, precipitating acute pulmonary congestion. Exertional dyspnea during AFib may be the primary complaint in patients with poor rate control during activity.
Fatigue and reduced exercise tolerance are common AFib symptoms reflecting both reduced cardiac output and, in patients with tachycardia-mediated rate effects, the physiological burden of sustained rapid heart rates. Many patients report significantly impaired exercise capacity during AFib that normalizes after cardioversion to sinus rhythm or with effective rate control.
Dizziness and lightheadedness occur from reduced cerebral perfusion secondary to reduced cardiac output or — with very rapid ventricular rates — from transient hypotension. True syncope (loss of consciousness) is less common in AFib than in other arrhythmias but warrants urgent evaluation, particularly when occurring at AFib onset, as it may indicate severe hemodynamic compromise requiring urgent cardioversion.
Chest discomfort — pressure, tightness, or heaviness — can occur during AFib from myocardial ischemia secondary to increased oxygen demand (rapid heart rate) and reduced diastolic filling time (which reduces coronary perfusion). In patients with underlying coronary artery disease, AFib episodes can trigger true angina or even myocardial infarction by imposing excessive demand on ischemia-prone myocardium.
A clinically important subset of AFib patients are asymptomatic — their AFib produces no perceptible symptoms and is discovered only incidentally (on a routine ECG, during another evaluation, or through a wearable device). Asymptomatic AFib carries the same stroke risk as symptomatic AFib and requires the same risk assessment and anticoagulation decision-making. The growing prevalence of smartwatches and consumer-grade ECG devices capable of detecting AFib has expanded asymptomatic AFib detection substantially.
How AFib Causes Stroke — The Mechanism Behind the Risk
The stroke risk in atrial fibrillation arises from a specific and well-understood mechanism. When the atria fibrillate rather than contracting in a coordinated fashion, blood stagnates in the left atrial appendage (LAA) — a small, ear-shaped pouch that extends from the left atrium. The LAA has a narrow neck and trabeculated interior that make it highly susceptible to blood stasis during AFib. Stagnant blood activates the coagulation cascade, forming a thrombus (blood clot) that adheres to the LAA wall and enlarges over time.
This LAA thrombus is the source of approximately 90 percent of cardioembolic strokes in patients with non-valvular atrial fibrillation. When a portion of the thrombus dislodges — during a spontaneous electrical cardioversion back to sinus rhythm, during physical exertion, or seemingly at random — it travels through the left atrium, left ventricle, and aorta into the cerebral circulation, lodging in a cerebral artery and causing ischemic stroke. AFib-related strokes have several features that make them particularly devastating: they are typically large (because the cardioembolic clots are larger than those from atherosclerotic plaque rupture), they affect the cerebral cortex (producing language, motor, and cognitive deficits), and they have a high 30-day recurrence risk without anticoagulation.
Stroke risk quantification in AFib is standardized through the CHA₂DS₂-VASc score, which assigns points for independent stroke risk factors: Congestive heart failure (1 point), Hypertension (1 point), Age 75 or above (2 points), Diabetes mellitus (1 point), Stroke or TIA history (2 points), Vascular disease — prior MI or peripheral artery disease (1 point), Age 65 to 74 (1 point), Sex category — female sex (1 point). Scores of 2 or above in men, or 3 or above in women, indicate high enough stroke risk that the survival benefit of anticoagulation outweighs bleeding risk for most patients. Anticoagulation therapy — with direct oral anticoagulants (DOACs: apixaban, rivaroxaban, dabigatran, edoxaban) preferred over warfarin for non-valvular AFib — reduces AFib-related stroke risk by 60 to 70 percent.
Risk Factors for Atrial Fibrillation
Atrial fibrillation develops when conditions that promote atrial fibrosis, dilation, altered electrical conduction, and ectopic impulse generation combine to destabilize the atrial electrical substrate. The major risk factors include:
Age is the most powerful AFib risk factor: prevalence doubles with each decade after 50, affecting approximately 0.5 percent of those under 60, 4 percent of those in their 60s, 8 percent in their 70s, and 13 to 17 percent of those over 80. Age-related atrial fibrosis and electrical remodeling progressively create the substrate for AFib initiation and maintenance.
Hypertension is the single most common modifiable AFib risk factor, responsible for approximately 14 percent of AFib cases attributable to specific risk factors. Chronic pressure overload causes left atrial dilation (from elevated LV filling pressures transmitted to the left atrium) and atrial fibrosis, both of which promote AFib. Well-controlled blood pressure significantly reduces AFib incidence compared to poorly controlled hypertension.
Heart failure has a bidirectional relationship with AFib: AFib can precipitate or worsen heart failure by reducing cardiac output and causing tachycardia-mediated cardiomyopathy, while heart failure promotes AFib through elevated atrial pressures, neurohumoral activation, and atrial remodeling. Approximately 40 to 50 percent of patients with advanced heart failure have AFib, and each condition worsens the prognosis of the other.
Coronary artery disease and structural heart disease (valvular disease, cardiomyopathy) contribute to AFib through shared mechanisms of atrial dilation, fibrosis, and ischemic atrial injury. Mitral valve disease — particularly mitral stenosis, which chronically elevates left atrial pressure — is the classic structural cause of AFib and remains the primary driver in populations where rheumatic heart disease is prevalent.
Obesity increases AFib risk by 50 percent and is one of the most impactful modifiable AFib risk factors in contemporary populations. Obesity promotes AFib through direct mechanical effects (increased pericardial fat, which has paracrine inflammatory effects on the atrium), hemodynamic effects (elevated filling pressures from expanded blood volume and LV remodeling), and inflammatory pathways. Weight loss of 10 percent or more body weight in obese AFib patients produces meaningful reductions in AFib burden and symptom severity, and sustained weight loss after bariatric surgery has shown dramatic reductions in AFib recurrence.
Obstructive sleep apnea independently triples AFib risk through intermittent hypoxia, autonomic fluctuations (surges of sympathetic and parasympathetic tone), intrathoracic pressure changes, and atrial stretch during obstructive episodes. AFib ablation success rates are substantially lower in patients with untreated OSA, and CPAP therapy in AFib patients with OSA improves ablation outcomes and reduces AFib burden.
Excessive alcohol consumption is a potent acute and chronic AFib trigger. The “holiday heart” phenomenon — AFib episodes temporally associated with binge drinking, classically occurring on Monday mornings after weekend heavy drinking or after holiday periods — is well recognized clinically. Alcohol increases AFib risk through direct atrial toxicity, autonomic effects, and associated cardiomyopathy with heavy chronic use. Moderate-to-heavy habitual alcohol consumption increases long-term AFib incidence, and alcohol reduction is recommended for AFib risk reduction.
Thyroid dysfunction — particularly hyperthyroidism and even subclinical hyperthyroidism (suppressed TSH with normal T3/T4) — increases AFib risk substantially, as excess thyroid hormone directly alters atrial electrophysiology. Thyroid function testing is part of routine AFib evaluation, and treatment of underlying thyroid disease can sometimes restore sinus rhythm without antiarrhythmic therapy.
The American Heart Association’s AFib resources provide comprehensive patient education on this condition. The CDC atrial fibrillation information covers prevalence, risk factors, and prevention. The NHLBI AFib guide addresses symptoms, diagnosis, treatment options, and living with AFib.
Related reading: Heart Failure | What Causes Heart Disease? | Major Risk Factors for Heart Disease | Coronary Artery Disease | How to Lower Heart Disease Risk
Sources
- Hindricks G, et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation. Eur Heart J. 2021;42(5):373-498.
- January CT, et al. 2019 AHA/ACC/HRS Focused Update of the 2014 Guidelines for Management of Patients With Atrial Fibrillation. J Am Coll Cardiol. 2019;74(1):104-132.
- Wolf PA, Abbott RD, Kannel WB. Atrial Fibrillation as an Independent Risk Factor for Stroke. Stroke. 1991;22(8):983-988.
- Lip GY, et al. Refining Clinical Risk Stratification for Predicting Stroke and Thromboembolism in Atrial Fibrillation Using a Novel Risk Factor-Based Approach (CHA₂DS₂-VASc). Chest. 2010;137(2):263-272.
- Simons GR. Atrial Fibrillation and Obesity. Curr Opin Cardiol. 2020;35(1):45-51.
- Linz D, et al. Interactions and Implications of Obstructive Sleep Apnea and Atrial Fibrillation. J Am Coll Cardiol. 2018;72(24):3142-3154.
Diagnosing Atrial Fibrillation — How AFib Is Detected
The diagnosis of atrial fibrillation requires documentation of the arrhythmia on cardiac rhythm recording. The specific monitoring strategy depends on symptom frequency and episode duration — a patient with daily palpitations can often be diagnosed rapidly, while a patient with monthly brief episodes requires prolonged monitoring.
12-lead ECG is the definitive diagnostic tool when AFib is ongoing at the time of evaluation. The ECG shows the characteristic findings: absent P waves replaced by irregular fibrillatory activity (fine or coarse oscillations at 300 to 600 per minute), and an irregularly irregular ventricular response with narrow QRS complexes (unless aberrant conduction or bundle branch block is present). A single 12-lead ECG capturing AFib during symptoms is sufficient to confirm the diagnosis. Every patient presenting with palpitations, unexplained dyspnea, or new-onset symptoms should receive a 12-lead ECG as the first diagnostic step.
Holter monitor — continuous ECG recording for 24 to 48 hours — is the standard initial monitoring strategy for patients whose symptoms occur at least every few days. The device records every heartbeat during the monitoring period, allowing correlation of symptoms with rhythm, quantification of AFib burden (percentage of time in AFib), and detection of other arrhythmias. Holter monitoring detects AFib in approximately 20 to 30 percent of patients who had a normal initial ECG but symptoms suggestive of a paroxysmal arrhythmia.
Extended ambulatory monitoring — 7-day, 14-day, or 30-day patch monitors — substantially increases AFib detection compared to standard 24 to 48-hour Holter monitoring, particularly for patients with less frequent episodes. Adhesive patch monitors worn continuously for extended periods capture arrhythmias that would be missed in shorter recording windows. A 2014 NEJM study (CRYSTAL AF) demonstrated that 30-day event monitors detected AFib in 12.4 percent of patients within 6 months after cryptogenic stroke — compared to 2 percent with conventional short-duration monitoring — demonstrating how prolonged monitoring unmasks occult paroxysmal AFib as the stroke cause.
Implantable loop recorders (ILR) — small subcutaneous devices implanted under local anesthesia that monitor cardiac rhythm continuously for up to 3 years — are indicated when prolonged ambulatory monitoring fails to capture symptoms or when AFib screening is needed after cryptogenic stroke (stroke without identified cause). ILRs have transformed the detection of paroxysmal AFib in high-risk populations and are increasingly used in patients with unexplained stroke, syncope, and heart failure with potential AFib contribution.
Consumer wearable devices — smartwatches and fitness trackers with optical photoplethysmography (PPG) or single-lead ECG capability — are changing AFib detection at the population level. The Apple Heart Study demonstrated that the Apple Watch’s irregular rhythm notification algorithm could detect AFib with positive predictive value of 84 percent in referred patients, and the product’s ECG app can produce single-lead tracings that cardiologists can use to diagnose AFib. While consumer devices cannot replace medical-grade monitoring, they serve a valuable role in prompting symptomatic patients to seek evaluation and in capturing paroxysmal AFib that occurs during normal daily activities.
Treatment of Atrial Fibrillation — Three Pillars
AFib management is organized around three therapeutic pillars that address its three major clinical consequences: stroke risk (anticoagulation), symptoms from rapid ventricular rate (rate control), and the arrhythmia itself (rhythm control). All three pillars require attention in most AFib patients, though their relative priority varies by individual patient characteristics.
Anticoagulation for stroke prevention is the highest-priority AFib treatment decision. Direct oral anticoagulants (DOACs) — apixaban (Eliquis), rivaroxaban (Xarelto), dabigatran (Pradaxa), and edoxaban (Savaysa) — have replaced warfarin as the preferred anticoagulants for non-valvular AFib. DOACs produce similar or superior stroke reduction compared to warfarin with significantly lower risk of intracranial hemorrhage (the most catastrophic anticoagulation complication), fixed dosing without the need for routine INR monitoring, fewer drug and food interactions, and rapid onset/offset that simplifies perioperative management. The decision to anticoagulate is based on CHA₂DS₂-VASc score — patients with scores of 2 or above (men) or 3 or above (women) clearly benefit, while those with score 0 (men) or 1 (women) have stroke risk low enough that anticoagulation is not recommended. Aspirin does not provide meaningful stroke prevention in AFib and is not an anticoagulant substitute.
Rate control targets the ventricular rate response during AFib, aiming to reduce the tachycardia that causes symptoms and — if sustained — tachycardia-mediated cardiomyopathy. Target resting heart rate in AFib is generally below 110 bpm for most patients (lenient rate control) or below 80 bpm at rest and 110 bpm with exertion (strict rate control) — with the RACE II trial finding no outcome difference between lenient and strict rate control strategies, supporting a resting rate target below 110 bpm as sufficient for most patients. Rate control agents include beta-blockers (most effective, first-line for most patients), non-dihydropyridine calcium channel blockers (verapamil, diltiazem — effective but contraindicated in heart failure with reduced ejection fraction), and digoxin (less effective for activity-related rate control but useful in heart failure patients). For patients with inadequate pharmacological rate control, AV node ablation with permanent pacemaker implantation eliminates AV conduction and controls the ventricular rate definitively.
Rhythm control — the strategy of restoring and maintaining normal sinus rhythm — provides superior symptom control and quality of life improvement compared to rate control alone in most patients, and the EAST-AFNET 4 trial demonstrated that early rhythm control (initiated within 1 year of diagnosis) significantly reduced the composite of cardiovascular death, stroke, hospitalization for heart failure, and acute coronary syndrome compared to rate control in newly diagnosed AFib patients. Pharmacological rhythm control uses antiarrhythmic drugs — flecainide and propafenone (Class IC, first-line in structurally normal hearts), sotalol (Class III, requires QTc monitoring), amiodarone (most effective, used when others fail, limited by long-term toxicity), and dofetilide (Class III, initiated in hospital due to proarrhythmia monitoring requirements). Catheter ablation — radiofrequency or cryoballoon pulmonary vein isolation (PVI), which eliminates the triggers for most paroxysmal AFib that originate in the pulmonary vein ostia — is the most effective rhythm control strategy, producing 70 to 80 percent freedom from AFib recurrence in paroxysmal AFib patients at one year, superior to antiarrhythmic drugs. For persistent AFib, ablation effectiveness is lower and may require additional substrate modification beyond PVI alone.
Risk Factor Modification — The Foundation of Long-Term AFib Management
Risk factor management is increasingly recognized as an essential and underutilized pillar of AFib management that improves symptoms, reduces AFib burden, and enhances the effectiveness of pharmacological and ablative treatments. The LEGACY study and ARREST-AF cohort demonstrated that aggressive risk factor management — targeting weight, blood pressure, glucose, lipids, sleep apnea, alcohol, and physical activity simultaneously — produced dramatic reductions in AFib burden and symptom severity independent of antiarrhythmic therapy or ablation. Patients who achieved sustained weight loss of 10 percent or more were significantly more likely to achieve freedom from AFib at long-term follow-up compared to those who did not lose weight.
The practical implications: blood pressure should be treated to target (below 130/80 mmHg) in all AFib patients with hypertension; obese patients should receive structured weight loss support (dietary modification, physical activity, and consideration of pharmacotherapy or bariatric surgery for severe obesity); alcohol consumption should be moderated or eliminated; sleep apnea should be screened for and treated with CPAP if confirmed; regular moderate aerobic exercise (which reduces AFib recurrence risk) should be encouraged; and smoking cessation should be achieved. These lifestyle and risk factor targets are not adjuncts to medical or procedural AFib management — they are integral to it, and patients who manage risk factors effectively have meaningfully better AFib outcomes than those who do not.