Getting a stage 2 cancer diagnosis carries a different emotional weight than stage 1. “Stage 2” sounds more serious — and in some ways it is. But it does not mean what many people fear when they first hear it. Stage 2 cancer is not advanced cancer. It is not metastatic cancer. It is still disease that doctors treat with the goal of cure.
If your cancer has been staged at 2 — or if you’ve received news that your staging has been revised upward from stage 1 — this guide gives you a clear, honest picture of what that means: what’s different, what stays the same, and what comes next.
Stage 2 cancer is locoregional — it has not spread to distant organs. Treatment is given with curative intent in almost all cases. Survival rates for most stage 2 cancers remain above 75%, and for breast and prostate cancer they are near 100%.
What Does Stage 2 Cancer Mean?
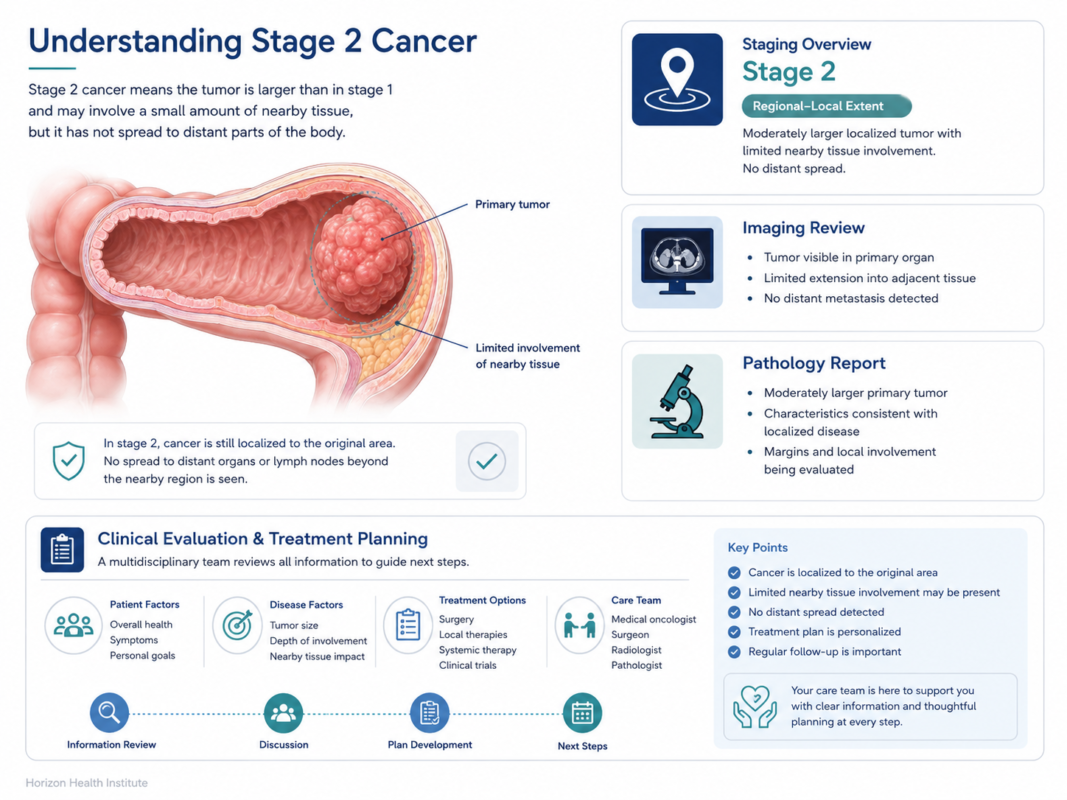
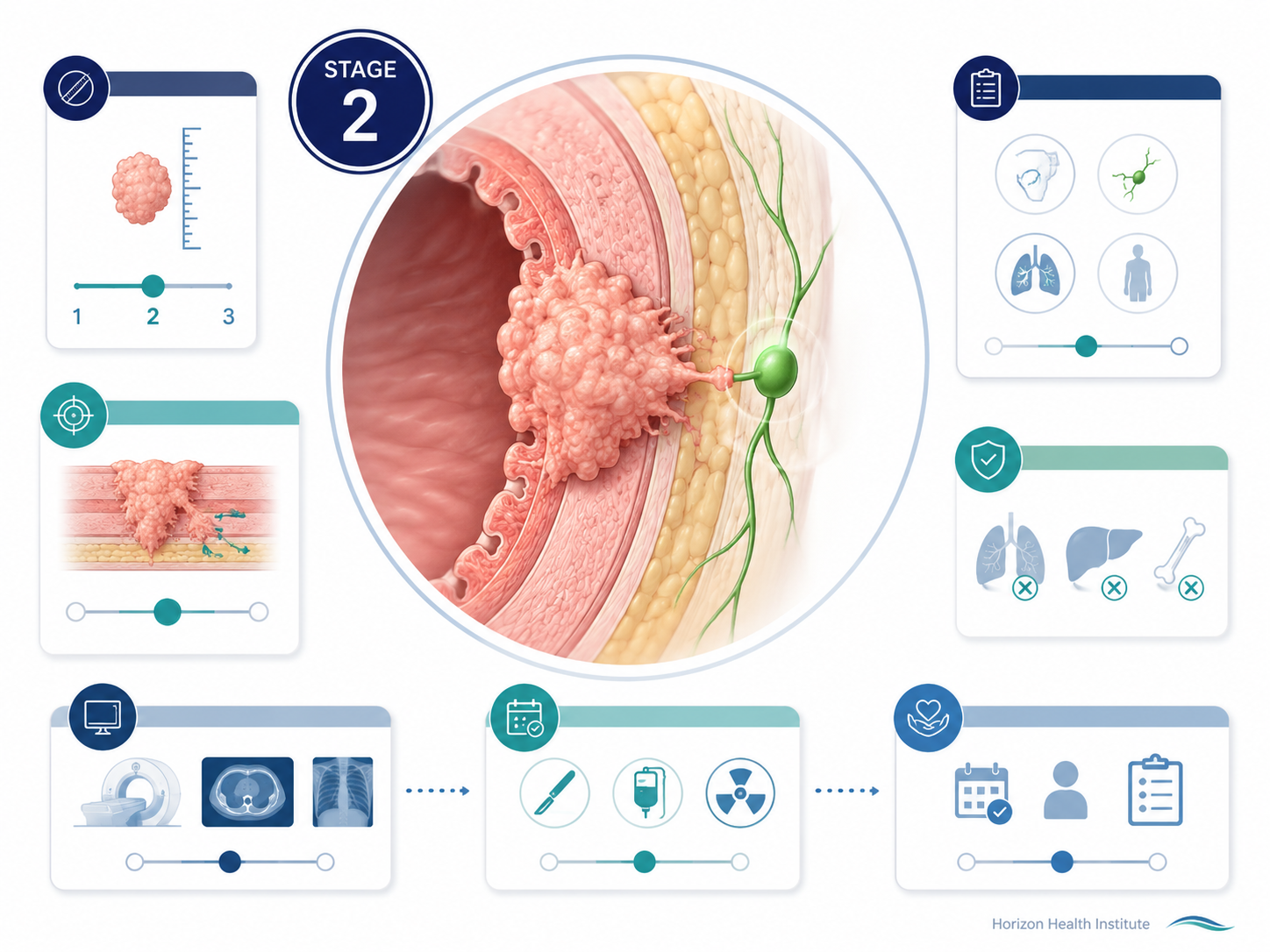
Stage 2 cancer still falls within the locoregional category — the cancer has not yet reached distant organs like the liver, lungs, or bones. What distinguishes it from stage 1:
- The tumor is larger — it has grown beyond the small, well-contained mass typical of stage 1
- In some cancer types, cancer has reached nearby lymph nodes — but only regional (local) nodes, not distant lymph nodes or organs
Using the TNM framework, stage 2 typically involves T2 or T3 (larger tumor), N0 to N1 (no or limited regional lymph node involvement), and M0 (no distant spread).
Stage 2 = tumor is larger than at stage 1, and/or limited regional lymph node involvement — but cancer has not spread to distant organs. Treatment is nearly always curative in intent.
This is not the same as saying cancer has “spread” in the way people fear. Stage 2 means the cancer is still regionally contained, still treatable, still beatable. To understand the full staging framework and what stage 1 looks like by comparison, our stage 1 cancer guide covers the complete staging system and survival rates.
Stage 2A vs Stage 2B — What’s the Difference?
Most cancers divide stage 2 into substages (2A, 2B — sometimes 2C) based on tumor size, depth of invasion, or the extent of lymph node involvement.
Breast Cancer
- Stage 2A: Tumor 2 cm or smaller with 1–3 positive axillary lymph nodes; OR tumor 2–5 cm with no lymph node involvement
- Stage 2B: Tumor 2–5 cm with 1–3 positive lymph nodes; OR tumor larger than 5 cm with no lymph nodes involved
For most patients, treatment approach is similar across 2A and 2B, though stage 2B is more likely to include neoadjuvant chemotherapy before surgery.
Lung Cancer (Non-Small Cell)
- Stage 2A: Tumor 4–5 cm confined to the lung, no lymph node involvement
- Stage 2B: Tumor larger than 5 cm (≤7 cm) with no nodes; OR tumor with spread to ipsilateral hilar lymph nodes (N1)
Colorectal Cancer
Unlike breast and lung, colorectal stage 2 has no lymph node involvement — that distinction belongs to stage 3:
- Stage 2A: Tumor grown into pericolorectal tissue (T3, N0)
- Stage 2B: Tumor penetrated through the visceral peritoneum (T4a, N0)
- Stage 2C: Tumor directly invaded adjacent organs (T4b, N0) — highest recurrence risk
Melanoma
Melanoma stage 2 substaging is based on tumor thickness and ulceration — no lymph node involvement (that becomes stage 3):
- Stage 2A: Tumor 1.0–2.0 mm with ulceration; or 2.0–4.0 mm without ulceration
- Stage 2B: Tumor 2.0–4.0 mm with ulceration; or >4.0 mm without ulceration
- Stage 2C: Tumor >4.0 mm with ulceration — now eligible for adjuvant pembrolizumab
Ask your oncologist specifically which substage you have and how it affects your treatment plan. Both 2A and 2B are treated with curative intent in most cancer types.
Stage 2 Cancer Survival Rates by Type
Before reading the table, a key reminder: relative survival rates are population statistics from hundreds of thousands of patients. They do not predict what happens to any individual. Your prognosis depends on tumor grade, molecular subtype, treatment center quality, your age, overall health, and other factors.
| Cancer Type | Stage 1 (5-Year) | Stage 2 (5-Year) | Stage 4 (5-Year) |
|---|---|---|---|
| Breast | ~99% | ~86–91% | ~28% |
| Lung (NSCLC) | ~68–92% | ~46–53% | ~7% |
| Colorectal | ~90% | ~72–83% | ~14% |
| Prostate | ~100% | ~100% | ~32% |
| Melanoma | ~98–99% | ~65–82% | ~30% |
| Ovarian | ~92% | ~75% | ~31% |
| Bladder | ~88% | ~46–63% | ~8% |
| Cervical | ~80–93% | ~58–69% | ~17% |
| Stomach | ~75% | ~46% | ~6% |
| Thyroid | ~100% | ~100% | ~55% |
Source: NCI SEER Program 2023; American Cancer Society Cancer Statistics 2024
Breast and prostate cancer remain near 100% at stage 2 — reflecting well-established, effective treatment protocols. Lung cancer shows the steepest drop between stage 1 and stage 2, underscoring the importance of early detection via low-dose CT screening. Across every type, the gap between stage 2 and stage 4 survival is substantial.
Factors that influence your individual prognosis at stage 2:
- Tumor grade: High-grade (poorly differentiated) tumors carry higher recurrence risk
- Molecular subtype: Triple-negative breast cancer at stage 2 has higher recurrence risk than HR+ HER2- types
- Number of lymph nodes involved: One positive node vs three positive nodes changes risk stratification
- Response to neoadjuvant therapy: Achieving pathologic complete response (pCR) is a strong favorable sign
- Surgical margins: Clear (negative) margins significantly improve outcomes
Is Stage 2 Cancer Serious?
Yes — and you deserve a straight answer.
Stage 2 is more serious than stage 1. The tumor is larger. In some cancer types, it has begun to involve lymph nodes. The recurrence risk is higher, and treatment is typically more intensive. Feeling more anxious at a stage 2 diagnosis than at stage 1 is completely valid, even when the survival numbers still look strong.
But “serious” is not the same as “unlikely to survive.” What stage 2 is not:
- It is not metastatic cancer — it has not spread to distant organs
- It is not stage 4 — “advanced cancer” in the news typically refers to stage 4 disease
- For breast cancer, prostate cancer, and thyroid cancer, stage 2 survival rates remain near 100%
If you want to understand what it looks like when cancer does reach distant sites and how medicine approaches that stage, our metastatic cancer guide covers exactly that.
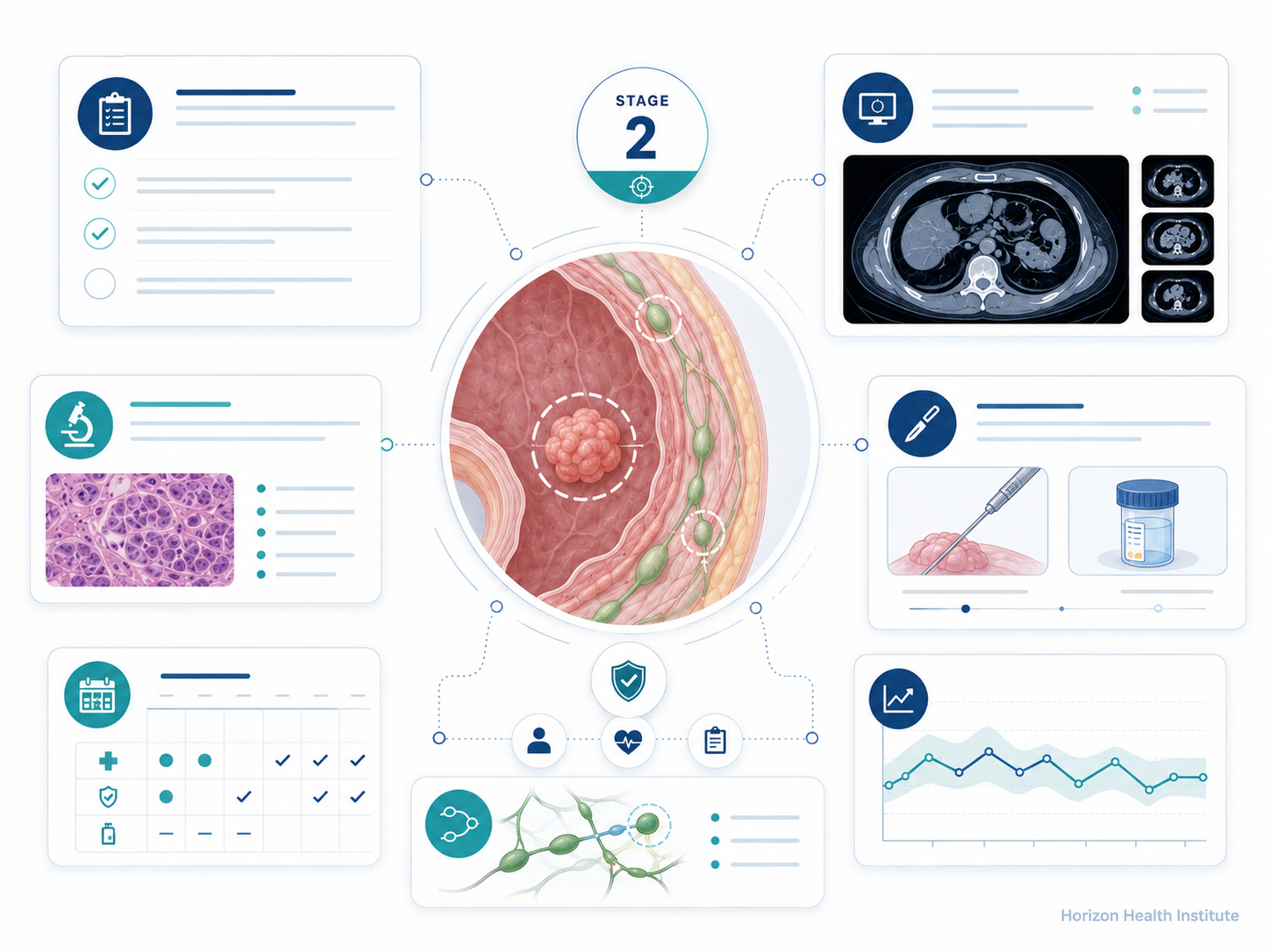
How Stage 2 Cancer Is Diagnosed
The diagnostic process for stage 2 follows the same sequence as stage 1 — detection, imaging, biopsy, lymph node assessment — but with some additional steps reflecting the higher stage.
More Comprehensive Lymph Node Evaluation
At stage 2, lymph node assessment becomes more thorough. While stage 1 often uses a sentinel lymph node biopsy (checking just the first one or two nodes), stage 2 may require a more extensive lymph node dissection. In breast cancer, discovering 1–3 positive lymph nodes at surgery is what moves a patient from stage 1 to stage 2 — and this isn’t always confirmed until pathology comes back after surgery.
PET Scan More Commonly Used
To definitively rule out distant spread (M0), a PET scan is more routinely ordered at stage 2 than at stage 1. This full-body scan detects metabolically active cancer cells and can identify hidden (occult) metastases that wouldn’t appear on a standard CT scan.
Biomarker and Molecular Testing
At stage 2, molecular testing becomes more clinically important because it directly drives systemic therapy decisions:
- ER/PR and HER2 status (breast cancer) — determines hormone therapy and HER2-targeted therapy eligibility
- EGFR, ALK, ROS1 (lung cancer) — guides targeted therapy decisions after surgery
- Microsatellite instability (MSI-H) (colorectal) — may indicate benefit from immunotherapy
- BRAF V600E (melanoma) — opens door to BRAF/MEK inhibitor therapy
- Oncotype DX score (HR+/HER2- breast) — helps predict whether chemotherapy will provide meaningful benefit
A cancer diagnosed as stage 1 on imaging may be upstaged to stage 2 after surgery, when pathologists examine the full tumor and lymph nodes. This happens when imaging misses small lymph node deposits. Your treatment plan may be adjusted based on the pathologic (final) stage.
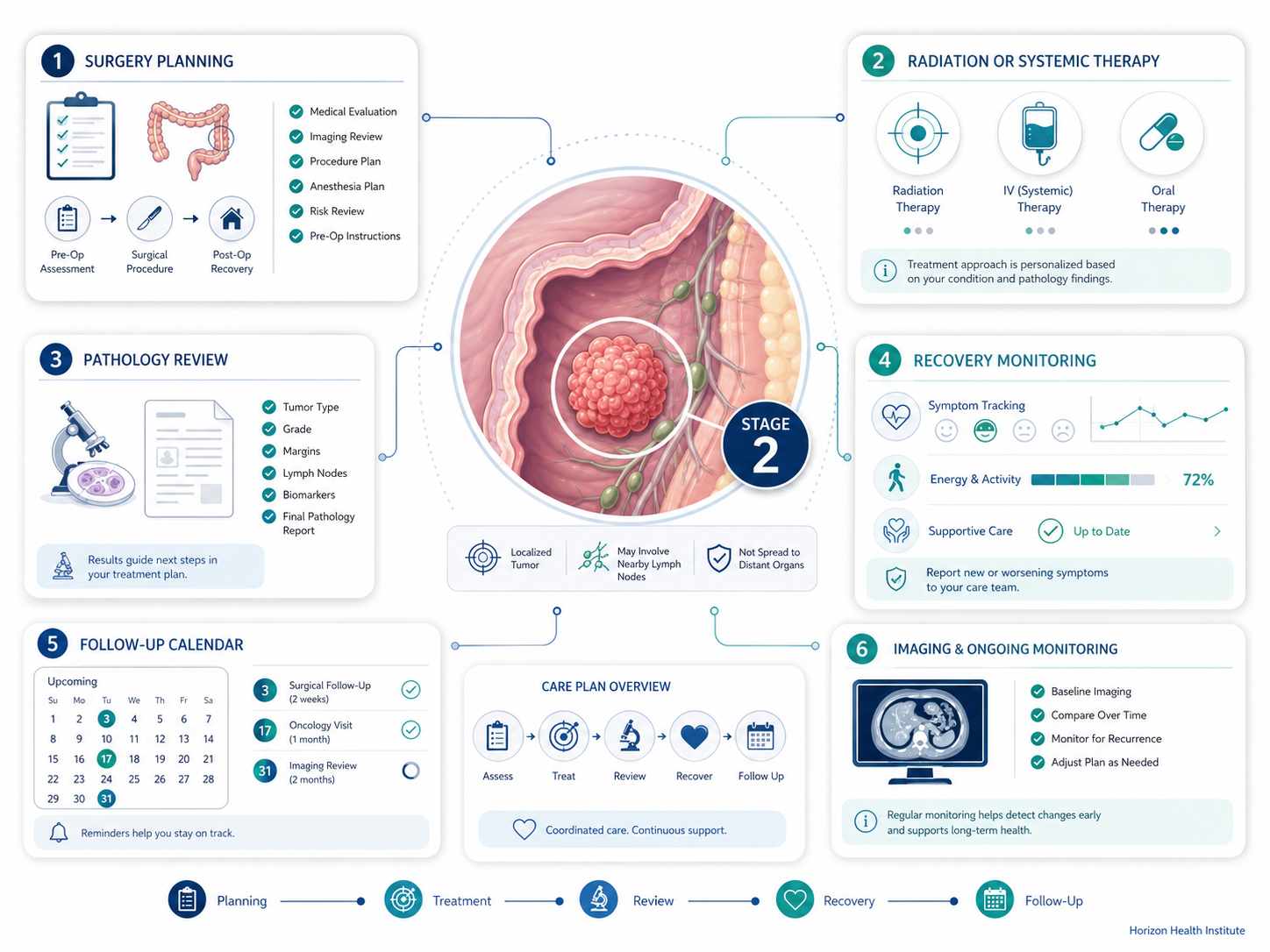
Stage 2 Cancer Treatment Options
Stage 2 treatment is almost always multimodal — meaning you’ll receive more than one type of treatment. The goal remains curative in nearly all cases, but the approach is more intensive than stage 1.
Surgery
Surgery remains the cornerstone for most stage 2 solid tumors. At stage 2, surgery may be more extensive: wider excision margins, more lymph nodes removed for pathologic assessment, and in some cases mastectomy rather than lumpectomy (large stage 2B breast tumors). Modern robotic and laparoscopic techniques remain available where tumor location permits.
Neoadjuvant Therapy (Treatment Before Surgery)
One of the key differences at stage 2 is the option — and sometimes recommendation — of neoadjuvant therapy: giving chemotherapy, targeted therapy, or immunotherapy before surgery. Benefits include:
- Shrinking the tumor to enable less extensive surgery or improve resection
- Testing cancer’s response to treatment while it’s still measurable
- Achieving a pathologic complete response (pCR) — no cancer cells found in the removed tissue — a strong favorable prognostic marker
Neoadjuvant therapy is standard for locally advanced breast cancer (stage 2B+) and increasingly used for stage 2 rectal and some lung cancers.
Adjuvant Chemotherapy
Given after surgery to eliminate residual microscopic cancer cells. At stage 2:
- Standard for NSCLC stage 2 after surgery
- Recommended for high-risk colorectal stage 2 (T4, perforation, poor differentiation, MSI-stable)
- Common for triple-negative and HER2+ breast cancer at stage 2
- Not routinely given for HR+/HER2- breast cancer at stage 2 with low Oncotype DX score
Radiation Therapy
Adjuvant radiation is widely used at stage 2: standard after lumpectomy for breast cancer; neoadjuvant chemoradiation for rectal cancer; external beam + brachytherapy for cervical cancer; primary treatment or post-surgery option for prostate cancer.
Immunotherapy
- Melanoma stage 2C: Pembrolizumab (Keytruda) for 1 year after surgery (KEYNOTE-716 trial) significantly reduces recurrence risk
- Triple-negative breast cancer stage 2: Pembrolizumab included in neoadjuvant regimens (KEYNOTE-522)
- High MSI-H colorectal: Immune checkpoint inhibitors may be considered
Hormone and Targeted Therapy
- HR+ breast cancer: Tamoxifen or aromatase inhibitors for 5–10 years post-surgery
- HER2+ breast cancer: Trastuzumab (Herceptin) + pertuzumab (Perjeta) significantly improve stage 2 outcomes
- Prostate cancer stage 2: Androgen deprivation therapy (ADT) combined with radiation for intermediate/high-risk cases
- EGFR+ NSCLC stage 2: Osimertinib (Tagrisso) for up to 3 years after surgery (ADAURA trial)
Can Stage 2 Cancer Be Cured?
For most stage 2 cancers, yes — treatment is given with curative intent. The goal is complete elimination of cancer cells, not just slowing the disease.
Stage 2 has a meaningfully higher recurrence risk than stage 1. After completing treatment, follow-up surveillance is scheduled at more frequent intervals — typically every 3–4 months for the first two years, then every 6 months, then annually. What to know:
- Recurrence means cancer has returned after remission — not that treatment failed outright
- Most recurrences after stage 2 are caught during scheduled surveillance before symptoms appear
- Treatments for recurrent cancer have improved substantially with immunotherapy and targeted agents
You’ll hear terms like “no evidence of disease” (NED) or “complete response” rather than “cured” — oncologists typically reserve the word “cure” until 5–10 years have passed without recurrence.
Questions to Ask After a Stage 2 Diagnosis
- What is my exact substage (2A, 2B, 2C), and what does it mean for my specific treatment?
- Is neoadjuvant therapy (treatment before surgery) recommended — and why or why not?
- Will I need chemotherapy? What regimen, and for how long?
- Should I have molecular or biomarker testing (Oncotype DX, EGFR, HER2, MSI)?
- Am I eligible for an immunotherapy clinical trial?
- What are the short-term and long-term side effects of the recommended treatment?
- How will we know if treatment is working?
- Should I consider a second opinion at a comprehensive cancer center?
- What follow-up schedule will I need after completing treatment?
- Are there lifestyle changes — diet, exercise — that could improve my outcome?
Frequently Asked Questions
Sources
- National Cancer Institute — Cancer Staging. cancer.gov
- NCI SEER Program — Cancer Stat Facts: 5-Year Relative Survival Rates by Stage (2023). seer.cancer.gov
- American Cancer Society — Cancer Facts & Figures 2024. cancer.org
- Mayo Clinic — Cancer staging. mayoclinic.org
- ASCO Cancer.Net — Stages of Cancer. cancer.net
- AJCC Cancer Staging Manual, 8th Edition. springer.com