
Urinary symptoms are extraordinarily common and almost always have a benign explanation. Urinary tract infections, benign prostatic hyperplasia, overactive bladder, kidney stones — these are the bread and butter of primary care and urology. Most urinary symptoms investigated appropriately reveal nothing malignant.
But there are scenarios where urinary symptoms — particularly when they don’t respond to treatment, recur without explanation, or occur in the right clinical context — represent the earliest signal of bladder cancer, prostate cancer, kidney cancer, or a gynecologic malignancy. Knowing when to push for more than another antibiotic course could be life-saving.
The Classification of Urinary Symptoms
Urologists classify lower urinary tract symptoms (LUTS) into two broad categories, and different cancers tend to produce different patterns:
Irritative/storage symptoms: Frequency (urinating more often than usual), urgency (sudden compelling urge to urinate), dysuria (burning or pain during urination), nocturia (waking at night to urinate), and urge incontinence. These symptoms suggest bladder mucosal irritation — characteristic of bladder cancer, UTI, or interstitial cystitis.
Obstructive/voiding symptoms: Hesitancy (delay in starting to urinate), weak stream, straining, incomplete emptying, intermittent flow, and terminal dribbling. These symptoms suggest mechanical obstruction of the urethra or bladder outlet — characteristic of BPH, locally advanced prostate cancer, or pelvic mass.
Bladder Cancer: When “Recurring UTIs” Aren’t Infections
Bladder cancer is the fourth most common cancer in American men and is responsible for approximately 17,000 deaths annually. Despite this burden, it receives far less public awareness than breast or prostate cancer — with significant consequences for diagnostic delay.
While hematuria (blood in urine) is the classic presenting symptom, occurring in 90 percent of bladder cancer patients, irritative urinary symptoms without any blood occur in 20 to 30 percent. These symptoms — frequency, urgency, dysuria — are clinically identical to those produced by a UTI.
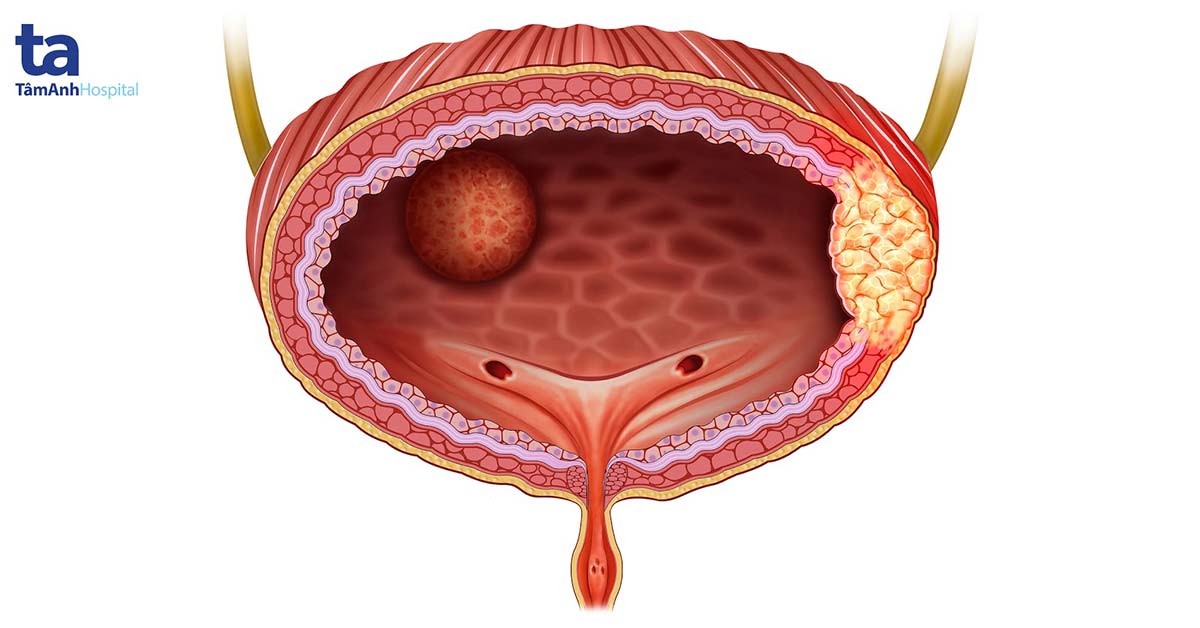
Carcinoma in situ (CIS) of the bladder is a flat, high-grade malignant lesion that causes severe irritative symptoms — urgency, frequency, dysuria — sometimes without any hematuria. CIS is completely invisible on CT and ultrasound. It cannot be found on urine cytology with high sensitivity. The only reliable diagnosis is cystoscopy with bladder biopsies.
The pattern of diagnostic failure: Patient develops irritative urinary symptoms → treated as UTI with antibiotics → temporarily improves → “recurs” → another antibiotic course → cycle continues for 12+ months before cystoscopy is performed. CIS carries a high risk of progression to muscle-invasive bladder cancer if untreated.
Cancer Associations by Urinary Symptom Pattern
| Symptom Pattern | Cancer to Consider | Key Clinical Feature |
|---|---|---|
| Frequency + urgency + dysuria, no proven UTI | Bladder cancer (CIS) | Negative urine culture; doesn’t respond to antibiotics |
| Painless visible blood in urine | Bladder cancer, RCC, upper tract urothelial | See blood in urine article |
| Hesitancy + weak stream (men ≥50) | Prostate cancer (locally advanced); BPH first | PSA + DRE; mpMRI if elevated |
| Urinary frequency + bloating (women ≥40) | Ovarian cancer (bladder compression) | Pelvic exam + TVS + CA-125 |
| Pneumaturia (air in urine) | Colorectal cancer (colovesical fistula) | Emergency evaluation — pathognomonic of fistula |
| Urinary frequency + flank pain | Renal/ureteral obstruction from tumor or nodes | CT abdomen to evaluate upper tract |
Prostate Cancer and Urinary Symptoms: The Important Nuance
Prostate cancer has a complicated relationship with urinary symptoms. The urinary symptoms commonly attributed to prostate cancer — hesitancy, weak stream, frequency, nocturia — are actually symptoms of benign prostatic hyperplasia (BPH), the non-cancerous enlargement of the prostate affecting the majority of men over 50.
Early-stage prostate cancer does not cause urinary symptoms. Most cancers detected at the curable stage are found through PSA screening in asymptomatic men. A man waiting for urinary symptoms to prompt investigation is not employing an effective detection strategy. What detects prostate cancer early is PSA blood testing and digital rectal examination.
Locally advanced prostate cancer can eventually cause obstructive LUTS through direct invasion of the bladder neck or urethra — but at this stage, the cancer has grown well beyond the prostate capsule. Multiparametric MRI (mpMRI) of the prostate is now standard practice before biopsy, with PI-RADS scoring guiding biopsy decisions.
Ovarian Cancer: The Bladder Is the Canary
Ovarian cancer is the deadliest gynecologic cancer, largely because it is diagnosed at Stage III or IV in the majority of cases. A key reason for late-stage diagnosis is that its early symptom profile overlaps entirely with IBS and overactive bladder.
The Ovarian Cancer Symptom Index identifies four key symptoms: bloating, pelvic or abdominal pain, difficulty eating/early satiety, and urinary urgency or frequency. When these occur more than 12 days per month and have been present for less than one year, the specificity for ovarian cancer is significantly higher than for benign functional disorders.
A woman over 40 with new urinary urgency and frequency — particularly combined with bloating or early satiety — should have a pelvic examination, transvaginal ultrasound, and serum CA-125. Diagnosing this presentation as “overactive bladder” and treating with anticholinergics without pelvic evaluation is a common and potentially fatal error.
In women ≥40, the following combination occurring >12 days per month and present <1 year should trigger pelvic evaluation:
- Bloating or abdominal distension
- Pelvic or abdominal pain
- Difficulty eating or feeling full quickly
- Urinary urgency or frequency (new onset)
When Urinary Symptoms Require More Than Antibiotics
Urinary tract infections should respond to 3–7 days of appropriate antibiotics. These scenarios should trigger cancer-directed evaluation rather than another antibiotic course:
- Urinary symptoms without a documented positive culture (no infection proven)
- Urinary symptoms that persist despite appropriate antibiotic treatment for culture-proven UTI
- UTI-like symptoms recurring 3+ times per year without obvious predisposing cause
- UA showing blood or abnormal cells without bacteria
- Urinary symptoms with any visible blood in urine
- Urinary symptoms with weight loss or fatigue
- Air in the urine stream (pneumaturia) — emergency evaluation for colovesical fistula
Frequently Asked Questions
References
- NCCN Clinical Practice Guidelines: Bladder Cancer; Prostate Cancer. 2024.
- AUA Guidelines: Early Detection of Prostate Cancer; Benign Prostatic Hyperplasia. 2023.
- Goff BA, et al. Ovarian carcinoma diagnosis. Cancer. 2000.
- Siegel RL, et al. Cancer Statistics 2023. CA Cancer J Clin. 2023.
- USPSTF. Screening for Prostate Cancer. JAMA. 2018.
- Ramirez PT, et al. Cervical cancer management. N Engl J Med. 2022.