What Is Insulin and Why Is It Important?
Few molecules in the human body carry as much consequence as insulin. What is insulin? It is a small protein hormone produced by the pancreas that serves as the master regulator of blood glucose — the biological key that allows glucose to enter cells throughout the body and be used for energy. Without insulin, glucose accumulates in the blood while cells are simultaneously starved of fuel, a paradox that — before the discovery and extraction of insulin in 1921 — was invariably fatal within months of onset in those who needed it most. Today, insulin remains one of the most critically important and carefully studied molecules in medicine, and understanding how it works, why it matters, and what happens when its production or action fails is foundational to understanding diabetes, metabolic health, and the biology of energy itself.
What Is Insulin? The Basic Biology
Insulin is a peptide hormone — a small protein made of two chains of amino acids (the A-chain with 21 amino acids and the B-chain with 30 amino acids) linked together by disulfide bonds. It is produced by beta cells in the islets of Langerhans, specialized clusters of cells scattered throughout the pancreas. The pancreas contains approximately one million of these islets, each a miniature endocrine organ capable of detecting blood glucose levels and responding within minutes with precisely calibrated hormone secretion.
Insulin is produced in several stages. Beta cells first synthesize a longer precursor molecule called preproinsulin in the endoplasmic reticulum. This is cleaved into proinsulin, which folds into a specific three-dimensional shape stabilized by the disulfide bonds. Proinsulin is then packaged into secretory granules, where enzymes remove a connecting segment called the C-peptide, producing the final two-chain insulin molecule. The granules dock at the cell surface, ready to release insulin rapidly when blood glucose rises. Interestingly, the C-peptide is released in equal molar amounts with insulin, making it a useful clinical marker for measuring how much insulin the pancreas is actually producing — information that is helpful in distinguishing Type 1 from Type 2 diabetes and in tracking residual beta cell function.
To fully understand what insulin is and how it fits into the broader picture of glucose regulation, it helps to first explore how the body controls blood sugar — the comprehensive regulatory system within which insulin plays its central role.
How Insulin Is Released: The Glucose-Sensing Mechanism
Insulin secretion is triggered primarily by rising blood glucose, with the response beginning within two to five minutes of glucose reaching the beta cells. The mechanism by which beta cells detect glucose is elegant in its precision: glucose enters beta cells through specialized GLUT2 transporter proteins, is metabolized by glucokinase (an enzyme that produces ATP from glucose in proportion to the glucose concentration), and the resulting rise in the ATP-to-ADP ratio closes ATP-sensitive potassium channels in the cell membrane. Channel closure causes the cell membrane to depolarize, triggering calcium influx through voltage-gated calcium channels. This calcium surge causes the insulin-containing secretory granules to fuse with the cell membrane and release their contents into the bloodstream — a process called exocytosis.
The insulin response to a meal occurs in two distinct phases:
- First phase (0–10 minutes): A rapid burst of pre-stored insulin from granules already docked at the cell membrane, released within the first two to five minutes of glucose detection. This first-phase surge quickly suppresses the liver’s glucose output and signals peripheral tissues to prepare for glucose uptake. It is the component of insulin secretion that most reliably distinguishes healthy glucose regulation from early Type 2 diabetes — first-phase secretion is the first to deteriorate as beta cell function declines
- Second phase (10–120 minutes): A sustained, more gradually rising insulin release from newly mobilized granules, continuing as long as blood glucose remains elevated. The second phase handles the bulk of the post-meal glucose load, managing glucose disposal over the full absorption window
Insulin release is not only triggered by glucose. Amino acids from protein digestion — particularly leucine and arginine — also stimulate insulin secretion. Gut hormones called incretins (GLP-1 and GIP), released by intestinal cells in response to food, amplify insulin secretion significantly before glucose even reaches the pancreas, accounting for up to 70 percent of the total post-meal insulin response. Fat has minimal direct effect on insulin secretion but slows gastric emptying, blunting the glucose peak from a meal.
How Insulin Works: Signaling at the Cellular Level
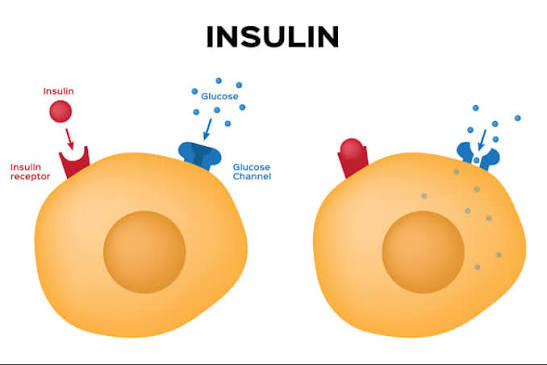
Once in the bloodstream, insulin binds to specific insulin receptors on the surface of target cells — primarily muscle cells, fat cells, and liver cells. The insulin receptor is a transmembrane protein with two alpha subunits (outside the cell, where insulin binds) and two beta subunits (spanning the membrane, where intracellular signaling begins). When insulin binds, the receptor’s beta subunits activate tyrosine kinase activity — they add phosphate groups to themselves and to downstream signaling proteins in a cascade that ultimately produces glucose uptake, metabolic effects, and gene expression changes.
The most important downstream effect in terms of blood sugar control is the activation of the PI3K-Akt signaling pathway, which causes GLUT4 glucose transporter proteins to translocate from intracellular storage vesicles to the cell surface membrane. GLUT4 is essentially a glucose-specific door that opens in response to insulin — when it moves to the cell surface, it creates channels through which glucose can flow from the blood (where it is at high concentration after a meal) into the cell (where the concentration is lower). In muscle cells, this glucose is used for immediate energy or stored as glycogen; in fat cells, it is converted to triglycerides for storage.
- Muscle: Stimulates GLUT4 glucose uptake; promotes glycogen synthesis; stimulates protein synthesis
- Liver: Suppresses glucose output (glycogenolysis + gluconeogenesis); promotes glycogen synthesis; promotes fat synthesis from excess glucose
- Fat tissue: Stimulates GLUT4 glucose uptake; promotes fat storage (lipogenesis); inhibits fat breakdown (lipolysis)
- Brain: Regulates appetite, energy balance, and cognition via insulin receptors in the hypothalamus; does not require insulin for glucose uptake
- Blood vessels: Promotes vasodilation via nitric oxide; anti-inflammatory effects on endothelium when signaling is normal
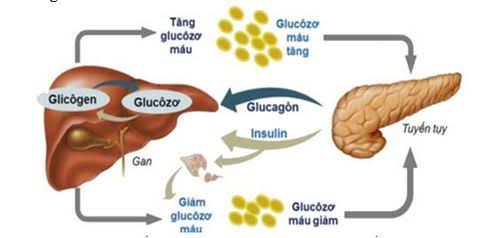
- Pancreas (alpha cells): Suppresses glucagon secretion, preventing the liver from adding glucose when blood sugar is already elevated
Insulin’s Roles Beyond Blood Sugar
While insulin is best known as the hormone that lowers blood sugar, its biological roles extend far beyond glucose metabolism. Insulin is an anabolic hormone — one that promotes growth, synthesis, and storage — with effects throughout the body that matter profoundly for health beyond glycemic control.
Protein metabolism: Insulin stimulates protein synthesis in muscle cells and simultaneously inhibits protein breakdown (proteolysis). This anabolic effect on muscle is the reason insulin is critical for muscle growth and maintenance — which is why people with severely deficient insulin production (untreated Type 1 diabetes) experience rapid muscle wasting alongside fat loss, as the body breaks down protein for energy and gluconeogenesis in the absence of adequate insulin.
Fat metabolism: Insulin powerfully suppresses lipolysis — the breakdown of stored triglycerides in fat cells into free fatty acids. Between meals and during fasting, declining insulin levels allow lipolysis to proceed, releasing free fatty acids that serve as alternative fuel for most body tissues (sparing glucose for the brain). After meals, rising insulin shuts off lipolysis and shifts fat cells into storage mode. In Type 1 diabetes without insulin, unrestrained lipolysis produces the massive free fatty acid release that the liver converts into ketone bodies — the underlying biochemistry of diabetic ketoacidosis.
Vascular effects: Normal insulin signaling promotes vasodilation by stimulating nitric oxide production in the endothelium (the inner lining of blood vessels), improving blood flow to tissues. Insulin resistance impairs this vasodilatory effect while often leaving intact the pathway by which insulin promotes sodium retention and sympathetic nervous system activation — a mismatch that contributes to the high blood pressure frequently seen with insulin resistance and metabolic syndrome.
Brain effects: The brain has insulin receptors in the hypothalamus and other regions, where insulin acts as a satiety signal — reducing food intake and promoting energy expenditure. Brain insulin resistance is associated with increased appetite, weight gain, and may contribute to the cognitive impairment increasingly linked to metabolic dysfunction.
Why Insulin Is Essential: Life Without It
The discovery of insulin in 1921 by Frederick Banting, Charles Best, John Macleod, and James Collip at the University of Toronto is one of the most consequential events in the history of medicine. Before 1922, when the first human patient received insulin injections, a diagnosis of Type 1 diabetes was a death sentence — typically within one to three years, as the body progressively wasted away for lack of cellular fuel. Children diagnosed with Type 1 were placed on starvation diets (the only treatment that prolonged survival) and slowly deteriorated despite every effort.
Without insulin, the physiology is catastrophic. Glucose cannot enter most cells, so blood sugar rises relentlessly. Cells, starved of fuel, send distress signals that the brain interprets as starvation — triggering the release of counter-regulatory hormones (glucagon, cortisol, epinephrine) that further raise blood sugar while breaking down fat and muscle for alternative energy. The liver converts the released free fatty acids into ketone bodies at a rate that overwhelms the body’s buffering capacity, producing diabetic ketoacidosis — a condition in which the blood becomes dangerously acidic. Without treatment, DKA progresses to coma and death.
The first patient to receive purified insulin — a fourteen-year-old named Leonard Thompson in January 1922 — was near death when he received the first injection. Within days, his blood sugar normalized and his symptoms reversed. The transformation was described as miraculous by the physicians who witnessed it. Banting and Macleod received the Nobel Prize in Physiology or Medicine in 1923.
Today, insulin remains the essential treatment for Type 1 diabetes and is required by many people with advanced Type 2 diabetes as well. Modern insulin preparations have improved dramatically from the early animal-derived formulations: recombinant human insulin, rapid-acting analogs (that peak within 15 minutes), long-acting basal insulins (that provide stable coverage for 24 hours or more), and ultra-long-acting formulations have all been developed to better mimic the body’s natural insulin pattern. Continuous insulin delivery via pumps, combined with continuous glucose monitoring, has created increasingly automated “closed-loop” systems that approach the function of a mechanical pancreas.
When Insulin Production or Action Fails
Insulin failure takes two fundamentally different forms corresponding to the two main types of diabetes:
Insulin deficiency (Type 1 diabetes): The immune system destroys the beta cells that produce insulin. Initial symptoms appear when roughly 80 to 90 percent of beta cell mass has been eliminated and residual insulin production can no longer maintain blood sugar. The onset is typically dramatic — over days to weeks — with rapid hyperglycemia, weight loss, ketoacidosis risk, and an absolute requirement for exogenous insulin from diagnosis. There is no alternative treatment; without insulin replacement, Type 1 diabetes is fatal. Our guide on what is diabetes explains the differences between Type 1 and Type 2 in detail.
Insulin resistance and relative deficiency (Type 2 diabetes): Beta cells continue producing insulin, but cells throughout the body respond to it inadequately. Initially, beta cells compensate by producing more insulin — sometimes three to five times the normal amount — to maintain blood sugar in the normal range. Over years, beta cell function declines under this sustained high demand. When beta cell output can no longer compensate for the degree of insulin resistance, blood sugar rises into the prediabetes and then diabetes range. Treatment initially uses medications that improve insulin sensitivity (metformin) or reduce glucose absorption, with insulin added when beta cell function falls below the level needed to maintain acceptable control.
Exogenous Insulin: Types and Modern Formulations
For people who require insulin as a medication — primarily those with Type 1 diabetes and some with Type 2 — understanding the different types of insulin available is important for management. Modern insulin formulations are categorized primarily by their time-action profiles:
- Rapid-acting analogs (lispro, aspart, glulisine): Onset within 10–15 minutes, peak at 1–2 hours, duration 3–5 hours. Taken immediately before meals to cover post-meal glucose rises
- Short-acting (regular) insulin: Onset 30–60 minutes, peak 2–4 hours, duration 5–8 hours. Given 30 minutes before meals; largely replaced by rapid-acting analogs in most settings
- Intermediate-acting (NPH) insulin: Onset 2–4 hours, peak 4–10 hours, duration 10–16 hours. Used as a basal insulin in some regimens
- Long-acting analogs (glargine, detemir, degludec): Onset 1–2 hours, no pronounced peak, duration 20–42 hours. Provides stable baseline insulin coverage throughout the day and night, mimicking the pancreas’s continuous low-level secretion between meals
Most people requiring insulin therapy use a “basal-bolus” regimen combining a long-acting insulin for baseline coverage with rapid-acting insulin doses at each meal, calibrated to the carbohydrate content of the meal and the current blood sugar level. This approach most closely mimics normal pancreatic function. Insulin pumps deliver rapid-acting insulin continuously at a programmed basal rate, with user-initiated boluses at mealtimes — providing even more flexibility and precision than multiple daily injections.
The story of insulin — from its discovery to the sophisticated formulations and delivery systems available today — is one of the most remarkable chapters in the history of medicine, and the molecule at its center remains as essential today as it was when the first patient received it more than a century ago. Monitoring how well the body’s insulin system is functioning — through tools like the A1C test and home blood sugar monitoring — is a central part of managing any condition involving insulin production or action. For guidance on interpreting these measurements, see our guide on the A1C test and our overview of home blood sugar monitoring.
Insulin and Weight: Understanding the Connection
Insulin’s role as an anabolic (storage-promoting) hormone means it has a complex and often misunderstood relationship with body weight. In the postprandial state — after eating — insulin promotes fat storage and suppresses fat breakdown (lipolysis). This is normal and appropriate: the body is using food energy efficiently and storing any excess. Between meals, as insulin falls, lipolysis is permitted and stored fat is mobilized for energy. In a healthy person eating a balanced diet with adequate time between meals, this cycle of insulin-mediated storage and low-insulin fat release is well-balanced.
Problems arise when insulin levels remain chronically elevated — a state called hyperinsulinemia. Chronically high insulin persistently suppresses lipolysis and promotes fat storage, making it harder for the body to access stored fat for energy even between meals. This can make weight loss more difficult and can promote fat accumulation — particularly visceral fat — even without excessive caloric intake. Hyperinsulinemia is closely associated with insulin resistance: the two conditions drive each other in a reinforcing cycle, since higher insulin is needed to overcome resistance, and the resulting hyperinsulinemia worsens resistance over time through down-regulation of insulin receptors.
Dietary approaches that reduce postprandial insulin surges — including higher-protein diets, lower-glycemic carbohydrate choices, and adequate dietary fiber — may help reduce chronic hyperinsulinemia in people with insulin resistance, contributing to improved fat metabolism and weight management. This is the metabolic rationale behind the effectiveness of reduced-carbohydrate dietary patterns for people with Type 2 diabetes and prediabetes, though it is important to note that total caloric balance remains important alongside insulin dynamics.
Measuring Insulin: What the Tests Reveal
While blood glucose tests measure what insulin does (the effect on blood sugar), direct insulin measurement is sometimes used clinically to assess how much insulin the body is producing and how efficiently it is working. Several tests are available:
Fasting insulin is the most commonly used measure of insulin production. Measured after at least eight hours without eating, fasting insulin reflects baseline pancreatic output and provides an indirect measure of insulin sensitivity — higher fasting insulin levels suggest the pancreas is compensating for insulin resistance. Normal fasting insulin is generally considered to be below 25 mIU/L (with optimal levels often cited below 10 mIU/L), though reference ranges vary by laboratory and the clinical significance of specific values is interpreted in context.
C-peptide is released in equal amounts to insulin from beta cells and persists in the blood longer than insulin itself, making it a more reliable measure of beta cell function. C-peptide testing is particularly useful for distinguishing Type 1 from Type 2 diabetes (Type 1 shows very low or undetectable C-peptide, reflecting destroyed beta cells; Type 2 typically shows normal or elevated C-peptide), and for assessing residual beta cell function in people already taking exogenous insulin (since injected insulin does not contain C-peptide).
The HOMA-IR index (Homeostatic Model Assessment of Insulin Resistance) calculates insulin resistance from fasting glucose and fasting insulin values: HOMA-IR = (fasting glucose in mg/dL × fasting insulin in mIU/L) / 405. Values above 2.0 generally suggest meaningful insulin resistance; values above 3.0 indicate significant resistance. While not used as a formal diagnostic test, HOMA-IR is widely used in research and increasingly in clinical practice to assess insulin sensitivity and track changes with lifestyle or medication interventions.
Supporting Healthy Insulin Function Through Lifestyle
For people seeking to maintain healthy insulin sensitivity and support optimal insulin function — whether to prevent diabetes, manage prediabetes, or complement medication therapy — the evidence-based lifestyle factors are consistent and well-established.
Regular physical activity is the most powerful lifestyle tool for improving insulin sensitivity. Exercise activates AMPK (AMP-activated protein kinase), a cellular energy sensor that promotes GLUT4 translocation to the cell surface independently of insulin signaling — allowing muscle cells to absorb glucose without requiring insulin’s involvement. Chronic exercise training upregulates the total number of insulin receptors and GLUT4 transporters in muscle tissue, making every unit of insulin more effective. Both aerobic exercise (which primarily improves mitochondrial function and reduces visceral fat) and resistance training (which increases muscle mass and GLUT4 content) contribute to improved insulin sensitivity through distinct but complementary pathways.
Sleep quality and duration have a direct and surprisingly large impact on insulin sensitivity. Even one night of poor sleep — defined as sleeping five to six hours instead of the recommended seven to nine — reduces insulin sensitivity by 20 to 25 percent the following day, as measured by glucose clamp studies. Chronic sleep restriction worsens insulin resistance progressively and promotes visceral fat accumulation through elevated cortisol and changes in appetite-regulating hormones. Treating obstructive sleep apnea, which causes repeated nocturnal oxygen deprivation and cortisol surges, significantly improves insulin sensitivity in affected individuals.
Dietary quality affects insulin dynamics in multiple ways. Diets high in refined carbohydrates and added sugars produce repeated large insulin surges that, over years, may accelerate beta cell exhaustion and worsen insulin resistance through receptor down-regulation. Dietary fiber slows glucose absorption, blunting post-meal insulin demand. Saturated fat can impair insulin receptor signaling at the cellular level, while monounsaturated fats (olive oil, avocados, nuts) and omega-3 fatty acids from fatty fish appear to preserve or improve insulin sensitivity. Polyphenols from vegetables, berries, and green tea have emerging evidence for improving insulin signaling in observational studies and small trials.
Understanding what insulin is and how it functions at every level — from beta cell secretion to cellular receptor binding to tissue-specific metabolic effects — provides the foundation for understanding why certain health conditions develop, why specific interventions work, and why blood sugar management matters so profoundly for virtually every dimension of long-term health.
Sources: American Diabetes Association. Standards of Medical Care in Diabetes — 2024. Diabetes Care. 2024;47(Suppl 1):S20–S42. • Bliss M. The Discovery of Insulin. University of Chicago Press; 2007. • Saltiel AR, Kahn CR. Insulin signalling and the regulation of glucose and lipid metabolism. Nature. 2001;414(6865):799–806.