Cancer monitoring is the systematic, ongoing process of evaluating disease status in patients who have been diagnosed with cancer — whether during active treatment, after completing curative therapy, during intentional observation of a low-risk tumor, or while managing advanced disease over time. Understanding what cancer monitoring involves, and why each tool is used, helps patients make sense of what can otherwise feel like an endless series of blood draws, scans, and appointments.
Cancer monitoring is not the same as cancer screening, which detects cancer in people with no prior diagnosis. It is also distinct from cancer follow-up care, which focuses on survivorship issues like late effects and psychosocial support. Cancer monitoring is specifically about tracking what the cancer is doing — whether it is responding to treatment, remaining stable, growing, or returning after appearing to have been eliminated.
What Is Cancer Monitoring?
Modern cancer monitoring encompasses four distinct contexts:
- On-treatment monitoring: Tracking response to chemotherapy, targeted therapy, immunotherapy, or radiation — assessing whether the cancer is shrinking, stable, or growing while on active therapy
- Post-treatment surveillance: Periodic evaluation after curative-intent treatment to detect recurrence at its earliest, most treatable stage
- Active surveillance: Intentional, structured monitoring of a low-risk tumor without immediate active treatment — curative therapy is deferred but not abandoned; a clear protocol triggers intervention if the cancer changes
- Metastatic disease monitoring: Ongoing assessment to determine whether a treatment regimen is still working and when to change strategies
For more on the survivorship context of monitoring — including late effects, care coordination, and survivorship care plans — see the cancer follow-up care guide. For clinical trials testing next-generation monitoring technologies, see cancer clinical trials.
Tumor Markers — What Blood Tests Can (and Cannot) Tell You
Tumor markers are proteins, antigens, or other substances measurable in blood or body fluids that are produced by cancer cells or by the body in response to cancer. Used serially over time, they provide a trend line your physician can act on — even when a single value in isolation means little.
| Marker | Cancer Type | Primary Monitoring Use |
|---|---|---|
| CEA | Colorectal (primary); breast, lung, gastric | Post-surgical CRC surveillance every 3–6 months × 5 years; rising CEA can identify potentially curable hepatic/pulmonary metastases |
| PSA | Prostate cancer | Active surveillance; biochemical recurrence post-RP (threshold >0.2 ng/mL × 2); post-RT Phoenix criterion (nadir + 2 ng/mL); metastatic monitoring |
| CA-125 | Ovarian cancer | Treatment response; recurrence surveillance; ~80–90% sensitivity for advanced disease; rising CA-125 prompts CT imaging |
| AFP | HCC; non-seminomatous germ cell tumors | HCC surveillance every 6 months (with ultrasound per AASLD); testicular cancer treatment response |
| Beta-hCG | Choriocarcinoma; non-seminoma testicular | One of oncology’s most sensitive markers — even minor post-treatment elevations are clinically significant |
| Thyroglobulin (Tg) | Differentiated thyroid cancer | Post-thyroidectomy; suppressed Tg <0.2 ng/mL = excellent response; rising Tg triggers neck ultrasound ± whole-body scan |
| Calcitonin | Medullary thyroid carcinoma | Primary biomarker for this tumor type; highly sensitive and specific |
| Chromogranin A | Neuroendocrine tumors (NETs) | Disease burden and treatment response monitoring |
| CA 19-9 | Pancreatic; biliary tract cancer | Treatment response monitoring (not useful for screening or early detection) |
| LDH | Lymphoma; melanoma; germ cell tumors | Non-specific disease burden marker; incorporated into staging systems |
| CA 15-3 / CA 27-29 | Breast cancer | Metastatic disease monitoring only — ASCO explicitly does NOT recommend for asymptomatic early-stage surveillance; no survival benefit shown |
Imaging in Cancer Monitoring
CT Scan and RECIST 1.1
CT scanning is the workhorse of cancer response assessment for solid tumors. Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 provides the international standard for measuring tumor response — used in clinical trials and clinical practice alike. Radiologists identify up to 5 measurable target lesions and track the sum of their longest diameters across scans.
In most metastatic solid tumors, CT imaging is repeated every 8–12 weeks (every 2–3 treatment cycles) during first-line treatment. When your oncologist says your cancer has “partially responded” or “progressed,” they are usually applying RECIST criteria even if they do not use that term. Stable disease — which might sound like bad news — can represent an excellent outcome for many advanced cancers where the goal is disease control rather than cure.
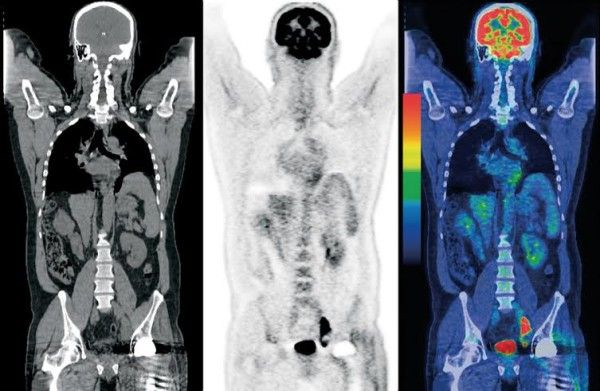
PET-CT and the Deauville Scale
PET-CT exploits the Warburg effect — cancer cells consume glucose at dramatically higher rates than normal tissue. FDG (18F-fluorodeoxyglucose), a radioactive glucose analog, accumulates in metabolically active tumor tissue and appears as bright “hot spots” on imaging. The Lugano classification and Deauville 5-point scale are standard for lymphoma response: Deauville 1–2 = complete metabolic response; Deauville 3 = borderline (context-dependent); Deauville 4–5 = residual metabolic disease. The RATHL trial (Johnson PWM, NEJM 2016) established that Hodgkin lymphoma patients with a negative interim PET at 2 cycles can safely omit bleomycin, reducing pulmonary toxicity without compromising cure rates.
PSMA-PET (piflufolastat/Pylarify; flotufolastat) has transformed prostate cancer monitoring — identifying metastatic disease at PSA levels below 1 ng/mL where conventional CT and bone scan are essentially blind.
MRI and the Pseudoprogression Challenge
MRI is essential for brain tumor monitoring, liver characterization, pelvic tumors, and bone marrow assessment. In patients with glioblastoma who undergo concurrent chemoradiation with temozolomide, 20–30% show apparent tumor enlargement on the first post-treatment MRI (typically 6–12 weeks after radiation) — representing inflammatory pseudoprogression rather than true cancer growth. Multiparametric MRI (mpMRI) with PI-RADS scoring is now standard in prostate cancer active surveillance, with a negative predictive value approaching 90% for ruling out clinically significant cancer in PI-RADS 1–2 lesions.
Liquid Biopsy — The Future of Cancer Monitoring
Liquid biopsy is one of the most rapidly evolving areas in oncology. Circulating tumor DNA (ctDNA) — fragments of cancer DNA shed into the bloodstream during cell death — has a plasma half-life of approximately 90 minutes, meaning ctDNA levels reflect current tumor burden almost in real time. This contrasts sharply with imaging, which can only detect anatomically visible disease that has already grown to a detectable size.
Resistance mutation detection. The EGFR T790M plasma test is now a standard alternative to repeat tissue biopsy in patients with EGFR-mutant NSCLC who progress on first-line EGFR TKI therapy. Plasma T790M sensitivity is approximately 70% versus ~80% for tissue, but avoids an invasive procedure. T790M-positive patients (plasma or tissue) are eligible for osimertinib.
Post-surgical minimal residual disease (MRD) detection. The landmark DYNAMIC trial established ctDNA-guided adjuvant chemotherapy in stage II colorectal cancer:
First prospectively validated biomarker for guiding adjuvant chemotherapy in early-stage colorectal cancer — ctDNA-negative patients achieved excellent outcomes without chemotherapy and its associated toxicity.
Early recurrence detection. In breast cancer, ctDNA becomes detectable a median of 8–10 months before recurrence is visible on conventional CT imaging — and months earlier in several other solid tumor types as well. Whether acting on ctDNA-positive results before imaging-detectable disease improves survival is under active investigation in multiple trials (MERMAID-2 for lung cancer; INTERCEPT for various solid tumors).

Circulating tumor cells (CTCs) — intact cancer cells shed from tumors into the bloodstream — are measured by the FDA-cleared CellSearch system. In metastatic breast cancer, ≥5 CTCs per 7.5 mL is associated with significantly shorter progression-free and overall survival (Cristofanilli M et al., NEJM 2004). Multiple FDA-cleared and breakthrough-designated ctDNA MRD tests are available: Signatera (Natera), Guardant Reveal, and Foundation One Tracker. Liquid biopsy is a powerful complement — not yet a replacement — for tissue biopsy, which remains essential for initial diagnosis and comprehensive molecular profiling.
Active Surveillance — When Monitoring Is the Treatment
Active surveillance is a structured, curative-intent monitoring program for low-risk cancers — curative treatment is deferred but not abandoned. It is fundamentally different from watchful waiting (expectant management), which is palliative: the patient is observed with no plan for curative intervention, and therapy starts only when symptoms require it.
Prostate cancer active surveillance is the NCCN-preferred option for low-risk localized prostate cancer (Grade Group 1; some favorable intermediate-risk patients):
- PSA every 3–6 months for year 1; then every 6–12 months if stable
- Multiparametric MRI at baseline; repeated for PSA changes or at 1-year intervals
- Confirmatory biopsy within 6–12 months; repeat systematic ± MRI-targeted biopsy every 1–4 years
- Triggers to convert to active treatment: grade reclassification (GG≥2); PSA doubling time <3 months; PI-RADS upgrade to 4–5; patient preference
The PROTECT trial at 15-year follow-up (Hamdy FC et al., NEJM 2023) found prostate cancer-specific mortality of 3.1% in the active monitoring arm versus 2.4% surgery and 3.0% radiation — not statistically significant (p=0.53). However, the active monitoring arm had more distant metastases (9.4% vs. 4.7% for surgery, p=0.008) — confirming that vigilant monitoring adherence is what makes active surveillance safe. Other cancers on active surveillance include low-risk papillary thyroid microcarcinomas, asymptomatic follicular lymphoma, small renal masses, and selected early-stage CLL.
Monitoring Challenges: Immunotherapy, Scanxiety, and Hematology MRD
iRECIST and Pseudoprogression in Immunotherapy
Immunotherapy creates monitoring challenges that standard RECIST 1.1 was not designed to handle. Immune cell infiltration into tumors can transiently increase tumor size — making cancer appear to worsen even when it is responding. Pseudoprogression affects approximately 5–10% of immunotherapy-treated patients and can lead to premature treatment discontinuation.
The iRECIST criteria allow “unconfirmed progressive disease” (iUPD): if a patient appears to progress but is clinically stable, treatment can continue and confirmatory imaging performed 4–8 weeks later. If progression is confirmed, it becomes “immune confirmed progressive disease” (iCPD), driving a treatment change. The opposite phenomenon — hyperprogression (paradoxical tumor acceleration in ~10–15% of patients) — is associated with MDM2/MDM4 amplification and remains an active research area.
MRD in Hematologic Malignancies
- ALL: MRD <0.01% (10⁻⁴) after induction drives treatment intensity; NGS-based assays detecting 10⁻⁶ are now available
- Multiple myeloma: MRD negativity by NGS (ClonoSEQ, FDA-cleared) or PET-CT is an emerging regulatory endpoint; sustained MRD negativity predicts significantly prolonged PFS
- CLL: Undetectable MRD (uMRD) after fixed-duration venetoclax-based therapy predicts prolonged disease-free intervals without continuous therapy
- AML: MRD by flow cytometry or NPM1/FLT3-ITD PCR at day 28 predicts relapse risk and guides consolidation intensity
Scanxiety and Monitoring Interval Optimization
Scanxiety — anticipatory anxiety surrounding scheduled scans and waiting for results — affects 30–40% of cancer patients at clinically significant levels. Evidence shows extending surveillance intervals in patients who remain recurrence-free reduces scanxiety without increasing the risk of missing recurrence. If monitoring-related anxiety is affecting your quality of life, ask your oncologist whether your surveillance schedule can be safely extended. For comprehensive psychosocial survivorship support, see the cancer follow-up care article. For innovative monitoring technologies in trials, see cancer clinical trials.
Frequently Asked Questions
- Tie J et al. — DYNAMIC trial ctDNA-guided adjuvant chemotherapy stage II CRC; NEJM 2022
- Hamdy FC, Lane JA et al. — PROTECT trial 15-year AS vs. treatment prostate cancer; NEJM 2023
- Johnson PWM et al. — RATHL trial interim PET Hodgkin lymphoma; NEJM 2016
- Cristofanilli M et al. — CTC prognostic value metastatic breast cancer; NEJM 2004
- Eisenhauer EA et al. — RECIST 1.1 criteria; Eur J Cancer 2009
- Newcomb LF et al. — CANARY AS conversion data; JCO 2016
- Champiat S et al. — Hyperprogression definition and incidence; Clin Cancer Res 2017
- ASCO — Colorectal cancer surveillance guideline; 2013/updated
- AASLD — HCC surveillance in cirrhosis; Hepatology 2018
- AUA — Prostate cancer active surveillance guideline; 2023
- NCI — Cancer diagnosis and staging resources: cancer.gov/about-cancer/diagnosis-staging
- NCCN Guidelines — Disease-specific monitoring: nccn.org/guidelines
This article is for educational purposes only and does not constitute medical advice. Discuss all cancer monitoring decisions with your oncology care team.
Pingback: Cancer Remission: What It Means and How It's Measured - Horizon Health Guide