Hearing the words “you have cancer” changes everything — even when a doctor quickly adds “and we caught it early.” A stage 1 diagnosis brings its own wave of questions: What exactly does stage 1 mean? What are my chances? What does life look like from here?
If you or someone you love has just received a stage 1 cancer diagnosis, this guide is for you. We’ll walk through what stage 1 actually means medically, survival rates broken down by cancer type, how diagnosis and treatment typically work, and — just as importantly — what you can realistically expect in the weeks ahead.
Most stage 1 cancers have a 5-year survival rate above 90%, and treatment is nearly always given with the intent to cure. But a short answer isn’t enough when it’s your health. You deserve the full picture.
What Does Stage 1 Cancer Mean?
Cancer staging describes how far a cancer has grown and whether it has moved beyond its original location. The most widely used framework is the TNM system, developed by the American Joint Committee on Cancer (AJCC):
- T (Tumor): How large and invasive the primary tumor is. T1 means small; T4 means large or deeply invasive.
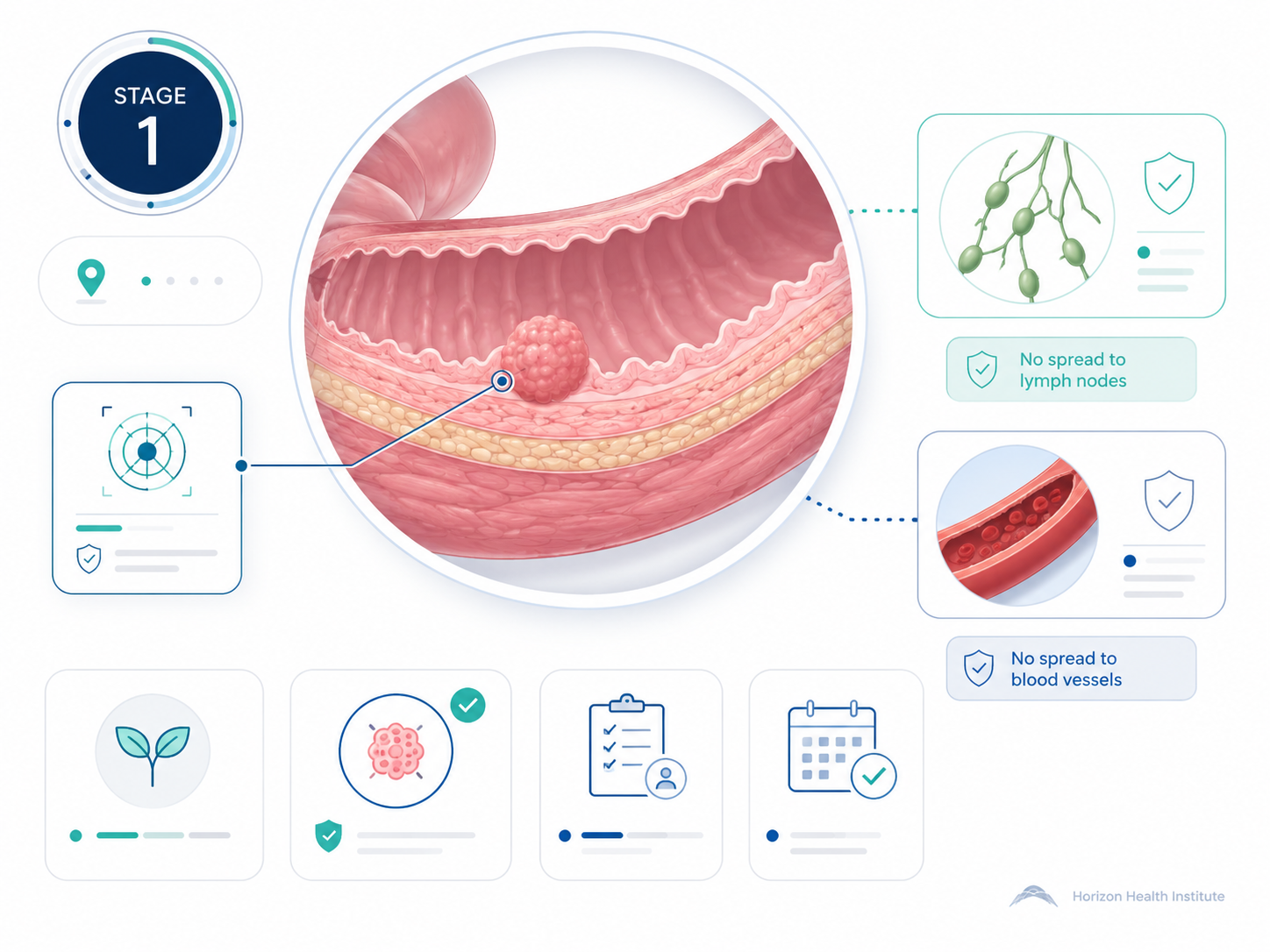
- N (Node): Whether cancer has reached nearby lymph nodes. N0 means none; N3 means extensive spread.
- M (Metastasis): Whether cancer has spread to distant organs. M0 means no distant spread; M1 means it has.
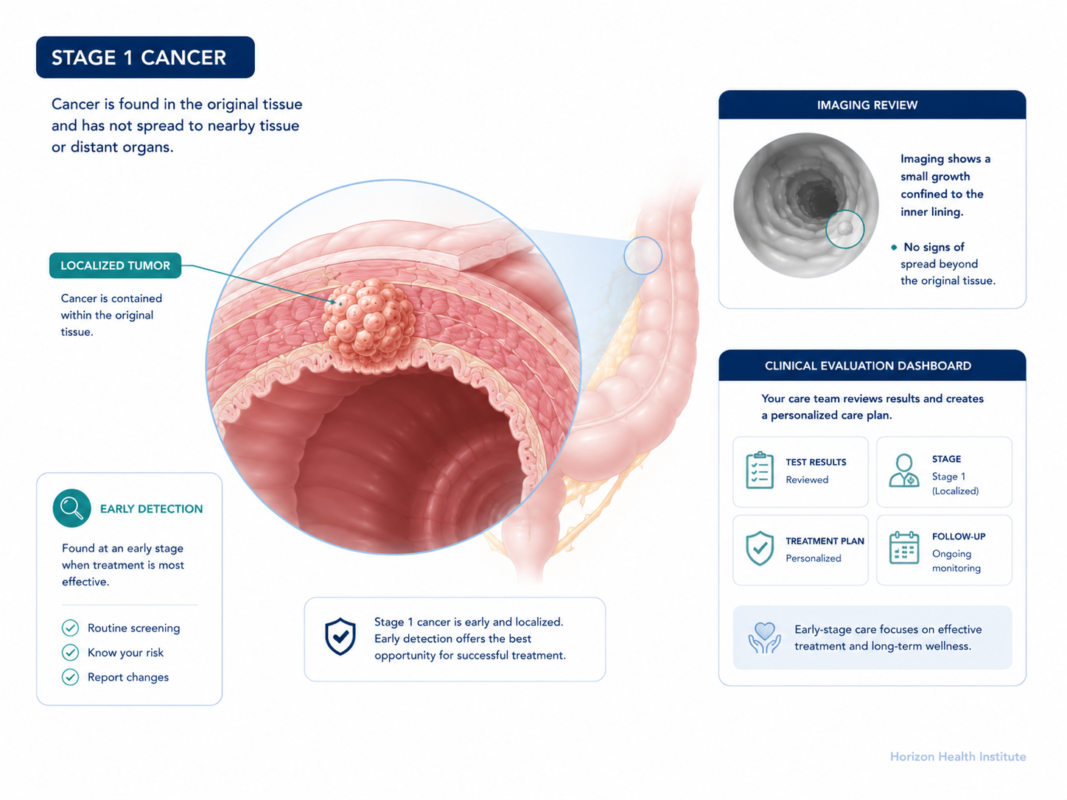
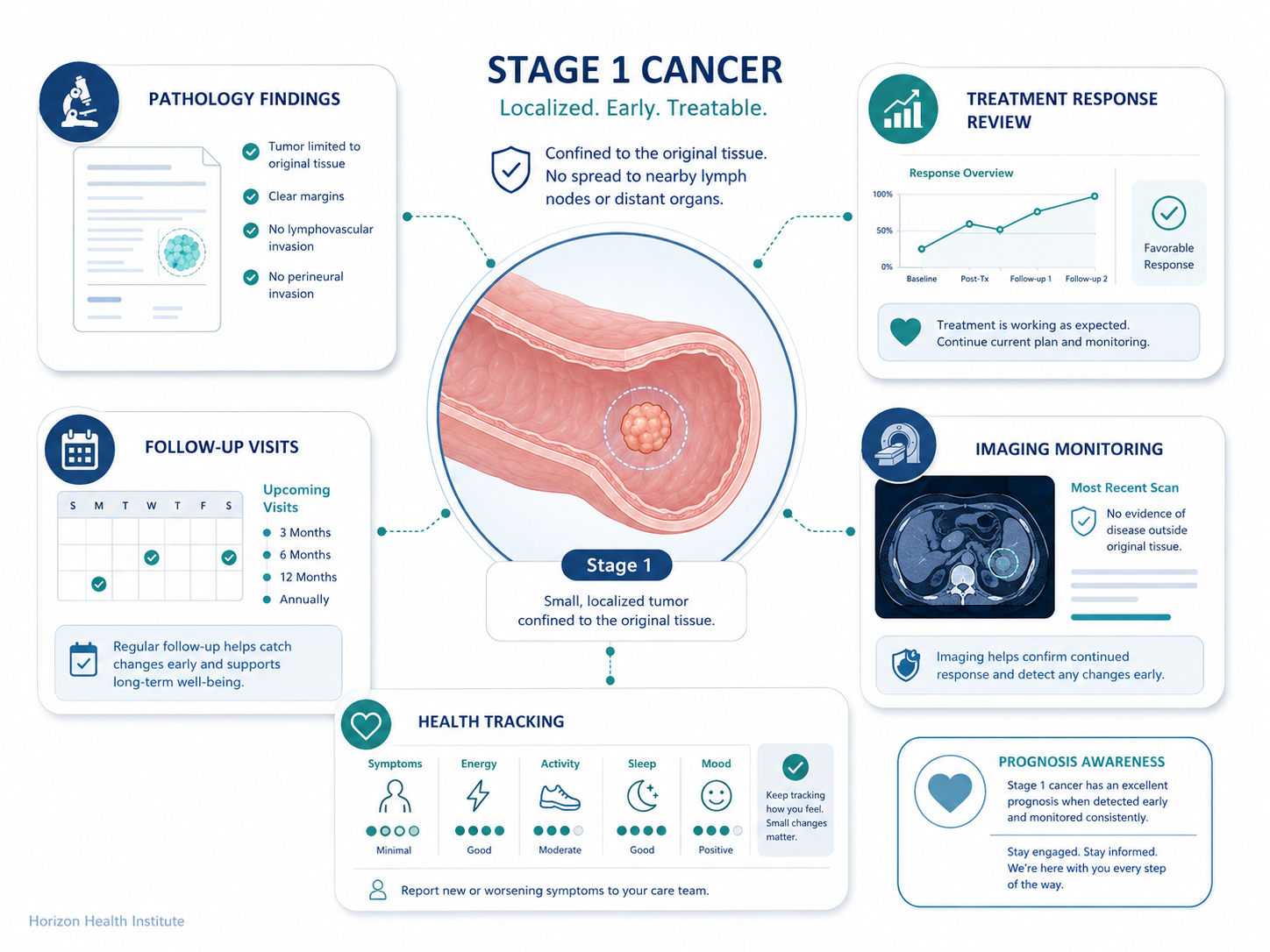
Stage 1 = T1 or T2 + N0 + M0. The tumor is relatively small, hasn’t reached the lymph nodes, and hasn’t traveled to other parts of the body. This is a contained cancer — and a contained cancer is one doctors can most reliably eliminate.
Worth noting: not all cancers use the same staging numbers. Most solid tumors (breast, lung, colon, prostate) follow stages 1 through 4. Blood cancers like leukemias and lymphomas use different systems entirely. This guide focuses on solid tumor cancers staged using the TNM system.
If you want to understand the full picture of what “localized” cancer means — and how doctors determine whether cancer is still contained — our localized cancer guide explains how doctors determine if cancer is still contained and what that means for your diagnosis.
Stage 1A vs Stage 1B — What’s the Difference?
Some cancers split stage 1 into two substages: 1A and 1B. The difference usually comes down to tumor size or depth of invasion. The important thing to know: both are still stage 1, and both are treated with the intent to cure.
Lung Cancer: Where the Difference Matters Most
- Stage 1A: Tumor 3 cm or smaller, not involving the main bronchus. Five-year survival: approximately 92%.
- Stage 1B: Tumor between 3 and 4 cm, possibly with additional features. Five-year survival: approximately 68%.
That gap in survival rates shapes the treatment plan — including whether targeted therapy after surgery might be recommended.
Breast Cancer: Often a Small Distinction
- Stage 1A: Tumor 2 cm or smaller, no lymph node involvement.
- Stage 1B: Small or no detectable primary tumor, but microscopic cancer clusters (under 2 mm) found in one or two lymph nodes.
In practice, treatment for stage 1A and 1B breast cancer is often identical. The five-year survival rate for both is approximately 99%.
Cervical Cancer: Microscopic vs Visible
- Stage 1A: Detected only under a microscope; too small to see with the naked eye.
- Stage 1B: Visible tumor still fully confined to the cervix, with subdivisions by size (1B1, 1B2, 1B3).
Ask your oncologist specifically which substage you have and what it means for your treatment plan. In most cases, 1A and 1B are handled similarly — both with curative intent.
Stage 1 Cancer Survival Rates by Type
Survival rates are the first thing most people search for after a cancer diagnosis — and understandably so. Before reading the table, a few important points:
What “5-year relative survival rate” means: This is the percentage of people with a specific cancer who are alive five years after diagnosis, compared to people of similar age and sex without cancer. These are population-level statistics — they do not predict what will happen to any individual. Your personal prognosis depends on tumor grade, molecular subtype, treatment quality, your age, and your overall health.
| Cancer Type | Stage 1 — 5-Year Survival | Stage 4 — 5-Year Survival |
|---|---|---|
| Breast | ~99% | ~28% |
| Lung | ~92% (1A) / ~68% (1B) | ~7% |
| Colorectal | ~90% | ~14% |
| Prostate | ~nearly 100% | ~32% |
| Melanoma | ~98–99% | ~30% |
| Ovarian | ~92% | ~31% |
| Bladder | ~88% | ~8% |
| Thyroid | ~nearly 100% | ~55% |
| Cervical | ~80–93% | ~17% |
| Stomach | ~75% | ~6% |
Source: NCI SEER Program 2023; American Cancer Society Cancer Statistics 2024
The contrast between stage 1 and stage 4 survival is striking. For most cancer types, catching the disease at stage 1 means survival rates that are four to ten times higher. This is the clearest argument for screening, regular checkups, and not dismissing symptoms.
Factors that influence your individual prognosis at stage 1:
- Tumor grade: How abnormal the cells look — high-grade tumors grow faster
- Molecular subtype: Triple-negative breast cancer is more aggressive than HR+ types, even at stage 1
- Age and general health: Affect both treatment options and recovery
- Access to care: Treatment at a high-volume cancer center is associated with better outcomes
- Genetic factors: BRCA mutations affect recurrence risk in breast and ovarian cancers
How Stage 1 Cancer Is Diagnosed
By the time you’ve been told you’re stage 1, your medical team has already worked through a specific diagnostic sequence. Understanding that process helps make sense of why certain tests were done — and what might still be coming.
Step 1: Initial Detection
Stage 1 cancer is most often found through routine screening — mammogram, colonoscopy, PSA test, Pap smear, or low-dose CT scan — before symptoms appear. Sometimes it’s discovered when a patient reports a symptom (a lump, unusual bleeding, a persistent cough), or found incidentally on imaging done for another reason.
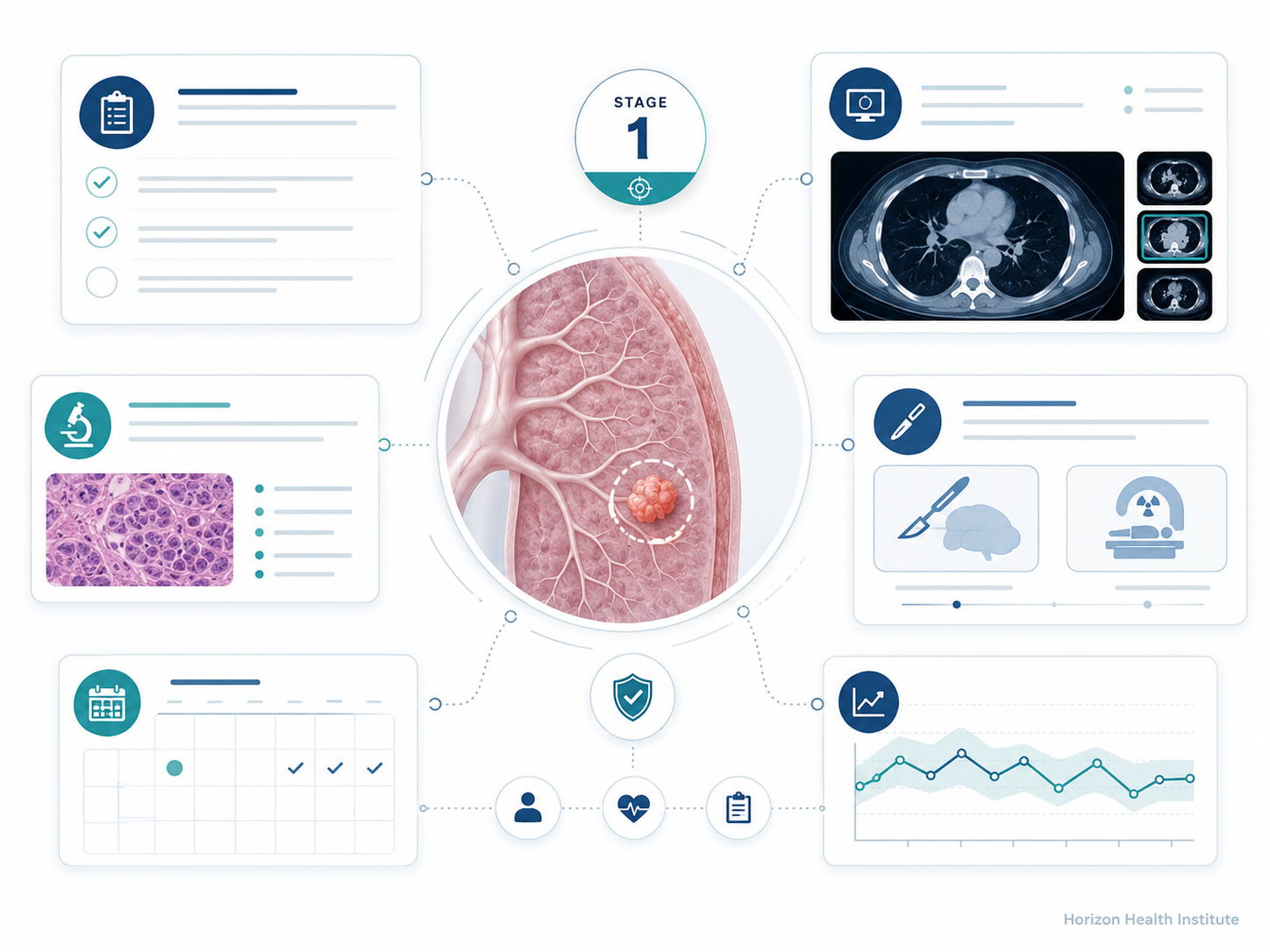
Step 2: Diagnostic Imaging
An abnormal finding triggers detailed imaging. CT, MRI, or ultrasound maps the size and location of the suspicious area and checks for any visible spread. Imaging alone cannot confirm cancer — it identifies where to look next.
Step 3: Biopsy
A biopsy is the definitive diagnostic step. Tissue from the suspicious area is examined by a pathologist, who determines: whether cancer is present, the cancer type and origin, and the grade — how abnormal the cells appear, which indicates aggressiveness.
Step 4: Lymph Node Assessment
At stage 1, confirming that lymph nodes are clear (N0) is essential. For breast cancer and melanoma, doctors often perform a sentinel lymph node biopsy — a targeted procedure identifying the first one or two lymph nodes that would catch spreading cancer cells. If those are cancer-free, it strongly suggests the entire lymph node network is unaffected.
Step 5: Confirming No Distant Spread
A PET scan, bone scan, or blood tumor markers may be ordered to confirm no distant metastasis. For many stage 1 cancers, the risk of distant spread is low enough that extensive additional imaging isn’t required.
The stage assigned before surgery — based on imaging and biopsies — is the clinical stage. After surgery, the pathologist examines the removed tissue and lymph nodes, producing the pathologic stage, which is more accurate. Occasionally, a cancer believed to be stage 1 before surgery is upstaged after full pathologic review.
Stage 1 Cancer Treatment Options
Treatment for stage 1 cancer is almost always pursued with curative intent — the aim is to eliminate all cancer cells, not just slow the disease. Treatment at this stage tends to be less intensive than at later stages, and many patients find it more manageable than they feared.
Surgery
Surgery is the cornerstone of stage 1 treatment for most solid tumors. The goal: remove the tumor completely with clear margins — meaning cancer-free tissue surrounds the removed tumor on all sides. Common stage 1 procedures include lumpectomy (breast), wide local excision (melanoma), lobectomy or segmentectomy (lung), and partial nephrectomy (kidney). Modern robotic and laparoscopic techniques make many stage 1 surgeries minimally invasive with shorter recovery times.
Radiation Therapy
Radiation is frequently added after surgery (adjuvant radiation) to destroy any remaining microscopic cancer cells. It’s standard after lumpectomy for breast cancer and used in some cervical and prostate cancer cases. Precision techniques like intensity-modulated radiation therapy (IMRT) protect surrounding healthy tissue.
Chemotherapy
At stage 1, chemotherapy is less commonly needed. Many patients skip it entirely. It may be recommended for certain high-risk stage 1 tumors — triple-negative breast cancer, some colorectal cancers — when features suggest elevated recurrence risk.
Hormone Therapy
For hormone receptor-positive (HR+) breast cancer, hormone-blocking therapy (tamoxifen or aromatase inhibitors) is standard after surgery, continuing for 5 to 10 years. For some prostate cancer cases, hormone therapy is combined with radiation.
Targeted Therapy
Some stage 1 cancers with specific genetic mutations respond to targeted drugs. Patients with EGFR-positive non-small cell lung cancer (stage 1B) may receive osimertinib (Tagrisso) after surgery for up to three years — shown in the ADAURA trial to significantly reduce recurrence risk.
Active Surveillance
For very low-risk cancers, watchful monitoring may be recommended instead of immediate treatment — common for low-risk prostate cancer and small papillary thyroid cancers. Active surveillance is not passive; it involves scheduled PSA tests, biopsies, and imaging, with treatment beginning only if the cancer shows signs of progression.
Can Stage 1 Cancer Be Cured?
Oncologists tend to use careful language around “cure.” Most won’t declare a cancer cured until 5 to 10 years have passed without recurrence, because some cancers can return years later. Instead, you’ll hear terms like “no evidence of disease (NED)” or “complete remission.”
What that means in practice for stage 1:
- Treatment is pursued with curative intent — the goal is complete elimination, not just control
- Most patients achieve NED status after completing treatment
- Recurrence rates are significantly lower at stage 1 than at later stages
Follow-up surveillance continues after treatment — typically every 3 to 6 months for the first few years, then annually. If cancer does return, recurrence after stage 1 treatment often comes back as a localized recurrence rather than automatically as advanced disease — and today’s treatments for recurrent cancers have improved substantially.
For a deeper understanding of what cancer spread looks like and what modern treatment can accomplish when cancer does reach distant sites, our metastatic cancer guide covers the full picture.
What Happens After a Stage 1 Diagnosis — Your Next Steps
The diagnosis is confirmed. The stage is set. Now what?
Days 1–7: Give Yourself Space
Fear, disbelief, anger, and even strange moments of calm are all normal responses to a cancer diagnosis. There is no correct emotional reaction. Write down every question as it surfaces — you’ll have more than you think, and your oncologist expects them.
Week 2–4: Build Your Medical Team
For stage 1 cancer, you’ll typically work with a medical oncologist, surgical oncologist, radiation oncologist (if needed), patient navigator, and oncology social worker. A second opinion from a major cancer center is standard practice and strongly encouraged — it’s not offensive to your doctor, and it may confirm the plan or surface an alternative approach.
Questions to Ask Your Oncologist
- What is my exact stage and substage, and what does it mean for my specific situation?
- What are the treatment options, and which do you recommend — and why?
- Is the goal of treatment curative or something else?
- What are the likely side effects, both short-term and long-term?
- Will I need surgery, radiation, chemotherapy — or a combination?
- Should I consider a clinical trial?
- What follow-up schedule will I need after treatment ends?
- Are there genetic tests I should have?
- Are there lifestyle changes that could improve my outcome?
- How will we know if treatment has worked?
Frequently Asked Questions
Sources
- National Cancer Institute — Cancer Staging. cancer.gov
- NCI SEER Program — Cancer Stat Facts: 5-Year Relative Survival Rates by Stage (2023). seer.cancer.gov
- American Cancer Society — Cancer Facts & Figures 2024. cancer.org
- American Cancer Society — Survival Rates by Cancer Type. cancer.org
- Mayo Clinic — Cancer staging: What it means and how it’s used. mayoclinic.org
- ASCO Cancer.Net — Understanding Cancer Staging. cancer.net