Hearing “stage 4” can feel like the ground disappearing beneath you. For patients and families, those two words often carry the weight of finality — a door closing.
But the science tells a different story. In 2011, the five-year survival rate for stage 4 melanoma was around 10%. Today, with immunotherapy, it’s nearly 49%. Stage 4 cancer is still serious — but it is not always the end, and for many people, it’s the beginning of a fight they can genuinely win.
This guide explains what stage 4 really means, how survival rates vary dramatically by cancer type, what modern treatments offer in 2024 and beyond, and how to navigate life after this diagnosis.
What Does Stage 4 Cancer Mean?
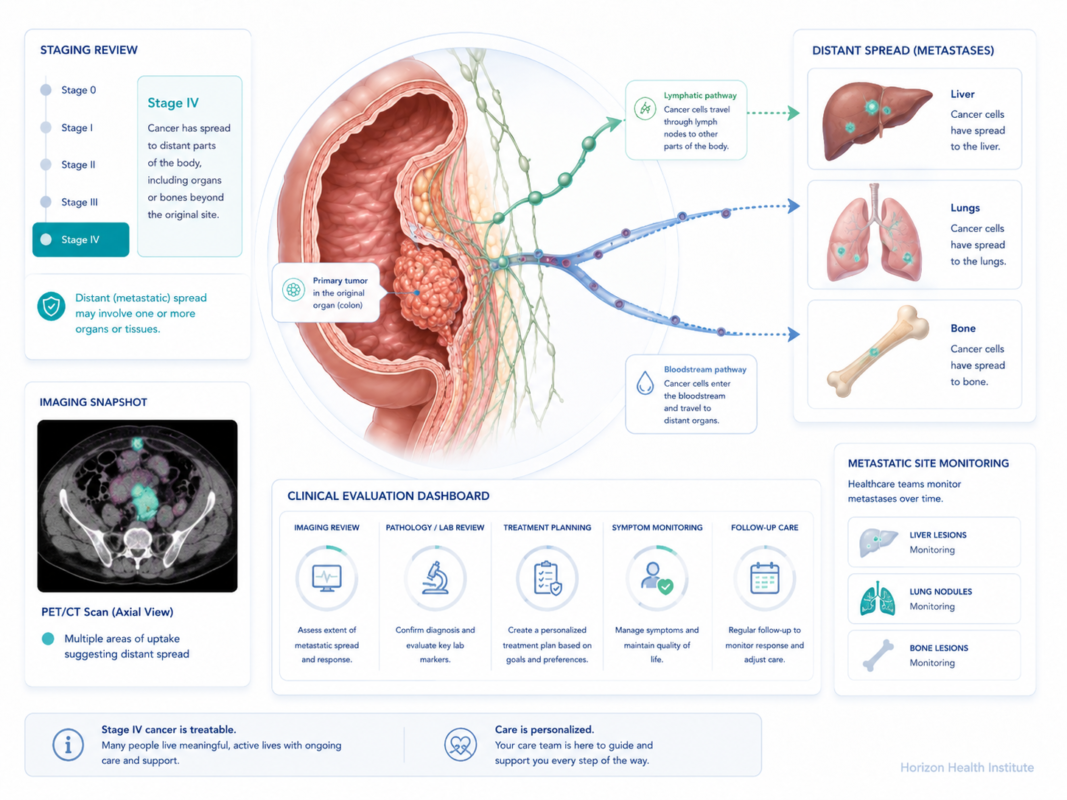
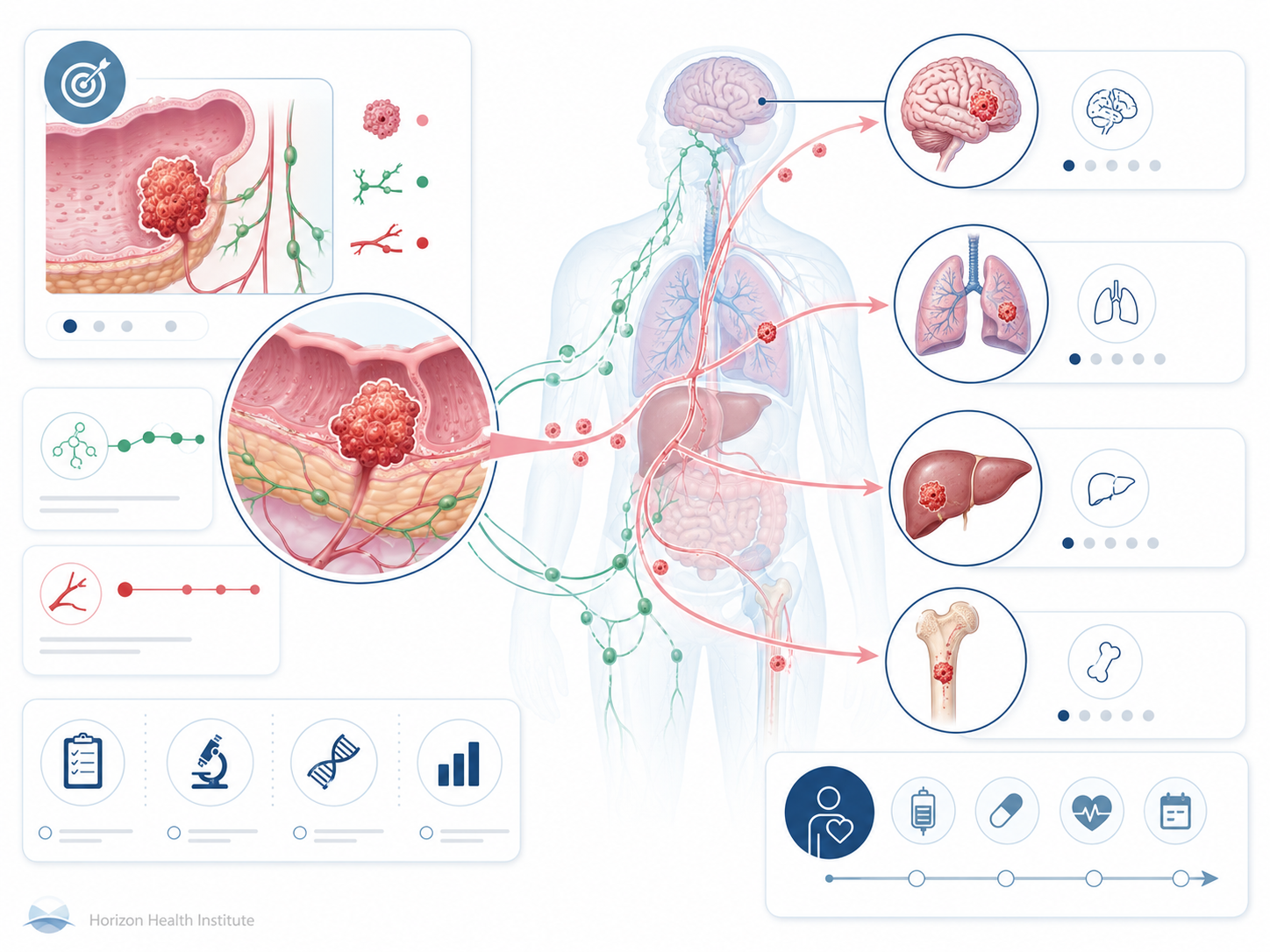
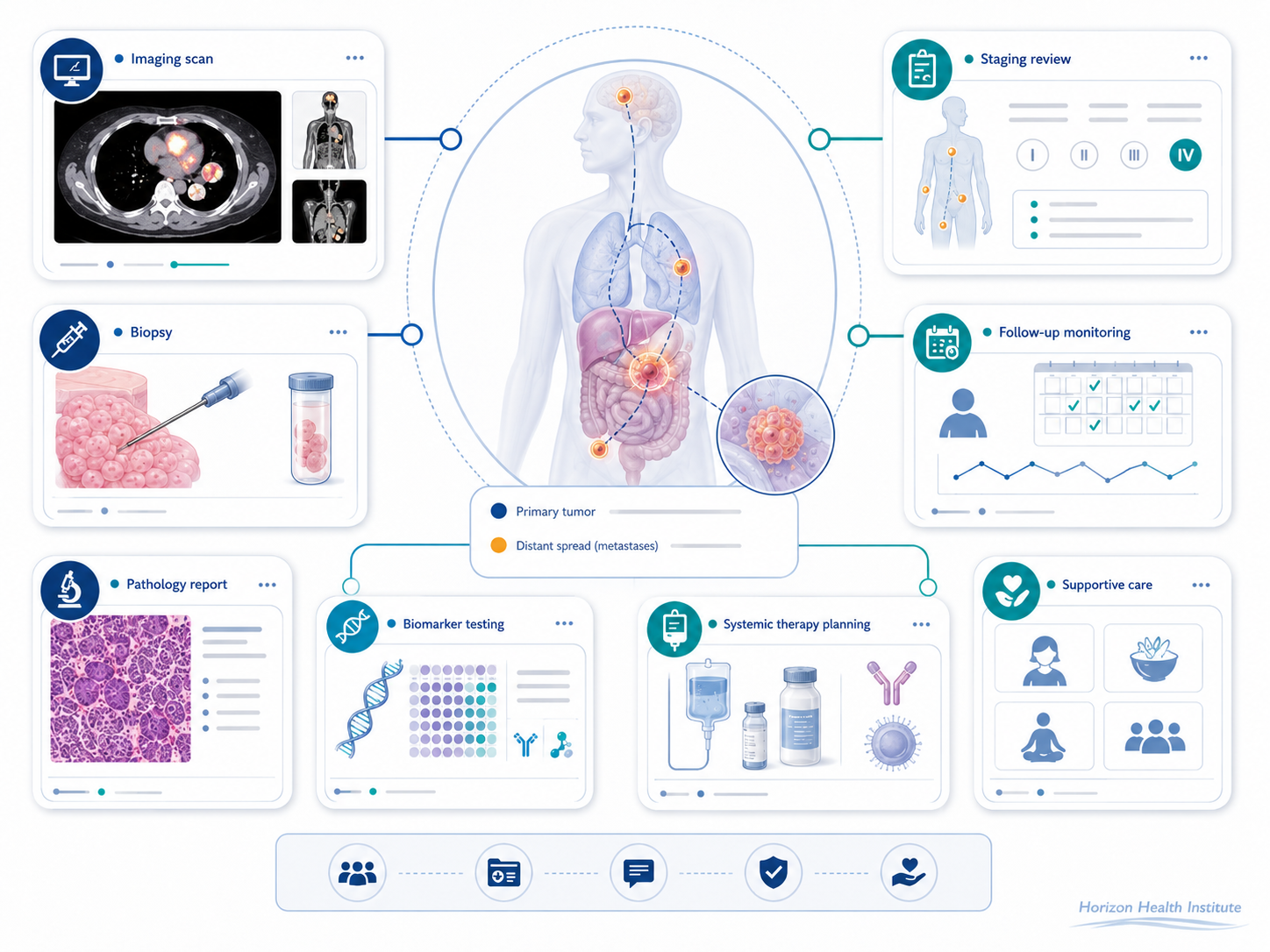
Cancer staging follows the TNM system — Tumor, Nodes, Metastasis. Stage 4 always means M1: distant metastasis has been confirmed. Cancer cells have broken away from the original tumor, entered the bloodstream or lymphatic system, and established new growths in other parts of the body.
This is different from stage 3, where cancer may be locally advanced but hasn’t jumped to distant organs yet. In stage 3 cancer, the goal is often still curative. Stage 4 shifts that goal for most cancers — though not all.
Common Sites Where Cancer Spreads
| Metastatic Site | Common Primary Cancers | Key Symptom |
|---|---|---|
| Bone | Breast, prostate, lung, kidney | Deep aching pain; fractures |
| Liver | Colorectal, breast, lung, pancreas | Jaundice, right-sided abdominal pain |
| Lung | Breast, colorectal, kidney, sarcoma | Shortness of breath, persistent cough |
| Brain | Lung, breast, melanoma, kidney | Headaches, seizures, confusion |
| Adrenal glands | Lung, kidney, melanoma | Often asymptomatic (found on scan) |
Stage 4 vs Metastatic Cancer — Are They the Same?
Yes. Oncologists prefer the term “metastatic” because it describes what’s actually happening biologically. You’ll also hear “advanced cancer” used interchangeably. All three terms describe the same stage of disease — cancer that has spread beyond the local region to distant sites.
For a deeper look at how metastatic disease is classified, treated, and managed, see our complete metastatic cancer guide.
Stage 4 Cancer Survival Rates by Type
Before reading these numbers, understand one important thing: survival rates are calculated from historical data — often 5–10 years old. They reflect how patients were treated in the past, not what today’s therapies can achieve. And critically, they are population averages. They cannot predict what happens to you specifically.
5-year survival (stage 4)
5-year survival (stage 4)
5-year survival (stage 4)
5-Year Relative Survival Rates at Stage 4 (SEER 2023)
| Cancer Type | 5-Year Survival | Key Driver of Prognosis |
|---|---|---|
| Thyroid (distant) | 57% | Slow-growing; RAI-responsive |
| Prostate (distant) | 34% | Hormone therapy extends years |
| Melanoma (distant) | 35% | Immunotherapy has transformed outcomes |
| Ovarian (distant) | 31% | PARP inhibitors significant advance |
| Breast (distant) | 29% | Targeted therapy (HER2+) major gains |
| Colorectal (distant) | 15% | VEGF inhibitors + chemotherapy |
| Lung NSCLC (distant) | 8–10% | Targeted therapy + immunotherapy |
| Bladder (distant) | 8% | Checkpoint inhibitors improving |
| Liver (distant) | 3% | Very poor prognosis |
| Pancreatic (distant) | 3% | Minimal improvement despite new drugs |
Which Stage 4 Cancers Have the Best Outcomes?
Thyroid cancer at stage 4 — particularly differentiated thyroid cancer — is often described as a chronic, manageable condition. Many patients live decades with stable distant metastases, particularly when tumors respond to radioactive iodine (RAI) therapy. Stage 4 testicular cancer similarly has a five-year survival of approximately 73%.
Why Have Outcomes Improved So Dramatically?
Targeted therapy works by attacking specific molecular drivers of cancer growth rather than just killing all fast-dividing cells. A patient with EGFR-mutated NSCLC treated with osimertinib (Tagrisso) has a median progression-free survival of 18.9 months — nearly three times longer than older chemotherapy.
Immunotherapy removes the brakes that tumors place on the immune system. In the CheckMate 067 trial, patients with metastatic melanoma receiving nivolumab plus ipilimumab had a five-year overall survival of 52% — a figure once unthinkable.
Symptoms of Stage 4 Cancer
Stage 4 symptoms depend on both the primary cancer site and where it has spread. Some patients feel relatively well at diagnosis; others are seriously ill. Here’s what to know.
Universal Symptoms
- Extreme fatigue — the most universal symptom; caused by cytokine release, metabolic competition, and systemic inflammation
- Unexplained weight loss — losing more than 10 pounds without trying; severe cases develop cachexia, a metabolic syndrome affecting up to 80% of patients with advanced cancer
- Chronic pain — bone metastases are the most common cause of severe pain; neuropathic pain from nerve compression also occurs
- Breathlessness — pleural effusion, lung metastases, or anemia can all restrict breathing
- Jaundice — yellowing of skin and eyes signals liver involvement or blocked bile ducts
- Loss of appetite — closely linked to cachexia; food aversion and early satiety are common
Symptoms by Metastatic Site
Bone metastases: Deep, aching pain often worse at night; fractures with minor trauma (pathologic fractures); hypercalcemia causing confusion and nausea.
Liver metastases: Right upper quadrant abdominal pain, nausea, jaundice, itching, fatigue from reduced liver function.
Brain metastases: Morning headaches worse when lying down, seizures, personality or memory changes, weakness on one side, vision changes.
Lung metastases: Progressive shortness of breath, persistent cough, chest pain, occasionally coughing blood.
Warning Signs: Call Your Doctor Right Away
- ⚠ Sudden, severe headache unlike any before
- ⚠ New seizure or loss of consciousness
- ⚠ Sudden confusion or disorientation
- ⚠ Bone fracture from minimal or no trauma
- ⚠ Severe, sudden back pain (possible spinal cord compression)
- ⚠ Difficulty breathing at rest
- ⚠ Inability to eat or drink for more than 24 hours
- ⚠ Yellowing of skin or eyes that appears suddenly
Treatment Options for Stage 4 Cancer
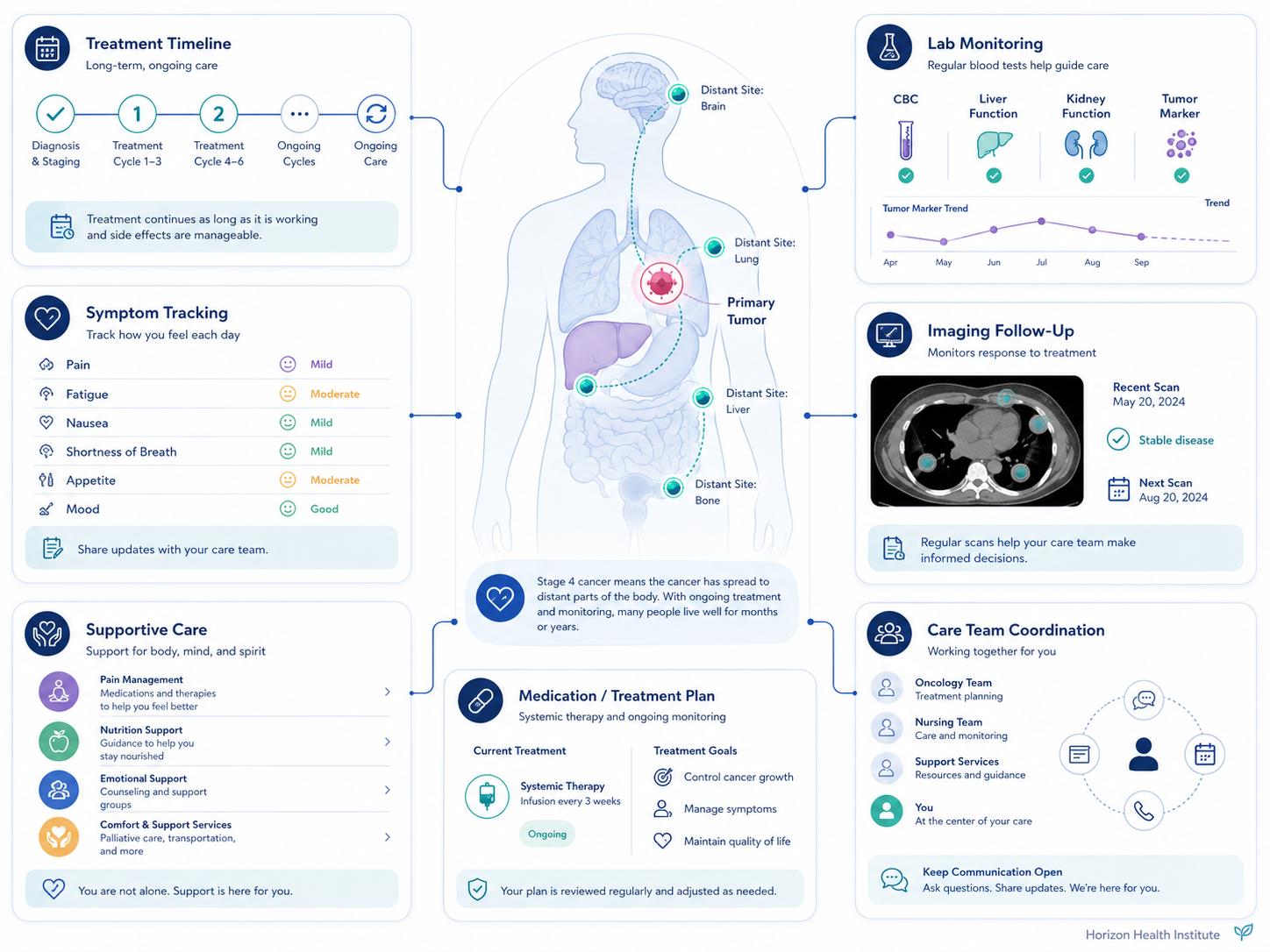
The goal of treatment shifts at stage 4. For some cancers, cure remains possible — particularly with targeted therapy or immunotherapy. For most, the goals become disease control, symptom management, and extending high-quality life. Treatment for stage 3 cancer and stage 4 often overlaps, but stage 4 adds a stronger emphasis on systemic therapies and a broader role for palliative support.
Chemotherapy
Traditional chemotherapy attacks all rapidly dividing cells throughout the body. At stage 4, it’s used when cancer lacks targetable mutations, has spread too widely for localized approaches, or requires fast-acting tumor reduction. Common regimens: FOLFOX or FOLFIRI (colorectal), carboplatin + pemetrexed (lung), AC-T (breast), FOLFIRINOX (pancreatic). Chemotherapy is often combined with targeted agents or immunotherapy to increase response rates.
Targeted Therapy
Targeted therapy requires knowing the cancer’s molecular profile — which means comprehensive genomic profiling before starting treatment is essential.
How Do I Know If I’m a Candidate for Targeted Therapy?
Ask your oncologist for comprehensive genomic profiling (e.g., FoundationOne CDx) on your tumor biopsy. This test screens for hundreds of mutations simultaneously and can identify targetable drivers your oncologist may otherwise miss.
Key targeted therapies at stage 4:
- Osimertinib (Tagrisso) — EGFR-mutated NSCLC; 18.9-month median progression-free survival
- Alectinib (Alecensa) — ALK+ NSCLC; 34.8-month median PFS (ALEX trial)
- Trastuzumab + pertuzumab — HER2+ metastatic breast cancer
- Olaparib (Lynparza) — BRCA1/2-mutated ovarian or breast cancer
- Dabrafenib + trametinib — BRAF V600E-mutated melanoma
- Palbociclib (Ibrance) — HR+/HER2- metastatic breast cancer with endocrine therapy
Immunotherapy
Immune checkpoint inhibitors are the most transformative advance in stage 4 oncology in the past decade. They block proteins (PD-1, PD-L1, CTLA-4) that tumors exploit to hide from the immune system.
Key drugs: pembrolizumab (Keytruda), nivolumab (Opdivo), ipilimumab (Yervoy), atezolizumab (Tecentriq)
| Trial | Cancer | Key Result |
|---|---|---|
| KEYNOTE-024 | NSCLC (PD-L1 ≥50%) | 5-yr OS: 31% (pembro) vs 16% (chemo) |
| CheckMate 067 | Metastatic melanoma | 5-yr OS: 52% (nivo + ipi) |
| KEYNOTE-158 | MSI-H/dMMR tumors (any type) | Pan-tumor FDA approval; ORR 36% |
Radiation Therapy
At stage 4, radiation shifts from curative to strategic:
- Palliative radiation: Single or short-course treatment to relieve bone pain. A single 8 Gy fraction provides relief in ~60–70% of patients.
- SBRT/SRS: High-dose, precisely targeted radiation to specific metastatic sites — brain, spine, or isolated organ mets.
- WBRT: Used for multiple brain metastases; increasingly replaced by SRS + immunotherapy approaches due to cognitive decline risk.
Oligometastatic Disease — A Separate Category
When cancer has spread to only one to five isolated, accessible sites, some patients qualify for aggressive, curative-intent treatment. The SABR-COMET trial showed SBRT to all oligometastatic sites produced five-year OS of 42% vs 17% in standard care — a significant paradigm shift showing stage 4 doesn’t always mean giving up on cure.
Palliative Care vs Hospice — Understanding the Difference
No term in oncology is more misunderstood — or more feared — than palliative care. Patients hear “palliative” and assume they’re being told to give up. This confusion costs lives.
Palliative care begins at diagnosis. It runs alongside chemotherapy, targeted therapy, radiation, and immunotherapy. Its focus: managing pain, nausea, fatigue, anxiety, and any other symptom that reduces quality of life.
A landmark 2010 study in the New England Journal of Medicine (Temel et al.) demonstrated this powerfully. Patients with stage 4 NSCLC who received early palliative care alongside standard treatment had better quality of life, less depression (16% vs 38%), and longer median overall survival: 11.6 months vs 8.9 months.
Important Distinction: Palliative care is specialized symptom management available from the day of diagnosis, alongside any active treatment. Hospice is end-of-life care provided when life expectancy is estimated at six months or less and the patient chooses to focus on comfort rather than disease-directed treatment. They are not the same thing.
Hospice care provides intensive comfort-focused support in the final phase of life — at home, in hospice facilities, or in hospitals. It covers pain medication, nursing visits, social work, and spiritual support. Patients on hospice sometimes outlive their six-month prognosis. Choosing hospice is not giving up — it’s choosing how to live on your own terms.
Living With Stage 4 Cancer — Practical Guidance
Mental health: Anxiety and depression affect 40–50% of patients with advanced cancer. These are clinical conditions requiring treatment — ask your oncology team for a referral to an oncology social worker or psychologist.
Exercise and nutrition: ASCO guidelines recommend 150 minutes per week of moderate aerobic activity for cancer patients able to exercise. Multiple studies show exercise reduces cancer-related fatigue, improves mood, and may extend survival. Focus on adequate protein and caloric intake — cachexia prevention starts early.
Clinical trials: Don’t save trials for “when nothing else works.” Many of the most promising drugs are only available in trials. ClinicalTrials.gov lists all current trials by cancer type, stage, mutation status, and location.
Financial assistance: Targeted therapies and immunotherapy can cost $10,000–$20,000 per month. Resources include manufacturer co-pay cards, NeedyMeds.org, and Triage Cancer for insurance navigation.
Second opinions: ASCO encourages second opinions for all cancer diagnoses, especially at stage 4. NCCN-designated comprehensive cancer centers have depth in rare presentations, novel therapies, and trial access.
Frequently Asked Questions
References
- National Cancer Institute. SEER Cancer Statistics. Surveillance, Epidemiology, and End Results Program. 2017–2023. seer.cancer.gov
- Temel JS, et al. Early Palliative Care for Patients with Metastatic NSCLC. New England Journal of Medicine. 2010;363(8):733–742.
- Reck M, et al. Pembrolizumab versus Chemotherapy for PD-L1–Positive NSCLC (KEYNOTE-024). New England Journal of Medicine. 2016;375(19):1823–1833.
- Larkin J, et al. Five-Year Survival with Nivolumab + Ipilimumab in Advanced Melanoma (CheckMate 067). New England Journal of Medicine. 2019;381(16):1535–1546.
- Palma DA, et al. Stereotactic Ablative Radiotherapy for Oligometastatic Cancers (SABR-COMET). The Lancet. 2019;393(10185):2051–2058.
- American Cancer Society. Cancer Statistics 2024. Atlanta, GA: ACS; 2024.
- Peters S, et al. Alectinib versus Crizotinib in ALK+ NSCLC (ALEX trial). New England Journal of Medicine. 2017;377(9):829–838.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Version 2024. nccn.org