Hormones and Blood Sugar: The Body’s Glucose Control System
Blood sugar regulation is not a simple on/off switch — it is a continuous, multi-hormone balancing act that the body performs thousands of times every day. Hormones and blood sugar are so tightly linked that nearly every major endocrine gland in the body contributes in some way to keeping glucose within a healthy range. Understanding which hormones raise glucose, which lower it, and how disruptions to hormonal balance drive diabetes and prediabetes gives people with these conditions a deeper framework for interpreting their daily glucose readings and making informed decisions about lifestyle and treatment. Our guide on how the body controls blood sugar provides the foundational overview; this article goes deeper into the specific hormones involved and what happens when each one is dysregulated.
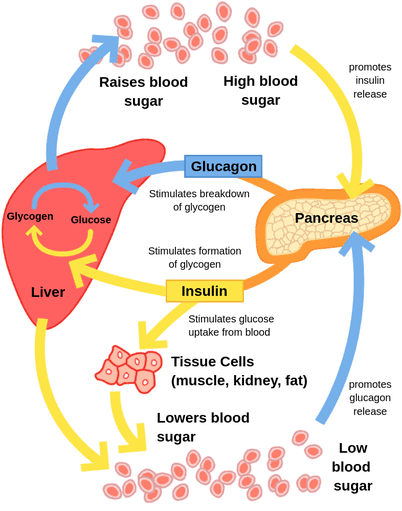
Insulin: The Only Hormone That Lowers Blood Glucose
Insulin, produced by beta cells in the pancreas, is the only hormone in the human body whose primary role is to lower blood glucose. When glucose enters the bloodstream after a meal, insulin is released in response, binding to receptors on muscle, fat, and liver cells and allowing glucose to enter those cells to be used for energy or stored as glycogen (in liver and muscle) or fat. Without insulin, cells cannot access glucose efficiently — the glucose piles up in the blood, producing hyperglycemia, while cells simultaneously starve for energy. This is the core problem in both Type 1 diabetes (where beta cells are destroyed by autoimmune attack, eliminating insulin production entirely) and Type 2 diabetes (where cells become resistant to insulin’s signal, and beta cells eventually exhaust themselves trying to compensate with ever-higher insulin output). Our guide on what is insulin covers the physiology in detail. Beyond its direct glucose-lowering action, insulin also suppresses the liver’s production of new glucose (gluconeogenesis) and inhibits the breakdown of fat — which is why insulin deficiency produces not only hyperglycemia but also ketone production from unregulated fat catabolism.
Glucagon: Insulin’s Direct Counterpart
Glucagon, produced by alpha cells in the pancreas — cells that sit adjacent to the insulin-producing beta cells — is the primary hormone that raises blood glucose when levels fall too low. Glucagon signals the liver to break down stored glycogen and release glucose into the bloodstream (glycogenolysis), and also stimulates the liver to synthesize new glucose from amino acids and other substrates (gluconeogenesis). In people without diabetes, glucagon and insulin work in tight opposition: as insulin rises after a meal, glucagon is suppressed; as glucose falls between meals or during fasting, glucagon rises and insulin falls, maintaining blood sugar in the normal range. In Type 1 diabetes, this counter-regulatory balance is disrupted in a critical way: not only does insulin secretion fail, but glucagon secretion becomes dysregulated — failing to suppress after meals (contributing to post-meal hyperglycemia) and failing to rise appropriately in response to hypoglycemia (contributing to the risk of severe low blood sugar). Our guide on what is blood sugar explains how these paired hormones maintain the narrow glucose window that keeps the body functioning optimally.

Cortisol: The Stress Hormone That Raises Blood Sugar
Cortisol, released from the adrenal glands in response to stress (physical or psychological), is one of the most powerful counter-regulatory hormones affecting blood sugar. Its glucose-raising effects are multiple and substantial: cortisol directly stimulates gluconeogenesis in the liver; it inhibits insulin signaling in peripheral tissues, producing a form of transient insulin resistance; and it reduces the uptake of glucose by muscle cells, leaving more glucose circulating in the blood. These effects make evolutionary sense — in a fight-or-flight scenario, the body needs ready fuel available — but they become problematic in the context of modern chronic psychological stress or in people with diabetes who already have impaired insulin responses. Chronic cortisol elevation, whether from sustained psychological stress, Cushing’s syndrome (excess cortisol from a tumor), or long-term corticosteroid medication use, consistently worsens glycemic control in people with diabetes and can push prediabetes toward full Type 2 diabetes. People who monitor blood sugar often notice that glucose readings are significantly higher on high-stress days even when diet and exercise are identical — this is cortisol’s direct effect on insulin resistance and hepatic glucose output. Our guide on illness and blood sugar changes covers how this cortisol mechanism explains the glucose elevation that occurs during infection and illness, representing the same physiological pathway triggered in a different context.
Epinephrine (Adrenaline): The Acute Glucose-Raising Hormone
Epinephrine — also known as adrenaline — is released from the adrenal medulla within seconds of a perceived threat, producing the immediate physical changes associated with acute stress: increased heart rate, dilated pupils, redirected blood flow to muscles, and rapidly elevated blood glucose. Like cortisol, epinephrine raises blood glucose by stimulating glycogenolysis in the liver (breakdown of stored glycogen into glucose), stimulating glucagon secretion, and inhibiting insulin secretion from the pancreas. Unlike cortisol’s gradual, sustained effect, epinephrine’s glucose-raising action is rapid and intense — blood glucose can rise by 50 mg/dL or more within minutes of an acute stress response. This explains why people with diabetes sometimes see surprisingly high glucose readings after a stressful meeting, an anxiety-provoking event, or an acute physical scare. Epinephrine also plays a critical role in the body’s defense against hypoglycemia: when blood glucose falls below a threshold of roughly 65 mg/dL, epinephrine is released, producing the familiar hypoglycemia symptoms of trembling, rapid heart rate, sweating, and anxiety — which serve as warning signals to prompt glucose intake. Our guide on hypoglycemia symptoms, causes and what to do covers this counter-regulatory response in detail and explains what to do when it occurs.
Growth Hormone: The Overnight Glucose Disruptor
Growth hormone, released in pulses from the pituitary gland — most prominently during deep sleep in the early morning hours — raises blood glucose through the same insulin-antagonist mechanisms as cortisol: it suppresses insulin action in peripheral tissues and stimulates hepatic glucose output. In people without diabetes, this is managed by a compensatory rise in insulin secretion. In people with Type 1 or Type 2 diabetes, this growth hormone-driven glucose rise between approximately 3 and 8 a.m. can produce the phenomenon known as the dawn phenomenon — a characteristic early-morning rise in blood sugar that occurs even without any food intake and that is sometimes mistaken for poor overnight insulin dosing or nocturnal hypoglycemia followed by rebound. Understanding that the dawn phenomenon is hormonally driven — specifically by growth hormone and to a lesser extent by cortisol’s morning surge — is important because it informs the management approach: the solution is typically timed insulin or medication adjustment rather than dietary changes. Our guide on morning blood sugar: what it means covers the dawn phenomenon and the Somogyi effect (rebound hyperglycemia from overnight hypoglycemia) as the two most common explanations for unexpectedly high morning glucose readings.
Sex Hormones: Estrogen, Testosterone, and Glucose Regulation
The sex hormones — estrogen, progesterone, and testosterone — each affect insulin sensitivity in ways that produce clinically meaningful differences in blood sugar management across sex and reproductive stage. Estrogen generally improves insulin sensitivity, which helps explain why premenopausal women with Type 2 diabetes tend to have somewhat better metabolic profiles than men of the same age. However, the relationship is complex: estrogen also affects the uptake of glucose into specific tissues and modulates glucagon secretion, and the interaction between estrogen and glucose metabolism is highly dependent on the form of estrogen, its concentration, and the presence of other hormones. Progesterone, in contrast, has insulin-antagonistic effects — which explains why blood glucose tends to rise in the second half of the menstrual cycle (the luteal phase, when progesterone is dominant) and during pregnancy, when placental progesterone combined with other placental hormones produces the insulin resistance that can progress to gestational diabetes in susceptible individuals. Testosterone affects insulin sensitivity in both sexes: in men, low testosterone is associated with increased insulin resistance and higher diabetes risk; in women with polycystic ovary syndrome (PCOS), elevated androgens (including testosterone) are a major driver of the insulin resistance that makes PCOS one of the strongest prediabetes risk factors in reproductive-age women. Understanding these hormonal patterns helps explain why blood sugar management needs may change across life stages — particularly around menstruation, pregnancy, and menopause — and why hormonal conditions like PCOS significantly elevate diabetes risk beyond what is explained by weight alone. Our guide on what is insulin resistance provides the mechanistic context for understanding how these hormonal influences translate into impaired insulin signaling at the cellular level.
Thyroid Hormones: Metabolic Rate and Blood Sugar
Thyroid hormones (primarily thyroxine, T4, and its active form triiodothyronine, T3) regulate metabolic rate throughout the body, affecting how quickly glucose is absorbed from the gastrointestinal tract, how rapidly liver glycogen is broken down, and how sensitively peripheral tissues respond to insulin. Hyperthyroidism — excess thyroid hormone — accelerates all of these processes: glucose absorption increases, liver glycogen breakdown is faster, and counter-regulatory hormone effects are amplified, producing elevated blood glucose that can cause or worsen diabetes in predisposed individuals. Hypothyroidism — insufficient thyroid hormone — slows metabolic rate, reduces glucose clearance, and is associated with elevated triglycerides and LDL cholesterol, all of which increase cardiovascular and metabolic disease risk. Because hypothyroidism often develops slowly and subtly, and because its symptoms (fatigue, weight gain, cold intolerance, brain fog) overlap with symptoms of uncontrolled diabetes, thyroid function testing is often recommended as part of diabetes workup and monitoring — particularly in women over 40, who are at highest risk for autoimmune thyroid disease. Our guide on dehydration and blood sugar explains a similar confounding-variable principle: when a single symptom (like fatigue or elevated glucose) can have multiple hormonal or physiological causes, targeted testing is essential for identifying the actual driver rather than treating the symptom alone.
How Hormonal Dysregulation Drives Type 2 Diabetes
Type 2 diabetes is fundamentally a disease of hormonal dysregulation, and the pathway from normal glucose metabolism to full diabetes involves multiple hormonal failures occurring in sequence. The sequence typically begins with the development of insulin resistance — cells becoming less responsive to insulin’s glucose-uptake signal, often driven by excess adipose tissue (particularly visceral fat), physical inactivity, and genetic predisposition. In response to insulin resistance, beta cells compensate by producing more insulin, maintaining normal blood glucose for years. As insulin resistance worsens, beta cells are pushed beyond their capacity and begin to lose function — at this stage, prediabetes develops (fasting glucose 100–125 mg/dL, A1C 5.7–6.4%). Eventually, beta cell function declines sufficiently that insulin output is inadequate to compensate for the degree of insulin resistance, and blood glucose rises persistently into the diabetic range (fasting glucose ≥126 mg/dL, A1C ≥6.5%). Meanwhile, glucagon regulation also fails — alpha cells become resistant to the suppressive effect of insulin on glucagon secretion, and glucagon levels remain inappropriately elevated after meals, adding hepatic glucose output at exactly the time the body should be clearing glucose from the blood. This combined failure of insulin secretion and glucagon regulation explains why blood sugar control in Type 2 diabetes becomes progressively harder to manage without pharmacological intervention as the disease advances. Our guide on what is prediabetes covers the inflection point where hormonal compensation begins to fail and intervention can still meaningfully alter the trajectory.
Managing Blood Sugar in the Context of Hormonal Variability
For people with diabetes, understanding that blood glucose readings are not determined solely by food and medication — but also by hormonal fluctuations driven by stress, sleep, illness, sex hormones, and thyroid function — reframes what good glucose management actually looks like. On high-stress days or illness days, glucose will be higher even with perfect dietary adherence; during the luteal phase of the menstrual cycle, more insulin may be needed; after a poor night’s sleep, growth hormone secretion patterns shift and morning glucose may be higher than usual; during the development of hypothyroidism, glucose control may worsen even with unchanged diet and medication. Recognizing these hormonal drivers allows for a more nuanced and compassionate interpretation of blood glucose data — distinguishing between glucose elevation that reflects a management failure and elevation that reflects a physiological hormonal response that requires a different kind of adjustment. Systematic tracking of glucose alongside notes about stress, sleep quality, illness, menstrual cycle phase, and other relevant factors — as described in our guide on how to track your blood sugar numbers — creates the longitudinal data needed to identify these patterns and discuss them meaningfully with a healthcare provider. Our guide on what causes high blood sugar covers the full range of non-dietary contributors to hyperglycemia, of which hormonal drivers represent one of the most significant and most frequently overlooked categories.
Incretins: The Gut Hormones That Amplify Insulin Release
Beyond the pancreatic hormones insulin and glucagon, a group of gut-derived hormones called incretins play a crucial and often underappreciated role in blood sugar regulation. The two primary incretins are glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), both released from cells in the small intestinal lining in response to food — particularly carbohydrates and fats. Their primary function is to amplify insulin secretion from beta cells in a glucose-dependent manner, meaning they stimulate insulin release only when blood glucose is elevated (a safety feature that prevents hypoglycemia from incretin action alone). GLP-1 also suppresses glucagon secretion, slows gastric emptying (reducing the speed at which glucose enters the bloodstream from digestion), and produces satiety signals that reduce food intake. In people with Type 2 diabetes, the incretin response is significantly blunted — particularly the GLP-1 response — meaning that insulin secretion after meals is less amplified than in people without diabetes, contributing to post-meal hyperglycemia. This understanding of incretin biology has driven two major classes of diabetes medications: GLP-1 receptor agonists (semaglutide, liraglutide, dulaglutide), which mimic the effects of GLP-1; and DPP-4 inhibitors (sitagliptin, saxagliptin), which prevent the rapid breakdown of naturally secreted GLP-1. The impressive weight-loss and cardiovascular benefits of GLP-1 receptor agonists — now widely used beyond diabetes for obesity treatment — are direct reflections of GLP-1’s role in appetite regulation and cardiovascular protection. Our guide on blood sugar after meals covers the post-meal glucose dynamics that incretins directly regulate, and explains what normal versus abnormal post-meal readings look like in practice.
Leptin, Adiponectin, and the Hormonal Role of Body Fat
Adipose tissue is not merely a passive energy store — it is an active endocrine organ that secretes hormones called adipokines, which profoundly influence insulin sensitivity and glucose metabolism. Two of the most important adipokines are leptin and adiponectin, which have opposing effects on insulin action and metabolic health. Leptin is secreted by fat cells in proportion to fat mass and signals the hypothalamus to reduce appetite and increase energy expenditure — its role in energy balance is crucial. However, in the setting of obesity, leptin resistance develops, where the brain no longer responds appropriately to leptin’s satiety signals despite very high circulating levels. Leptin resistance also has direct effects on insulin signaling and contributes to the metabolic dysfunction associated with excess adipose tissue. Adiponectin, in contrast, has strongly insulin-sensitizing effects: it promotes fatty acid oxidation in muscle, reduces hepatic glucose production, and improves cellular insulin signaling. In people with obesity and Type 2 diabetes, adiponectin levels are paradoxically low — inversely related to fat mass — which means that the very people who would most benefit from adiponectin’s insulin-sensitizing effects have the least of it. Weight loss — even modest reductions of 5–10% of body weight — raises adiponectin levels and reduces the insulin resistance that adiponectin deficiency contributes to. Our guide on insulin resistance covers how adipose tissue dysfunction feeds into insulin signaling failure, and our guide on what the A1C test means provides the monitoring framework for tracking how lifestyle changes that improve adipokine balance translate into measurable improvements in long-term blood sugar control.
Hormones, Blood Sugar, and Sleep: A Critical Connection
Sleep deprivation and poor sleep quality — both increasingly prevalent in modern populations — produce significant hormonal disruptions that directly worsen insulin sensitivity and blood sugar control. Even a single night of four to five hours of sleep has measurable effects: cortisol levels rise (as the body’s stress response activates in the absence of adequate rest), growth hormone secretion patterns become irregular, and insulin sensitivity in peripheral tissues can decline by 20–25% compared to a well-rested baseline. Over time, chronic sleep deprivation is associated with higher A1C levels in people with diabetes, higher rates of progression from prediabetes to Type 2 diabetes, and greater difficulty achieving glucose targets despite appropriate medication. Sleep also directly affects the hormones that regulate appetite: sleep-deprived individuals show elevated ghrelin (the hunger-stimulating hormone) and reduced leptin (the satiety hormone), producing increased hunger and food intake that compounds the insulin resistance effect. The relationship between sleep and blood sugar is bidirectional — uncontrolled diabetes also disrupts sleep through nocturia (frequent nighttime urination from high glucose), nighttime hypoglycemia, and the pain from neuropathy — creating a cycle that requires attention on both sides. Managing blood sugar and managing sleep quality are not separate tasks in diabetes care; they reinforce each other, and improvements in one reliably support improvements in the other. Our guide on what causes high blood sugar includes sleep deprivation among the non-dietary drivers that frequently surprise people with diabetes when they see higher glucose readings after poor sleep nights.
Working With Your Hormonal Profile in Diabetes Management
No two people with diabetes have the same hormonal landscape — and no single person’s hormonal profile stays constant over time. A 35-year-old woman with Type 2 diabetes and PCOS managing the insulin resistance driven by androgen excess will face different glucose dynamics than a 65-year-old man with hypothyroidism and cortisol dysregulation from chronic work stress. Both have “diabetes,” but the hormonal contributors differ substantially, and the most effective management strategy for each will reflect those differences. This is why the emerging concept of precision diabetes care — matching treatment strategy to the individual’s specific hormonal, metabolic, and genetic profile — promises to improve on the population-average approaches that characterize current standard of care. For people living with diabetes now, the practical implication is to bring a curious, investigative mindset to glucose data: when glucose is unexpectedly elevated despite consistent diet and medication, asking “what hormonal factor might be at play?” is more productive than simply concluding that the diabetes is worsening. Sharing this kind of contextual observation with a healthcare provider — “my glucose runs higher during the luteal phase of my cycle” or “my readings are consistently 30 points higher on high-stress workdays” — gives the provider actionable information that moves management toward something genuinely tailored. The framework for understanding how multiple factors interact with glucose — diet, hormones, activity, stress, sleep, illness, medications — is what transforms blood sugar monitoring from a passive record-keeping exercise into a powerful tool for improving health. Our guide on fasting blood sugar explained provides the reference values and interpretation framework that anchors this kind of systematic hormonal investigation in concrete numbers.
Sources: American Diabetes Association. “Standards of Medical Care in Diabetes.” Diabetes Care 2024. | Endocrine Society — Hormones and Endocrine Function. | National Institute of Diabetes and Digestive and Kidney Diseases — What Is Diabetes. | Mayo Clinic — Diabetes: Symptoms and Causes. | Polonsky KS. “The past 200 years in diabetes.” N Engl J Med 2012.