A cancer diagnosis is one of the most frightening moments a person can face. But here’s something most people don’t realize until their oncologist explains it: the stage at which cancer is found can make an enormous difference in what comes next. When localized cancer is discovered — meaning the disease is still confined to the organ where it started — the outlook for most cancer types is considerably better than when cancer has spread elsewhere. According to the National Cancer Institute, the overall 5-year relative survival rate for all cancers diagnosed at the localized stage is approximately 89%, compared to 72% for regional stage and just 22% for distant (metastatic) stage. (NCI SEER, 2023)
That number matters. And so does understanding what it actually means for you. A localized diagnosis doesn’t just affect your prognosis — it shapes the conversation you have with your oncologist, the treatment choices available to you, and the recovery path ahead. Knowing what you’re dealing with puts you in a much stronger position to ask the right questions and make decisions that align with your values and goals.
This article walks through what localized cancer means, how doctors confirm a cancer has stayed contained, what the survival statistics tell you — and what they don’t — and how localized cancers are typically treated. Whether you’ve just received a diagnosis or you’re trying to help a loved one make sense of theirs, this guide is designed to help you understand the road ahead clearly and honestly.
What Does “Localized Cancer” Mean?
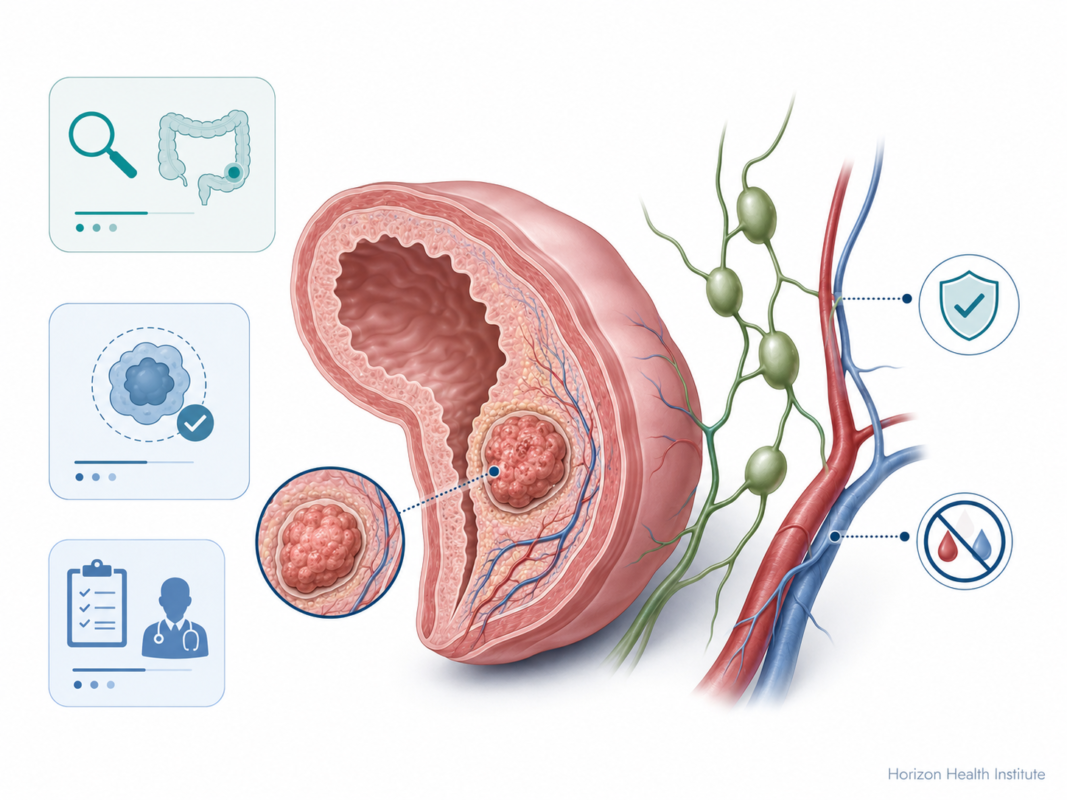
Localized cancer is cancer that is confined to the organ or tissue where it first developed and has not spread to nearby lymph nodes, surrounding tissues, or distant organs. In the NCI’s SEER staging system, “localized” is the earliest invasive cancer category — one stage below regional spread and two stages below distant (metastatic) cancer.
Localized breast cancer stays within breast tissue. Localized prostate cancer remains within the prostate gland. Localized colon cancer is contained within the wall of the colon. The disease may still be sizable or aggressive-looking under a microscope, but it has not crossed into other anatomical regions.
The term “localized” comes from the SEER summary stage system, developed by the National Cancer Institute to classify cancer cases in its Surveillance, Epidemiology, and End Results (SEER) database. SEER uses three broad categories:
- Localized — no spread beyond the organ of origin
- Regional — spread to nearby lymph nodes or adjacent tissues
- Distant — spread to organs far from the original site (also called metastatic cancer)
This classification is different from the TNM staging system (Tumor, Node, Metastasis) your oncologist uses in clinical practice. Localized stage generally corresponds to Stage I or early Stage II in TNM terms — but the exact relationship varies by cancer type. It’s worth asking your doctor which staging system they’re referencing when they explain your results.
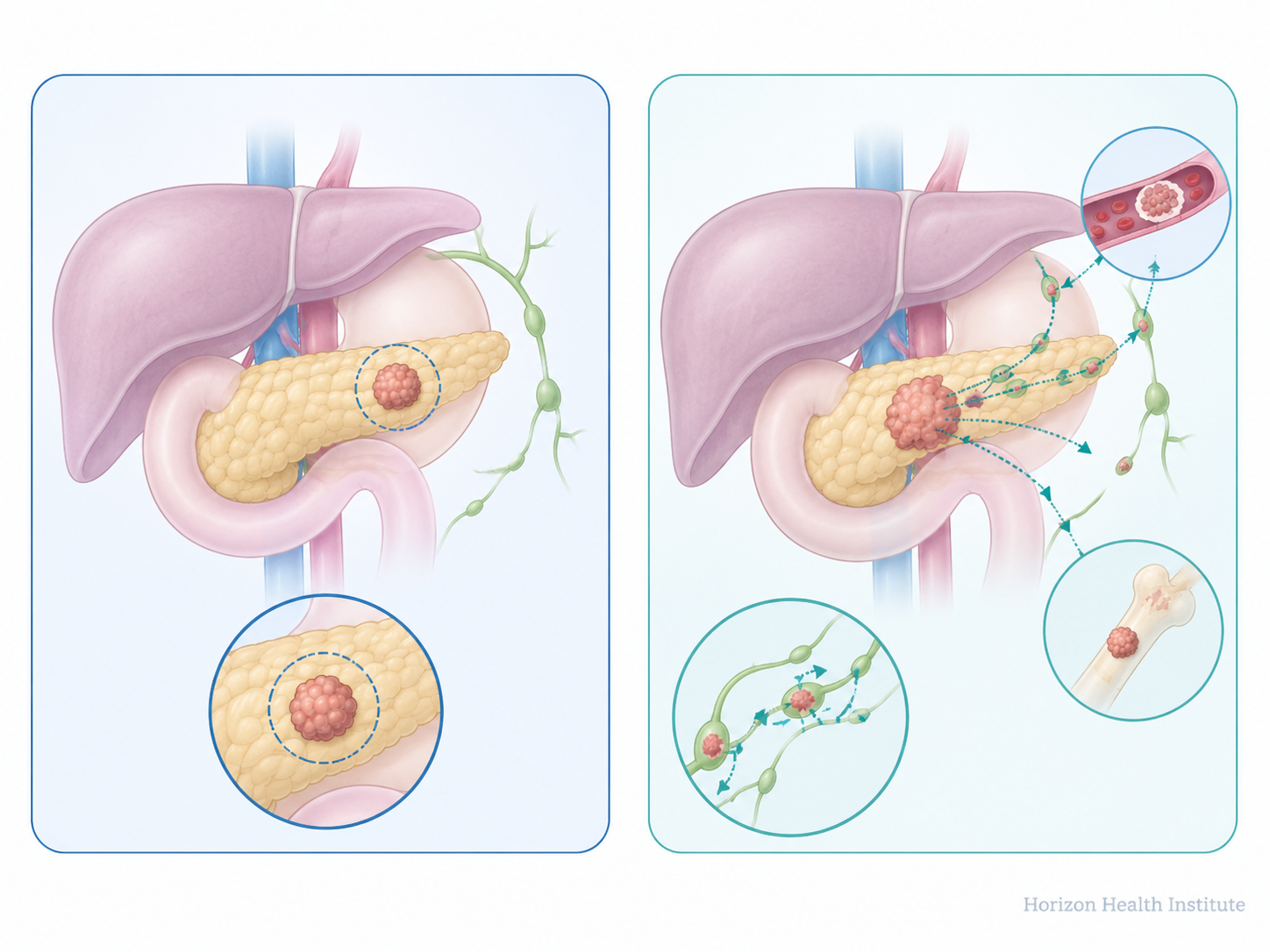
The practical meaning of “localized” also depends significantly on which cancer you have. Localized prostate cancer with a low Gleason score, for instance, is often so slow-growing that active monitoring without immediate treatment is a reasonable choice — many men with this diagnosis outlive the cancer without ever needing surgery or radiation. Localized pancreatic cancer, by contrast, requires prompt and aggressive intervention because of the tumor’s inherent biology. A localized kidney tumor in an 80-year-old with heart disease may be watched rather than removed. Staging is the first piece of the picture; your cancer’s specific type, grade, and your overall health fill in the rest.
According to the NCI SEER database, approximately 45% of all new US cancer diagnoses are made at the localized stage. (NCI SEER, 2023) Nearly half of all cancers are caught before they’ve had a chance to spread — a direct result of expanded screening programs and greater public awareness of early warning signs.
How Doctors Determine If Cancer Is Localized
Staging a cancer isn’t a single test — it’s a process. Your oncology team builds a complete picture of the disease using imaging, pathology, and sometimes surgical exploration. Each piece of information adds detail and refines the treatment plan.
The Diagnostic Workup
Once a tumor is identified — whether through a screening test, a symptom that brought you to your doctor, or an incidental finding on a scan — the staging workup typically includes:
- Imaging studies — CT scans, MRI, PET scans, and bone scans show whether cancer has traveled to lymph nodes or distant organs
- Biopsy and pathology — A tissue sample analyzed under a microscope confirms cancer type, grade (how aggressive the cells appear), and often molecular markers
- Sentinel lymph node biopsy — Used for breast cancer and melanoma; the first lymph node(s) draining the tumor site are sampled to test for spread
It’s worth understanding what different imaging tests are actually looking for. A CT scan shows anatomical detail — whether lymph nodes are enlarged, whether a suspicious mass appears in another organ. A PET scan adds a metabolic layer: cancer cells typically absorb glucose more rapidly than normal cells, creating “hot spots” that light up on the scan with a radioactive tracer. A PET-CT — which combines both — has become the standard for staging many cancers including lymphomas, lung cancers, and esophageal cancers. MRI is particularly valuable for evaluating soft-tissue tumors, rectal cancers, and any possible involvement of the brain or spinal cord.
What the Pathology Report Shows
Your pathology report is the most important document in your cancer diagnosis. It tells your oncologist:
- Tumor size (the T in TNM staging)
- Lymph node involvement (N — with N0 meaning no lymph node spread detected)
- Metastasis status (M — with M0 meaning no evidence of distant spread)
- Surgical margins — whether the tissue removed is cancer-free at the outer edges
- Grade — how different the cancer cells look from normal tissue (Grade 1 is closest to normal; Grade 3–4 signals more aggressive-looking cells)
When T, N, and M together indicate the cancer is confined to its original organ (typically T1–T2, N0, M0), the cancer is staged as localized. That classification drives treatment planning.
In some cancers — particularly colon and breast cancer — surgeons also examine nearby lymph nodes during the primary operation to check for microscopic cancer spread that imaging cannot detect. This is called a lymphadenectomy or lymph node dissection. Even a lymph node that looks normal on a CT scan can occasionally harbor microscopic cancer deposits, which is why surgical staging combined with pathological examination remains the most definitive method for confirming localized status.
Localized Cancer Survival Rates: What the Numbers Show
The survival statistics for localized cancer are, for most types, genuinely encouraging. But they’re also frequently misunderstood — so it’s worth taking a moment to read them carefully.
According to the NCI’s SEER database, the overall 5-year relative survival rate for all cancers diagnosed at the localized stage is 89%. (NCI SEER, 2023) This measures the percentage of people with cancer who survive at least five years after diagnosis compared to people of similar age and sex without cancer. It’s the standard benchmark in oncology.
Looking at individual cancer types makes the importance of early detection even clearer:
| Cancer Type | Localized 5-Year Survival | Regional 5-Year Survival | Distant 5-Year Survival |
|---|---|---|---|
| Breast cancer | 99% | 86% | 31% |
| Prostate cancer* | ~100% | ~100% | 34% |
| Melanoma (skin) | 99% | 71% | 32% |
| Colon cancer | 91% | 73% | 14% |
| Lung cancer | 61% | 35% | 7% |
| Source: American Cancer Society, Cancer Facts & Figures 2024. *Prostate regional rate reflects hormone-sensitive disease; outcomes vary significantly by Gleason score. | |||
The lung cancer figures deserve particular attention. Even though localized lung cancer has a lower survival rate than other localized cancers (61%), that’s still nearly nine times better than when lung cancer is caught at the distant stage (7%). The challenge is that only about 21% of lung cancer cases are found at the localized stage — which is precisely why low-dose CT screening for high-risk individuals matters so much. (NCI SEER, 2023)
It’s also worth knowing that survival rates across most cancer types have been improving steadily over the past two decades. The NCI reports that the overall US cancer death rate declined by 33% from 1991 to 2019 — driven by earlier detection, expanded screening, and more effective treatments. (NCI, 2023) The survival figures you see in published tables are calculated from patients diagnosed five to ten years ago; outcomes with today’s modern treatments may be even more favorable for people diagnosed now.
Survival statistics are population averages — they describe what happened to large groups of people over defined time periods. They cannot tell you what will happen to you specifically. Your individual outlook depends on cancer type and subtype, your age and overall health, tumor grade and molecular markers, and the treatment center you choose. These numbers are a starting framework — not a final verdict. Use them to set context, then focus your conversations with your oncologist on the specifics of your tumor biology.
How Localized Cancer Is Treated

Because localized cancer has not spread, the primary goal of treatment is curative — to eliminate the cancer entirely. That’s a meaningful distinction from treatment for regional or distant stage disease, which more often focuses on controlling growth and extending life. The range of treatment options for localized cancer is also typically broader, and the chances of achieving a complete response are substantially higher.
Surgery
Surgery remains the most common first-line treatment for localized solid tumors. The goal is to remove the tumor along with a clear margin of surrounding tissue, ensuring the edges are cancer-free. In many cases, surgery alone is curative for localized cancer.
Surgical techniques continue to advance. Minimally invasive approaches — robotic and laparoscopic surgery — are now standard for colon, prostate, and kidney cancers, often reducing hospital stays and recovery times significantly. For most localized breast cancers, lumpectomy combined with radiation therapy achieves the same cure rates as mastectomy while preserving the breast. (Mayo Clinic, 2023)
Depending on the cancer type and location, your surgeon may also remove some nearby lymph nodes to check for microscopic spread that wasn’t visible on imaging. In colon cancer, this often means removing the segment of colon containing the tumor along with the associated lymph node bundle. In early-stage breast cancer, a sentinel lymph node biopsy (removal of just one to three nodes) is typically preferred over a full axillary dissection to minimize the risk of lymphedema. Your surgical team will explain the scope of node sampling they recommend and why.
Recovery from surgery for localized cancer varies by procedure. A robotic-assisted prostatectomy may allow discharge in one to two days, while an open colectomy may require four to seven days in the hospital followed by several weeks of gradually returning to full activity. Your surgical team will provide specific guidance on wound care, activity restrictions, and when you can expect to feel like yourself again.
Radiation Therapy
Radiation destroys cancer cells using high-energy beams delivered with increasing precision. Modern radiation planning uses 3D imaging to map the tumor and surrounding structures, allowing higher doses to reach the cancer while sparing nearby healthy tissue. Depending on the situation, radiation may be used as the primary treatment (localized prostate cancer, head-and-neck cancers, certain lung tumors), after surgery to eliminate remaining cells (adjuvant radiation), or before surgery to shrink the tumor first (neoadjuvant radiation).
Targeted Therapy and Immunotherapy
Molecular testing of your tumor may reveal targets for precision treatments. Targeted therapy blocks specific proteins cancer cells depend on to grow — such as EGFR inhibitors in certain lung cancers and HER2-targeted agents in HER2-positive breast cancer. Immunotherapy trains your immune system to recognize and attack cancer cells, and is increasingly used in localized melanoma and bladder cancer. These treatments are typically added when tumor characteristics suggest standard surgery or radiation alone may not be enough.
Active Surveillance
Active surveillance — close monitoring without immediate intervention — is a validated approach for very-low-risk and low-risk localized prostate cancer (Gleason score 6 / Grade Group 1), small low-risk papillary thyroid tumors, and certain small kidney tumors in older patients with competing health concerns. Under active surveillance, your oncologist typically checks PSA levels every three to six months and may repeat imaging or biopsies annually to verify the cancer isn’t progressing. At the first sign of meaningful change, treatment is promptly initiated. Your oncologist will help you decide whether active surveillance is appropriate for your specific situation — it’s not a one-size-fits-all choice.
| Cancer Type | Common Localized Treatment(s) |
|---|---|
| Breast cancer | Lumpectomy + radiation; or mastectomy |
| Prostate cancer | Surgery, radiation, or active surveillance (low-risk) |
| Colon cancer | Colectomy; adjuvant chemotherapy if high-risk features |
| Lung cancer | Lobectomy or SBRT (stereotactic body radiation) |
| Melanoma | Wide local excision; sentinel lymph node biopsy |
| Bladder cancer | Transurethral resection + intravesical immunotherapy |
| Source: NCI, Mayo Clinic, 2023 | |
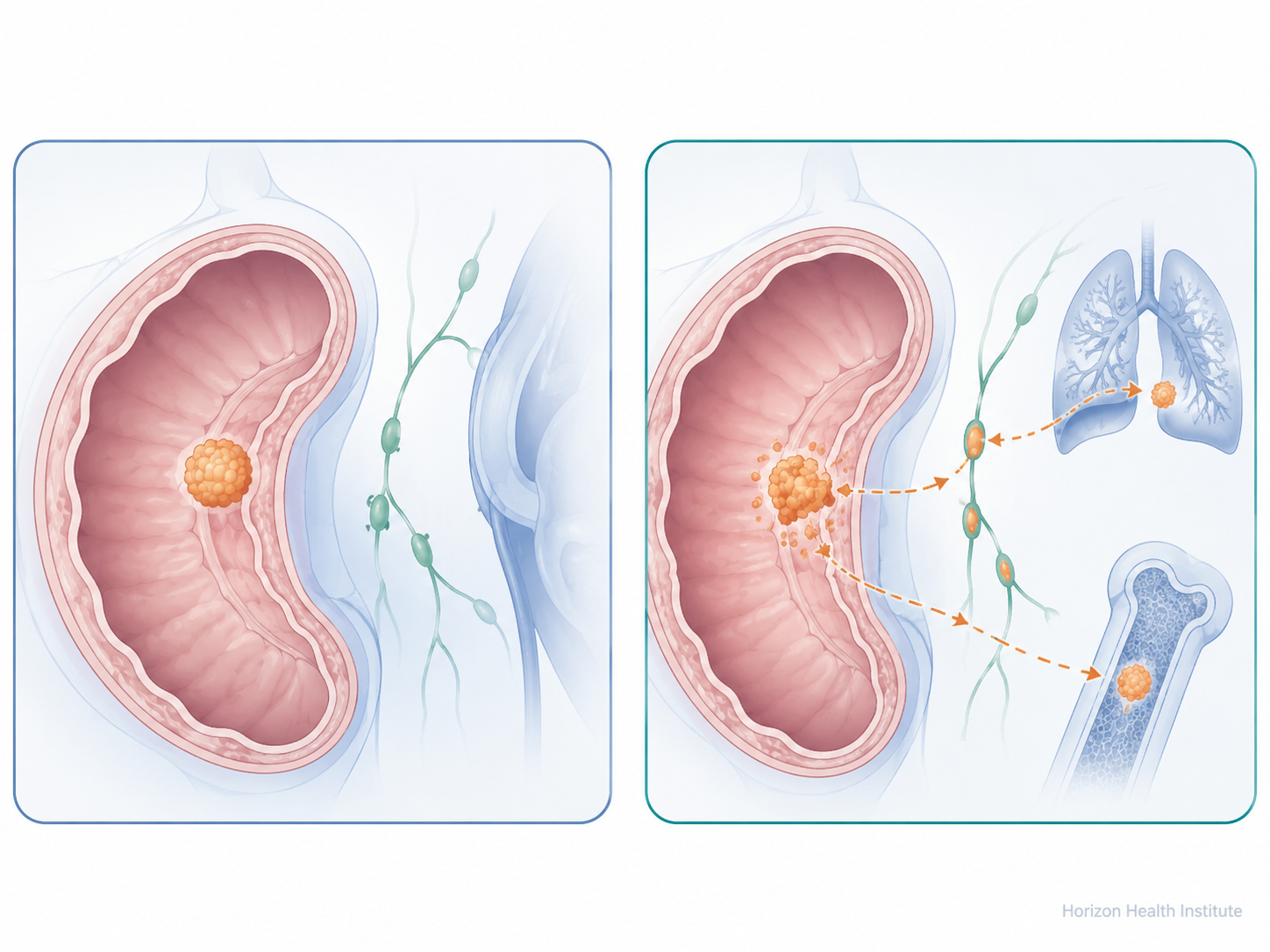
Can Localized Cancer Spread? What to Know
A localized diagnosis is genuinely good news — but it doesn’t mean the cancer can’t change course. Left untreated, localized cancer can progress to regional or distant stages. And even after successful treatment, recurrence is possible, sometimes years later.
Several factors influence whether a localized cancer stays contained:
- Treatment completeness — clear surgical margins substantially lower recurrence risk compared to incomplete resection
- Tumor grade — high-grade cancer cells are more biologically aggressive, even at a localized starting point
- Molecular profile — certain genetic features increase a tumor’s tendency to spread, independent of its apparent stage at diagnosis
After primary treatment, your oncology team will set up a structured surveillance schedule — regular check-ins, imaging, and lab work designed to catch any recurrence as early as possible. Early-detected recurrence carries better treatment options than disease found later. Surveillance schedules are typically most intensive in the first two to three years after treatment, when recurrence risk is usually highest, then become less frequent as time passes without any sign of disease.
Contact your oncologist promptly — don’t wait for your next scheduled visit — if you develop unexplained weight loss, persistent new pain in bones or abdomen, new lumps or swelling, or fatigue that doesn’t improve with rest. The goal of surveillance is to catch any change at its earliest, most manageable point.
The biology behind recurrence is worth understanding at a basic level. Even when a tumor appears fully localized, some cancer cells may have shed into the bloodstream or lymphatic system before treatment — a phenomenon called micrometastasis. In most cases, the immune system clears these circulating cells before they can establish elsewhere. But for some cancer types, particularly high-grade tumors, these cells can survive in a dormant state for months or years before growing into detectable deposits in distant organs. This biological reality is precisely why surveillance continues well after the primary treatment is completed — and why patients who feel completely well still need their follow-up appointments.
The Role of Screening in Catching Cancer Early
The single biggest driver of localized-stage cancer diagnoses is screening. Screening tests are designed to detect cancer — or pre-cancerous changes — before symptoms develop, which is precisely when the disease is most likely to still be localized.
Major evidence-based screening programs include:
- Mammography — recommended for women aged 40–74; identifies breast cancer before lumps are large enough to feel
- Colonoscopy and stool-based DNA tests — recommended starting at age 45 for average-risk adults; catch polyps before they become cancerous and detect early colon cancers
- Low-dose CT (LDCT) lung screening — recommended for adults aged 50–80 with a significant smoking history; reduced lung cancer mortality by up to 20% in high-risk populations in the landmark National Lung Screening Trial (NCI, NLST, 2023)
- PSA test and digital rectal exam — used in prostate cancer screening; discuss appropriate timing with your doctor, as benefits depend on age and individual risk
- Cervical Pap smear and HPV co-test — recommended from age 21 to 65; every 3 years for Pap alone, or every 5 years for Pap plus HPV co-test
If you have a family history of cancer — particularly first-degree relatives (parents, siblings, children) diagnosed before age 50, or multiple family members with the same cancer — genetic counseling may be an important additional step. Mutations in genes such as BRCA1 and BRCA2 substantially elevate lifetime risk for breast and ovarian cancer. Lynch syndrome gene mutations raise colorectal, endometrial, and other cancer risks significantly. Identifying these hereditary risk factors can lead to enhanced screening schedules, earlier age at first colonoscopy, or preventive interventions. Ask your primary care doctor for a referral to a genetic counselor if cancer runs in your family.
When to See a Doctor: Warning Signs to Watch For
Screening catches many cancers before symptoms appear — but not all cancers have a recommended screening test. Recognizing warning signs and acting on them promptly can also play a role in catching cancer at a localized stage.
The American Cancer Society uses the acronym CAUTION to describe seven warning signs that deserve medical attention:
- C — Change in bowel or bladder habits
- A — A sore that does not heal
- U — Unusual bleeding or discharge
- T — Thickening or lump in the breast, testicle, or anywhere else on the body
- I — Indigestion or difficulty swallowing
- O — Obvious change in a wart, mole, or skin lesion
- N — Nagging cough or hoarseness that persists
One symptom that often concerns people but doesn’t appear on the CAUTION list is unexplained fatigue. Persistent fatigue that lasts more than a few weeks and doesn’t improve with rest can sometimes be an early sign of blood cancers like lymphoma or leukemia. On its own, fatigue has many benign explanations. But if it’s severe and accompanied by unintentional weight loss, night sweats, or swollen lymph nodes in the neck, armpits, or groin, it’s worth bringing to your doctor’s attention rather than waiting to see if it resolves.
None of the CAUTION symptoms alone signals cancer. But any that persist for two to four weeks without a clear cause deserves a medical evaluation. Here’s a guide to how urgently to act:
- Unexplained bleeding — coughing up blood, blood in stool or urine not explained by a known cause
- A lump or swelling that has appeared or grown rapidly over days
- Neurological changes: sudden vision loss, a severe new headache, or new weakness on one side of the body
- A skin sore or lesion that hasn’t healed after three to four weeks
- More than 5–10 pounds of unexplained weight loss without dietary changes
- Hoarseness or a cough that has persisted for longer than three weeks
- A new lump or thickening in the breast, armpit, groin, or neck
- Persistent unexplained fatigue lasting more than 2–3 weeks, especially with night sweats or weight loss
- Mild bowel habit changes that have lasted less than a week
- Occasional mild indigestion that is new for you but comes and goes
- A mole that looks slightly different from before but is not growing rapidly or bleeding
Frequently Asked Questions
Most localized cancers are treated with curative intent — meaning the goal is to eliminate the cancer entirely. Many types, including localized breast, prostate, and colorectal cancers, carry very high cure rates with appropriate treatment. However, some high-grade localized tumors still carry a meaningful risk of recurrence even after successful initial therapy. The word “cured” in oncology usually means no evidence of disease five or more years after treatment — but your oncologist will discuss your specific cancer type, grade, and molecular profile to give you the most accurate expectation for your individual situation.
Localized cancer is confined to the organ where it started, with no evidence of spread to lymph nodes or surrounding tissue — for example, breast cancer limited to breast tissue, or colon cancer contained within the colon wall. Regional cancer has moved beyond the primary organ into nearby lymph nodes or adjacent structures. For breast cancer, this means cancer cells found in axillary (underarm) lymph nodes; for colon cancer, it means cancer in lymph nodes alongside the bowel; for prostate cancer, it means spread to pelvic lymph nodes. Regional cancers typically require more intensive treatment — often adding chemotherapy or immunotherapy to surgery or radiation — and carry lower 5-year survival rates than their localized counterparts.
Yes, in some situations. Radiation therapy can serve as the primary treatment for certain localized cancers, including localized prostate cancer and early-stage non-small cell lung cancer treated with stereotactic body radiotherapy (SBRT). Active surveillance is a validated option for low-risk localized prostate cancer (Gleason score 6) and select thyroid cancers. The right approach depends on your specific cancer type, grade, age, and personal preferences — a decision made together with your oncologist. A second opinion at a major cancer center is always reasonable before beginning treatment.
It depends on the cancer and the treatment. Surgery for a localized tumor takes a few hours, typically with one to five days in the hospital and several weeks of recovery. Standard external beam radiation for localized cancer usually runs five to eight weeks of daily weekday sessions. Stereotactic body radiation therapy (SBRT) — used for localized lung and prostate cancer — can be completed in just five focused sessions over one to two weeks. Your care team will give you a personalized timeline once your treatment plan is finalized.
“In situ” means the cancer cells are still confined to the exact layer of tissue where they started, without invading deeper structures. Ductal carcinoma in situ (DCIS) of the breast is the best-known example. It corresponds to Stage 0 — even earlier than “localized” in the SEER system. Once cancer cells break through that membrane layer, the disease becomes invasive and clinical staging begins. Whether an in situ diagnosis needs treatment depends on the cancer type, size, grade, and individual risk factors — and is a conversation worth having thoroughly with your oncologist or seeking a second opinion on, since approaches to in situ disease vary between institutions.
Receiving a cancer diagnosis at any stage is a life-changing event. But if your cancer has been identified as localized, you’re starting from a position where treatment options are broad and the goal — for most cancer types — is to cure the disease. The survival data from the NCI and the American Cancer Society offer real context: they show what has happened for large groups of people at similar stages of similar cancers, and the trend over the past two decades has been consistently toward better outcomes.
Ask your oncologist specific questions — not just about the stage, but about the grade, the molecular profile, the surgical margins, and whether a second opinion at a major cancer center might be worthwhile. Stay on top of your follow-up surveillance schedule. And if you’re not yet current on cancer screenings, make that appointment. The best localized cancer diagnosis is the one caught before you ever develop a symptom.
The content on Horizon Health Guide is intended for informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the guidance of your physician or another qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website. If you think you may have a medical emergency, call your doctor, go to the emergency department, or call 911 immediately.
References
- National Cancer Institute. (2023). SEER Cancer Statistics Review. National Institutes of Health. https://seer.cancer.gov/
- American Cancer Society. (2024). Cancer Facts & Figures 2024. https://www.cancer.org/research/cancer-facts-statistics/
- National Cancer Institute. (2023). What Is Cancer? https://www.cancer.gov/about-cancer/understanding/what-is-cancer
- Mayo Clinic. (2023). Cancer diagnosis and treatment. https://www.mayoclinic.org/diseases-conditions/cancer/diagnosis-treatment/drc-20370594
- Centers for Disease Control and Prevention. (2023). Cancer Data and Statistics. https://www.cdc.gov/cancer/
- Cleveland Clinic. (2023). Cancer Staging. https://my.clevelandclinic.org/health/diagnostics/21479-cancer-staging
- National Cancer Institute. (2023). Lung Cancer Screening (PDQ) — National Lung Screening Trial. https://www.cancer.gov/types/lung/patient/lung-screening-pdq
- American Cancer Society. (2023). Guidelines for the Early Detection of Cancer. https://www.cancer.org/cancer/screening/american-cancer-society-guidelines-for-the-early-detection-of-cancer.html
- American Joint Committee on Cancer. (2023). AJCC Cancer Staging Manual, 8th Edition.
- National Cancer Institute. (2022). Understanding Cancer Prognosis. https://www.cancer.gov/about-cancer/diagnosis-staging/prognosis