Of all the cancer stages, stage 3 is perhaps the one that triggers the deepest fear. Not because the numbers are necessarily the worst — stage 4 carries harder statistics — but because “stage 3” sounds close to the edge. Patients who receive this diagnosis often ask: “Is this the bad one?”
Here is an honest answer: stage 3 cancer is serious. It requires aggressive treatment. But it is not stage 4. It has not spread to distant organs. And for most cancer types, doctors still approach stage 3 with a plan aimed at cure — not just control.
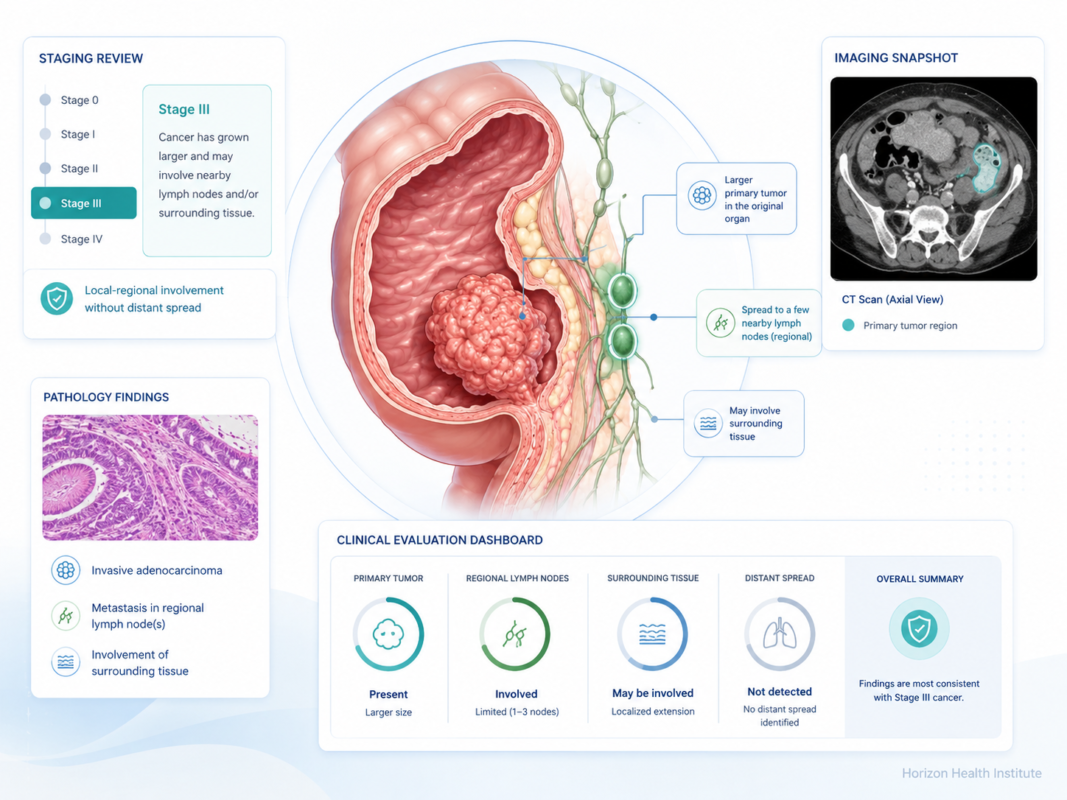
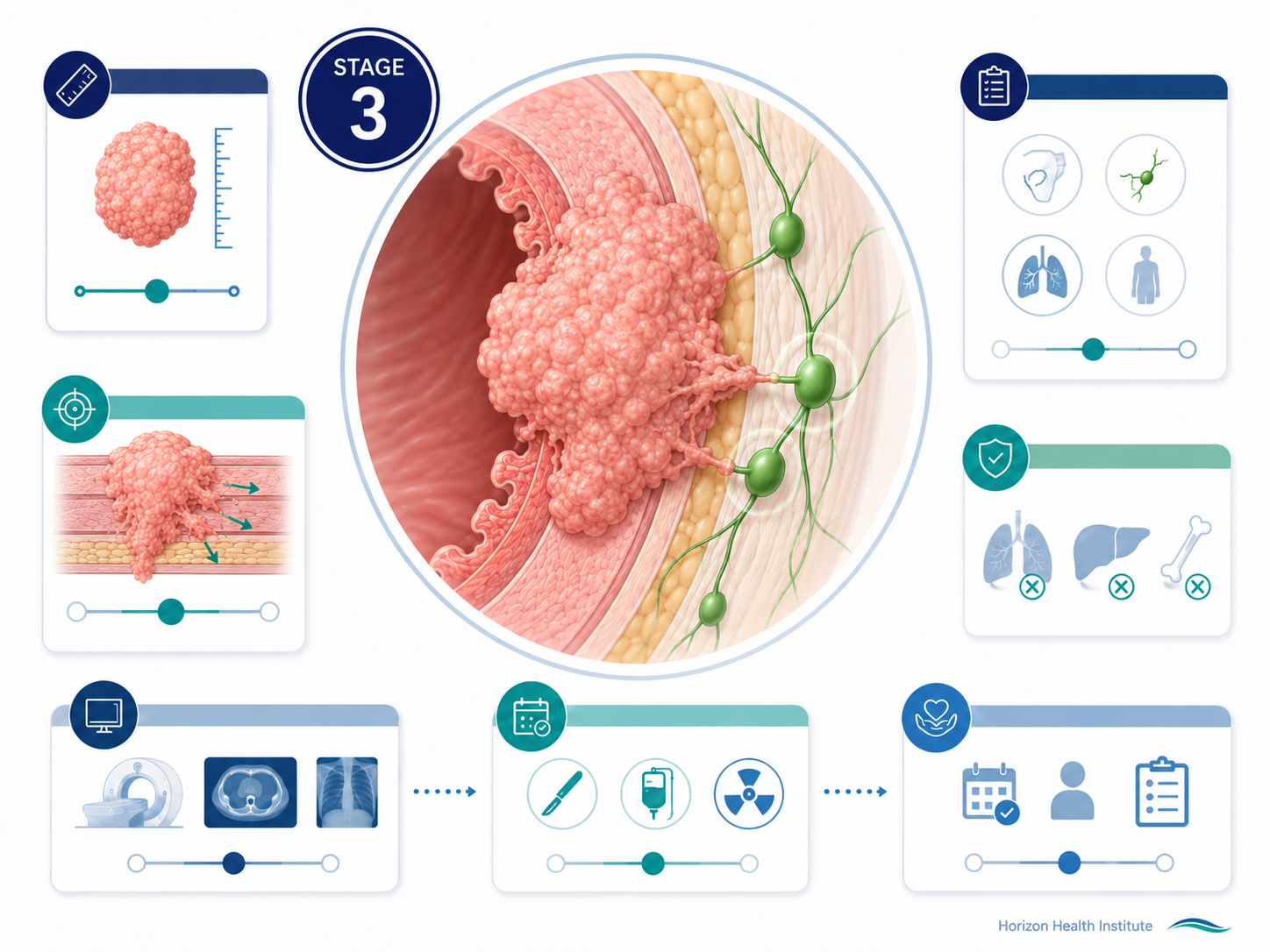
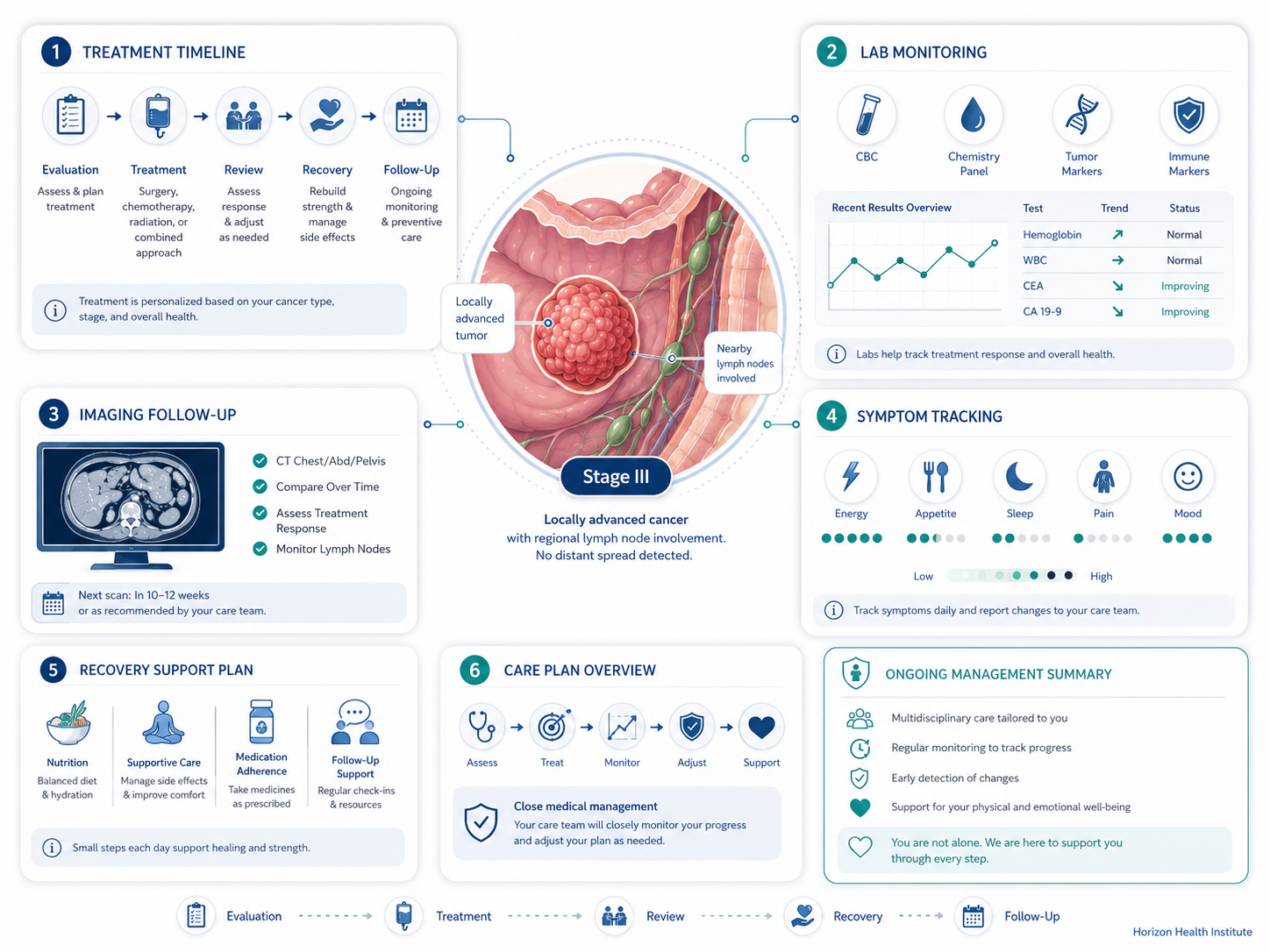
Stage 3 is called “locally advanced” cancer — the tumor has grown significantly and regional lymph nodes are involved, but cancer has not spread to distant organs (M0). Treatment is given with curative intent in the majority of cases.
What Does Stage 3 Cancer Mean?
Oncologists use the term “locally advanced cancer” for stage 3 disease. It describes cancer that has grown significantly — larger tumor, more lymph node involvement — but has still not broken out of the regional area of the body. In the TNM system:
- T (Tumor): Large or invasive primary tumor (T3–T4)
- N (Node): More extensive regional lymph node spread (N2–N3) than at stage 2
- M (Metastasis): M0 — no distant metastasis confirmed
Stage 3 = larger tumor and/or extensive regional lymph node spread — but no distant metastasis (M0). The liver is clear. The lungs are clear. The bones are clear. It is called “locally advanced” and treated with curative intent in the majority of cases.
Stage 3 is the most aggressive form of disease that has not yet crossed into distant spread. To understand what earlier stages look like and how they compare, our stage 2 cancer guide covers locoregional disease and how treatment at that level differs.
Stage 3A, 3B, and 3C — How Substages Differ
Breast Cancer
- Stage 3A: Tumor of any size with 4–9 positive axillary lymph nodes; or tumor >5 cm with 1–3 positive nodes or positive internal mammary nodes
- Stage 3B: Tumor grown into chest wall or skin (including inflammatory breast cancer); up to 9 positive nodes
- Stage 3C: 10 or more positive axillary lymph nodes; or spread to nodes above or below the clavicle; or involvement of both axillary and internal mammary nodes
Lung Cancer (Non-Small Cell)
- Stage 3A: Spread to ipsilateral mediastinal lymph nodes (N2). Some 3A cases are surgically resectable.
- Stage 3B: N3 (contralateral or supraclavicular nodes) or larger T with N2. Generally unresectable.
- Stage 3C: T3–T4 with N3. Unresectable — treated with chemoradiation + durvalumab consolidation.
Colorectal Cancer
In colorectal cancer, stage 3 is defined by lymph node involvement — the key distinction from stage 2 (which has no positive nodes):
- Stage 3A: T1–T2 tumor with 1–3 positive nodes (N1) — best-prognosis stage 3 (~89% 5-year survival)
- Stage 3B: T3–T4a with 1–3 nodes, or T2–T3 with 4–6 nodes (N2a)
- Stage 3C: T4a with N2; or T3–T4a with 7+ positive nodes — highest recurrence risk at stage 3
Melanoma
Melanoma stage 3 is defined by spread to regional lymph nodes or in-transit metastases, without distant spread:
- Stage 3A: Micrometastases in nodes, no ulceration — best-prognosis stage 3 melanoma (~78% 5-year survival)
- Stage 3B/3C: Larger or more numerous nodal deposits, ulcerated primary tumors
- Stage 3D: In-transit disease with 4+ positive nodes — highest-risk stage 3 melanoma
Ask your oncologist which substage applies to you and how it determines whether surgery, chemoradiation, or both are recommended. The substage distinction is critical at stage 3.
Stage 3 Cancer Survival Rates by Type
Survival rates at stage 3 show more variation than at earlier stages — some cancers remain highly treatable; others show significant drops from stage 2. These are population-level statistics from NCI SEER data — not predictions for individuals. Your prognosis is shaped by substage, tumor biology, treatment quality, molecular profile, and your overall health.
| Cancer Type | Stage 2 (5-Year) | Stage 3 (5-Year) | Stage 4 (5-Year) |
|---|---|---|---|
| Breast | ~86–91% | ~48–86% | ~28% |
| Lung (NSCLC) | ~46–53% | ~13–36% | ~7% |
| Colorectal | ~72–83% | ~42–89% | ~14% |
| Prostate | ~100% | ~100% | ~32% |
| Melanoma | ~65–82% | ~40–78% | ~30% |
| Ovarian | ~75% | ~39–59% | ~31% |
| Bladder | ~46–63% | ~36–38% | ~8% |
| Cervical | ~58–69% | ~32–57% | ~17% |
| Stomach | ~46% | ~20–26% | ~6% |
| Head & Neck | ~70–80% | ~50–65% | ~20–30% |
Source: NCI SEER Program 2023; American Cancer Society Cancer Statistics 2024
Two things stand out: the range within stage 3 is wide — colorectal 3A has ~89% survival while lung 3C has ~13%. And the gap to stage 4 remains meaningful — even for the hardest-to-treat cancers, stage 3 survival is substantially better than stage 4.
Factors that influence individual prognosis at stage 3:
- Substage (3A vs 3B vs 3C): Significant survival differences exist within stage 3 itself
- Resectability: Whether surgery is possible dramatically affects outcomes
- Response to neoadjuvant therapy: Achieving pathologic complete response (pCR) is a strong favorable prognostic marker
- Molecular features: PD-L1 expression, EGFR/ALK status, MSI-H, HER2 status affect treatment eligibility and outcomes
- Treatment center volume: High-volume comprehensive cancer centers show better outcomes for complex stage 3 cases
Resectable vs Unresectable Stage 3 — Why It Matters
At stage 1 and 2, most tumors can be surgically removed. At stage 3, this is no longer always true — and understanding this distinction is one of the most important concepts at this stage.
Resectable Stage 3
Surgery to remove the tumor is possible and part of the treatment plan:
- Some lung cancer 3A — single-node N2 disease may be resectable, especially after neoadjuvant chemotherapy
- Stage 3 breast cancer — neoadjuvant chemotherapy shrinks the tumor first, then surgery
- Stage 3 colorectal cancer — resection + lymph node removal, followed by adjuvant chemotherapy
- Stage 3 gastric cancer — perioperative FLOT chemotherapy + surgery
Unresectable Stage 3
The cancer cannot be surgically removed due to critical structure involvement:
- Lung 3B/3C — definitive concurrent chemoradiation + durvalumab consolidation (PACIFIC regimen)
- Stage 3 cervical cancer — primary chemoradiation (external beam + brachytherapy + cisplatin); surgery not standard
- Head and neck stage 3 — concurrent chemoradiation; surgery reserved for residual disease
Chemoradiation can sometimes convert an initially unresectable tumor to a resectable one. If treatment shrinks the tumor sufficiently, surgery may become possible — a strategy called downstaging or conversion therapy. This happens in rectal, head and neck, and some lung cancer 3B cases.
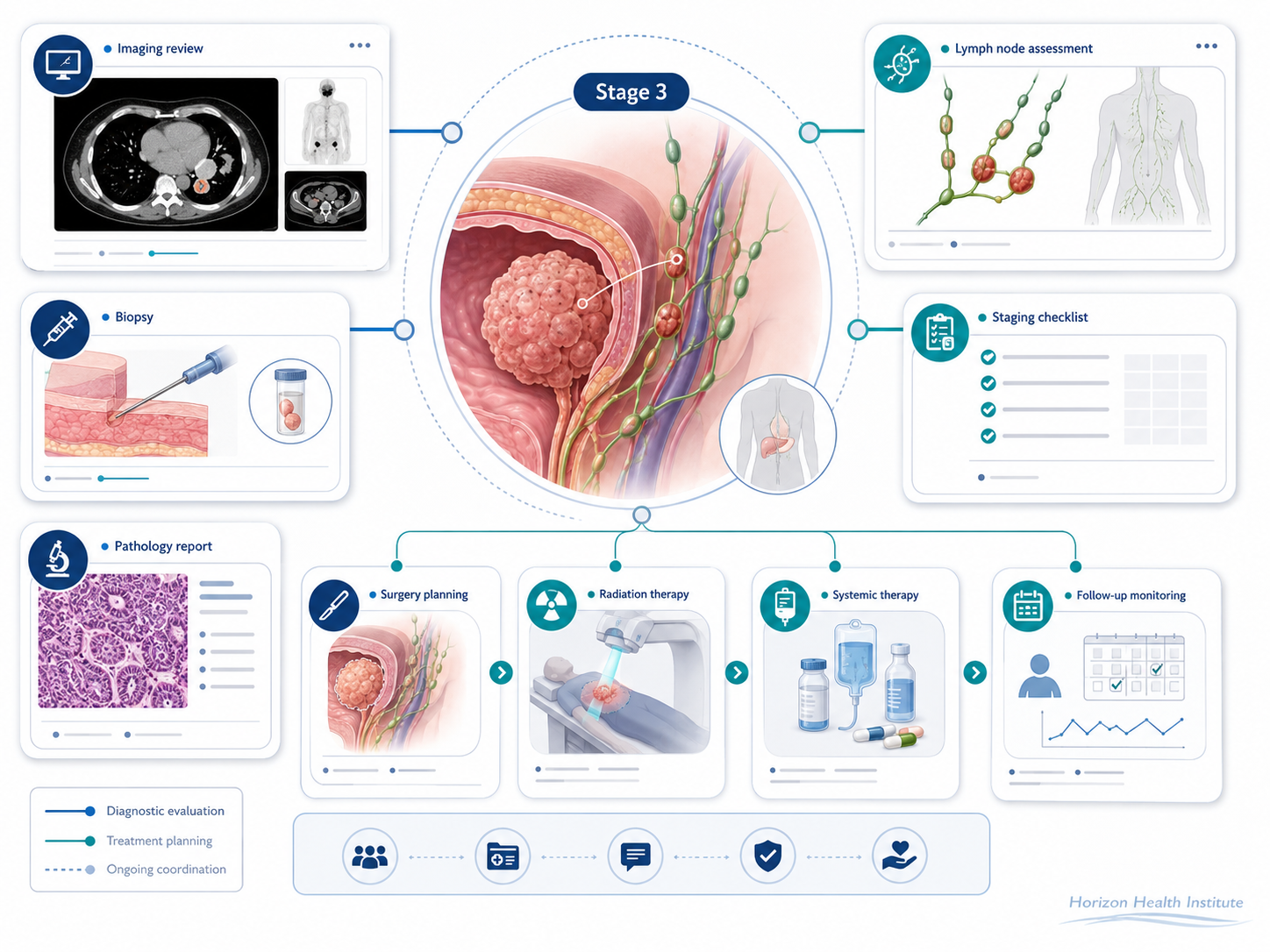
How Stage 3 Cancer Is Diagnosed
The stage 3 diagnostic workup is the most comprehensive of any stage — because the stakes of accuracy are highest at this point.
PET Scan — Nearly Universal
A PET scan is ordered for almost all stage 3 evaluations. It detects cancer activity throughout the entire body, identifying any distant deposits that would push the diagnosis to stage 4. A clean PET outside the regional area confirms M0 status — a prerequisite for any curative treatment plan.
Lymph Node Biopsy and Mediastinal Staging (Lung)
For lung cancer, confirming N2 vs N3 requires invasive procedures:
- Endobronchial ultrasound (EBUS): A bronchoscopy-based procedure that biopsies mediastinal nodes without open surgery — now standard at high-volume centers
- Mediastinoscopy: Surgical node sampling; still used when EBUS is insufficient
Multidisciplinary Tumor Board (MDT)
Stage 3 cases are typically presented to a multidisciplinary tumor board — a collaborative review by medical oncologists, surgeons, radiation oncologists, radiologists, and pathologists. MDT review at stage 3 is associated with more accurate staging decisions and better patient outcomes. If your hospital doesn’t routinely do this, a second opinion at a comprehensive cancer center is appropriate.
Molecular and Biomarker Testing
Results at stage 3 shape entire treatment strategies:
- PD-L1 expression (lung, bladder, cervical) — predicts immunotherapy benefit
- EGFR, ALK, ROS1, KRAS G12C (lung) — targeted therapy eligibility
- HER2 status (breast, gastric) — trastuzumab/pertuzumab eligibility
- Microsatellite instability (MSI-H) (colorectal) — immune checkpoint inhibitor benefit
- BRAF V600E (melanoma) — BRAF/MEK inhibitor eligibility
Stage 3 Cancer Treatment Options
Stage 3 treatment is the most complex of any stage. Nearly all patients receive multimodal therapy — two or more treatment types in a carefully sequenced plan. The right sequence depends on cancer type, substage, molecular profile, and resectability.
Concurrent Chemoradiation (CRT)
Concurrent chemoradiation — giving chemotherapy and radiation simultaneously — is the cornerstone for many unresectable stage 3 cancers. Chemotherapy acts as a radiosensitizer, making cancer cells more vulnerable to radiation. CRT is the primary treatment for unresectable NSCLC, cervical stage 3, head and neck stage 3, locally advanced rectal cancer (as neoadjuvant), and esophageal stage 3.
Durvalumab Consolidation — A Landmark Advance for Stage 3 Lung Cancer
For unresectable NSCLC stage 3 patients who do not progress after definitive chemoradiation, durvalumab (Imfinzi) is given for up to 12 months as consolidation immunotherapy. The PACIFIC trial established this as standard of care: 5-year overall survival with durvalumab reached ~43%, compared to ~33% with placebo — one of the most significant survival improvements in stage 3 lung cancer in decades.
Trimodality Therapy (Neoadjuvant CRT → Surgery → Adjuvant)
For resectable stage 3 cancers, the standard is often a three-part sequence: neoadjuvant chemoradiation to shrink the tumor → surgery to remove it → adjuvant therapy to reduce recurrence risk. Used for resectable lung 3A, locally advanced rectal cancer, esophageal stage 3, and some head and neck cases.
Neoadjuvant Chemotherapy Then Surgery (Breast Stage 3)
Systemic chemotherapy is given first to reduce tumor and lymph node burden, followed by surgery. Patients who achieve pathologic complete response (pCR) — no cancer found in the removed tissue — have significantly better long-term outcomes. For HER2+ or TNBC patients without pCR, additional targeted or immunotherapy after surgery further reduces recurrence risk.
Immunotherapy at Stage 3
- Durvalumab (NSCLC, PACIFIC trial): ~43% 5-year OS after CRT in unresectable stage 3
- Pembrolizumab (melanoma stage 3, adjuvant): KEYNOTE-716 — significantly reduced recurrence after surgery
- Pembrolizumab (TNBC, neoadjuvant): KEYNOTE-522 — improved pCR and event-free survival
- Nivolumab (esophageal, adjuvant): CheckMate 577 — improved disease-free survival after CRT + surgery
Hormone and Targeted Therapy
- Prostate stage 3 (high-risk): Long-duration ADT (2–3 years) + external beam radiation — standard of care
- HR+ breast cancer stage 3: Tamoxifen or aromatase inhibitors for 5–10 years after primary treatment
- HER2+ breast cancer stage 3: Trastuzumab + pertuzumab during neoadjuvant/adjuvant; T-DM1 for residual disease post-pCR failure
- EGFR+ NSCLC: Osimertinib adjuvant after surgery/CRT for eligible patients
- Gastric/GEJ stage 3: FLOT regimen (perioperative) improved 5-year OS from 24% to 45% in resectable cases (FLOT4 trial, Lancet 2019)
Can Stage 3 Cancer Be Cured?
For most stage 3 cancers, yes — treatment is undertaken with curative intent, meaning the goal is elimination of all cancer, not symptom management alone. The honest nuance is that cure rates at stage 3 are lower than at earlier stages, and recurrence risk is higher. But “curative intent” reflects what clinical data show is achievable.
After completing treatment, intensive surveillance continues:
- Imaging and tumor markers every 3–4 months for the first two years
- Many recurrences are caught early, while still treatable
- If cancer does recur, it often comes back locally (still regional) rather than immediately as distant metastasis
For a clear picture of what stage 4 — true metastatic cancer — looks like and what modern treatment can accomplish when cancer reaches distant organs, our metastatic cancer guide explains that stage in full detail.
Questions to Ask After a Stage 3 Diagnosis
- What is my exact substage (3A, 3B, 3C) and what does it mean for my specific treatment?
- Is my cancer considered resectable or unresectable — and what determines that?
- Will I receive chemoradiation, surgery, or both — and in what sequence?
- Will my case be reviewed by a multidisciplinary tumor board?
- Has my tumor been tested for PD-L1, MSI, EGFR, HER2, or other relevant biomarkers?
- Am I eligible for immunotherapy — as consolidation, neoadjuvant, or adjuvant therapy?
- Should I consider a clinical trial at this stage?
- What are the short-term and long-term side effects of the recommended treatment?
- Should I seek a second opinion at a comprehensive cancer center?
- What follow-up schedule will I need after completing treatment?
Frequently Asked Questions
Sources
- National Cancer Institute — Cancer Staging. cancer.gov
- NCI SEER Program — Cancer Stat Facts: 5-Year Relative Survival Rates by Stage (2023). seer.cancer.gov
- American Cancer Society — Cancer Facts & Figures 2024. cancer.org
- Antonia SJ et al. — Durvalumab after Chemoradiotherapy in Stage III Non–Small-Cell Lung Cancer (PACIFIC). NEJM 2022
- Mayo Clinic — Cancer staging. mayoclinic.org
- ASCO Cancer.Net — Stages of Cancer. cancer.net