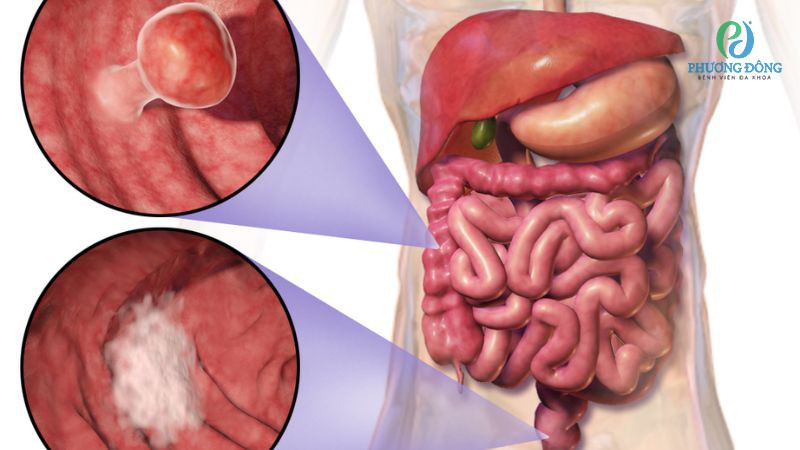
Colon cancer develops in the large intestine — the five-foot tube that forms the final section of the digestive tract before the rectum. In 2024, an estimated 106,590 Americans received a colon cancer diagnosis, making it the third most common cancer in the United States for both men and women. Despite that number, colon cancer carries a genuine quality that very few cancers can claim: it can be prevented, not just detected early.
The reason is biological timing. Colon cancer almost never develops from normal tissue overnight. It grows from polyps — benign growths on the colon lining — and that progression from normal cell to polyp to early cancer typically takes ten to fifteen years. A colonoscopy that finds and removes a polyp during that window doesn’t just find cancer early; it eliminates the cancer before it ever forms. That is the single most important fact about colon cancer.
What Is Colon Cancer?
Colon cancer is cancer that begins in the cells lining the colon — the large intestine. It is distinct from rectal cancer, which begins in the rectum (the final 12–15 centimeters before the anus). Together they are often grouped as “colorectal cancer,” but they are treated differently and have different anatomical behaviors, which is why distinguishing between them matters clinically.
About 95% of colon cancers are adenocarcinomas, arising from glandular cells in the inner lining of the colon. The colon itself is divided into sections: the ascending colon runs up the right side of the abdomen; the transverse colon crosses horizontally; the descending colon runs down the left side; the sigmoid colon curves into the pelvis before meeting the rectum. Where in the colon a tumor develops has profound implications for how it presents, how it grows, and how it is surgically removed.
Colon cancer accounts for roughly 70% of all colorectal cancers. About 25% of colon cancers arise in the sigmoid colon, making it the most common single location. The ascending (right) colon accounts for another 20%. This distribution matters because right-sided and left-sided colon cancers behave quite differently in terms of symptoms, molecular biology, and response to certain targeted therapies.
What Causes Colon Cancer — The Polyp Pathway
Most colon cancers do not arise from normal tissue. They develop through a stepwise progression called the adenoma-carcinoma sequence — a process so well characterized that it forms the scientific basis for colonoscopy as a cancer-prevention tool. The sequence works like this: normal colon epithelium acquires a mutation in the APC gene — the “gatekeeper” mutation of colorectal cancer — which allows cells to grow into a small adenomatous polyp. Over years, that polyp accumulates additional mutations in KRAS, SMAD4, and TP53, each one pushing the cells further toward malignancy. The full progression from normal tissue to invasive cancer typically takes ten to fifteen years.
This classical pathway — chromosomal instability (CIN) — accounts for roughly 80% of colon cancers. The other important pathway is the serrated pathway, in which sessile serrated lesions (flat, pale growths that are notoriously difficult to spot on colonoscopy) accumulate epigenetic changes, particularly silencing of the MLH1 gene. This disables the DNA mismatch repair system and produces microsatellite instability-high (MSI-H) cancer — a subtype that responds strikingly well to immunotherapy in a way that most other colon cancers do not.
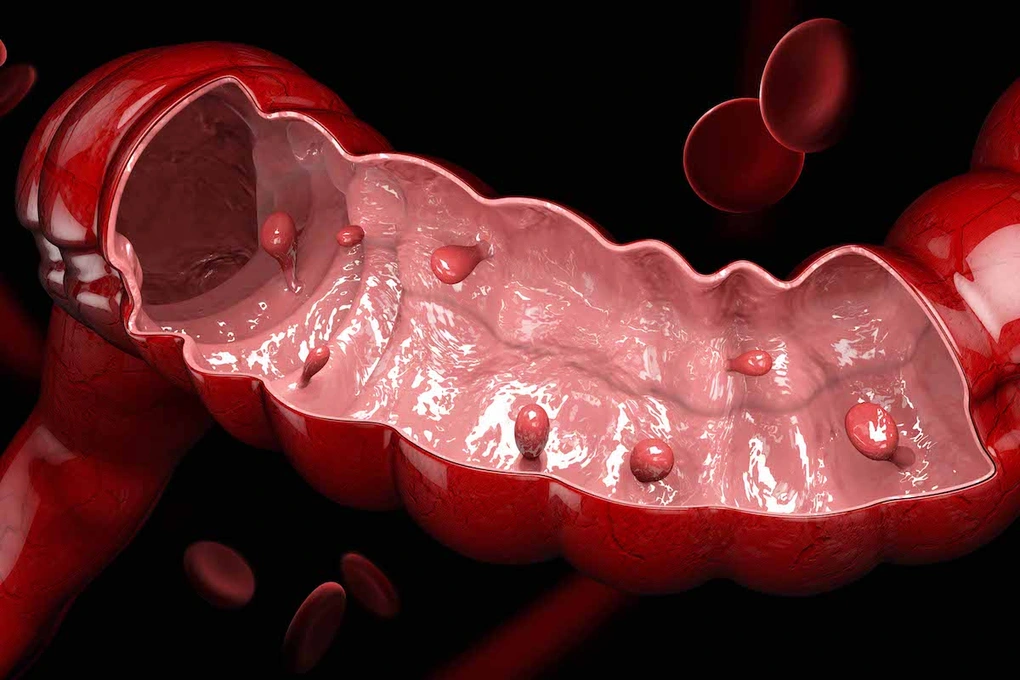
What makes a polyp dangerous? Size and type are the two key factors:
- Tubular adenomas smaller than 5mm: malignant transformation risk under 1%
- Tubular adenomas 5–9mm: approximately 1–2% lifetime cancer risk
- Adenomas 10mm or larger (“advanced adenomas”): approximately 5–10% risk; require close surveillance
- Adenomas larger than 20mm: up to 25% malignant transformation risk
- Villous adenomas: highest risk per unit size; flat and difficult to detect; 10–15% overall transformation rate
- Sessile serrated lesions: substantial malignant potential; often right-sided and pale-colored, making them among the most commonly missed lesions on colonoscopy
The practical implication is that not all polyps are the same. The pathology report from a colonoscopy polypectomy directly determines how soon you need the next scope — anywhere from one year (for large or high-risk adenomas) to ten years (for low-risk tubular adenomas or a clean exam).
Who Is at Risk?
Age is the strongest single risk factor. Colon cancer is rare before 40 and rises steeply after 50, with about 90% of cases occurring in people over 50. The USPSTF recommends beginning average-risk screening at 45, reflecting the well-documented rise in early-onset colon cancer — a trend that has increased approximately 2% per year since the 1990s.
Hereditary syndromes drive a meaningful fraction of cases. Lynch syndrome, caused by inherited mutations in mismatch repair genes (MLH1, MSH2, MSH6, or PMS2), confers a 50–80% lifetime colon cancer risk. Lynch-associated colon cancers tend to arise in the right colon at a younger average age (around 44–46 years) and are nearly always MSI-H. Familial adenomatous polyposis (FAP), caused by APC mutations, produces hundreds to thousands of polyps in adolescence, with near-100% lifetime cancer risk without prophylactic colectomy.
The majority of colon cancers are sporadic, shaped by lifestyle and environment:
- Red meat (more than two servings per week): approximately 20–30% increased risk; processed meat (IARC Group 1 carcinogen) raises risk by about 18% per 50 grams per day
- Physical inactivity: 30–40% elevated risk; regular exercise is among the most evidence-based protective behaviors
- Obesity, particularly abdominal obesity: 1.5 to 2 times higher risk
- Smoking: 30–40% increased risk
- Heavy alcohol use (two or more drinks daily): 20–30% increased risk
- Type 2 diabetes: approximately 1.3–1.5 times elevated risk
- Inflammatory bowel disease: risk rises significantly after 8–10 years of extensive colitis
On the protective side, regular physical activity reduces risk by 30–40%. Long-term low-dose aspirin (at least five years) reduces colon cancer risk by approximately 20–25%. Dietary fiber, fruits, and vegetables are consistently associated with lower rates.
Symptoms of Colon Cancer
The most critical thing to understand about colon cancer symptoms is that early-stage tumors frequently produce no symptoms at all. Stage I colon cancer — where cure rates exceed 90% — is almost always asymptomatic. Waiting for symptoms before getting a colonoscopy is, in most cases, waiting too long.
When symptoms do appear, their character depends heavily on where in the colon the tumor sits. The colon’s anatomy creates two fundamentally different symptom profiles.
Right colon tumors (ascending colon, cecum): The right colon is wide — roughly the diameter of a baseball — and stool here is still liquid. A tumor growing in this space can become very large before causing any obstruction. The bloodshed is typically occult: the tumor bleeds slowly, but since stool is liquid and blood mixes throughout, it is invisible to the eye. The result is chronic, invisible blood loss leading to iron deficiency anemia. Patients come to their doctor complaining of fatigue, weakness, shortness of breath, or palpitations and are told on blood work that their hemoglobin has quietly fallen to alarmingly low levels. The tumor in their right colon has been bleeding for months. This is why iron deficiency anemia in a man, or in a post-menopausal woman without another obvious cause, must be investigated with colonoscopy — not just treated with iron supplements.
Left colon and sigmoid tumors: The left colon is narrower — roughly the diameter of a sausage — and stool here is formed. A tumor in this segment acts more like a partial obstruction. Common presentations include visible rectal bleeding (dark or bright red), pencil-thin stools (from stool being forced through a narrowed lumen), alternating constipation and diarrhea, and cramping or urgency. Patients often notice these symptoms but attribute the bleeding to hemorrhoids — a dangerous assumption that delays diagnosis for months.
Iron deficiency anemia in a man or post-menopausal woman without an obvious cause always warrants a colonoscopy — not just iron replacement. Many right-sided colon cancers are first suspected from a blood test, not from any bleeding anyone can see. Treating the anemia without investigating its source is one of the most common delays in colon cancer diagnosis.
General alarm symptoms that should prompt evaluation at any age:
- Blood in or on stool — any amount, any color
- Unexplained change in bowel habits lasting more than two to three weeks
- Unintentional weight loss
- Persistent abdominal pain or cramping
- Fatigue disproportionate to other causes, especially with unexplained anemia
- Feeling that the bowel doesn’t fully empty after a movement
- A palpable abdominal mass (a late finding)
Diagnosis and Staging
Colonoscopy with biopsy is the definitive diagnostic procedure. Once cancer is confirmed, CT scanning of the chest, abdomen, and pelvis stages the disease — identifying liver metastases (the most common site of spread), lymph node involvement, and peritoneal disease. CEA is measured at baseline as a reference point for monitoring after treatment.
For cancer beyond Stage I, molecular testing of tumor tissue is essential:
- MSI/MMR status: Identifies MSI-H tumors and, for Stage IV disease, predicts response to immunotherapy
- KRAS and NRAS mutations: Present in about 50–60% of cases; exclude use of anti-EGFR antibodies
- BRAF V600E: Present in about 10%; marks a more aggressive subtype
- HER2 amplification: In approximately 3–4% of RAS/BRAF wild-type cases
Five-year survival by stage: Stage I approximately 90%; Stage IIA approximately 85%; Stage IIB approximately 72%; Stage IIIA approximately 90%; Stage IIIB approximately 72%; Stage IIIC approximately 53%; Stage IVA approximately 37%; Stage IVB approximately 14%.
Treatment by Stage
Stage I: Surgery alone — a right hemicolectomy, sigmoid colectomy, or left hemicolectomy depending on the tumor’s location. A minimum of 12 lymph nodes must be examined to accurately confirm N0 staging. Laparoscopic and robotic approaches produce equivalent oncologic outcomes. Five-year survival exceeds 90%.
Stage II: Surgery with adjuvant FOLFOX reserved for high-risk features: T4 tumor, perforation, fewer than 12 lymph nodes examined, lymphovascular invasion, or poorly differentiated histology.
Stage III: Surgery followed by six months of adjuvant FOLFOX or CAPOX — the standard of care established in the MOSAIC trial. Surveillance begins at completion of chemotherapy.
Stage IV — resectable disease: Perioperative FOLFOX combined with surgical resection of the primary tumor and metastases has achieved five-year survival rates of 30–40% for patients with liver-limited or lung-limited disease at experienced centers.
Stage IV — unresectable disease: First-line FOLFOX or FOLFIRI combined with targeted biologics selected by molecular profile. Bevacizumab for RAS-mutant tumors; cetuximab or panitumumab for RAS wild-type, left-sided tumors (right-sided colon cancers show poor responses to anti-EGFR therapy regardless of RAS status). Pembrolizumab for MSI-H/dMMR tumors (about 15% of Stage IV cases). Encorafenib plus cetuximab for BRAF V600E–mutant tumors in later lines. Median OS with modern regimens now exceeds 30 months.
Surveillance after surgery: Colonoscopy at one year, then three years, then every five years if normal. CT every 6–12 months for three to five years. CEA every 3–6 months for the first two years. Recurrence most commonly occurs within the first two to three years.
Frequently Asked Questions
Is colon cancer the same as colorectal cancer?
Not exactly. “Colorectal cancer” covers both colon and rectal cancers together. Colon cancer specifically refers to the large intestine, excluding the rectum. About 70% of colorectal cancers are colon cancers. For a full overview, see our colorectal cancer guide.
What is the most common early sign of colon cancer?
For right-sided colon cancer, the most common early finding is iron deficiency anemia on a blood test — not visible bleeding. For left-sided and sigmoid cancer, visible rectal bleeding is the most common symptom. In many patients, Stage I colon cancer produces no signs at all. For more detail, see our colon cancer symptoms guide.
Can colon cancer be cured?
Yes — Stage I colon cancer is cured in over 90% of patients with surgery alone. Stage III is treated with curative intent. Even limited Stage IV disease with resectable liver-only or lung-only metastases carries a 30–40% five-year survival with aggressive combined treatment.
What is the difference between a colon polyp and colon cancer?
A polyp is benign. Most never become cancer and can be completely removed during colonoscopy. An adenomatous polyp has the potential to progress to cancer over many years — removing it is curative of that future cancer. Colon cancer is an invasive malignancy that has breached the colon lining and may spread to lymph nodes or distant organs. For more on prevention, see our guide to colorectal cancer screening.
Sources
- American Cancer Society. Cancer Facts & Figures 2024. cancer.org
- US Preventive Services Task Force. Colorectal Cancer: Screening, 2021. uspreventiveservicestaskforce.org
- Siegel RL et al. Colorectal cancer statistics, 2023. CA: A Cancer Journal for Clinicians, 2023.
Related reading: Colorectal cancer overview | Colon cancer symptoms | Colorectal cancer screening | Colonoscopy guide
Systemic Treatment Advances in Colon Cancer
The treatment of metastatic colon cancer has been transformed by targeted therapies that address specific molecular alterations in tumor biology. Understanding these advances is increasingly important for patients because molecular profiling of the tumor now directly determines which systemic therapies are appropriate.
RAS/BRAF mutation status: KRAS and NRAS mutations (collectively “RAS mutations”) are present in approximately 50–55% of colorectal cancers and predict resistance to anti-EGFR antibodies (cetuximab, panitumumab). Testing for RAS mutations is standard in metastatic colon cancer and determines whether anti-EGFR therapy is appropriate. BRAF V600E mutations occur in approximately 8–12% of colorectal cancers and confer a poor prognosis with standard chemotherapy. The BEACON CRC trial established the BRAF/MEK/EGFR inhibitor combination (encorafenib + cetuximab ± binimetinib) as a new standard for BRAF V600E-mutant metastatic colorectal cancer.
HER2 amplification: Approximately 3–5% of metastatic colorectal cancers have HER2 amplification and can respond to anti-HER2 therapies including trastuzumab with tucatinib (approved by FDA in 2023) or trastuzumab/pertuzumab combination. HER2 testing is becoming part of standard molecular profiling in metastatic disease.
dMMR/MSI-H immunotherapy: Mismatch repair-deficient (dMMR) or microsatellite instability-high (MSI-H) colorectal cancers — approximately 5% of metastatic cases — respond to PD-1 checkpoint inhibitors. Pembrolizumab is approved as first-line monotherapy for dMMR/MSI-H metastatic colorectal cancer based on the KEYNOTE-177 trial, which showed superior progression-free survival compared to standard chemotherapy. Microsatellite instability testing (by PCR or next-generation sequencing) is standard in all newly diagnosed metastatic colorectal cancer and also has hereditary significance (Lynch syndrome).
For information about which symptoms may indicate colon cancer requiring evaluation, see our guide to colon cancer symptoms. For a comprehensive overview of colorectal cancer including both colon and rectal subtypes, see our main guide to colorectal cancer. For prevention through screening, see our guide to colorectal cancer screening.
Key Resources
- American Cancer Society — Colon and Rectal Cancer
- National Cancer Institute — Colon Cancer Treatment (PDQ)
- NCCN — Colon and Rectal Cancer Guidelines
Hereditary Colon Cancer Syndromes and Genetic Testing
Approximately 5% of colorectal cancers arise in patients with identifiable hereditary cancer syndromes. Recognizing hereditary colorectal cancer is important not only because it affects the individual patient’s surveillance and treatment planning, but because it has direct implications for first-degree relatives who may carry the same germline mutation and be at substantially elevated lifetime risk of colorectal cancer.
Lynch syndrome (hereditary non-polyposis colorectal cancer, HNPCC): Lynch syndrome is the most common hereditary colorectal cancer syndrome, accounting for approximately 3% of all colorectal cancers. It is caused by germline mutations in DNA mismatch repair (MMR) genes: MLH1, MSH2, MSH6, PMS2, or EPCAM. Lynch syndrome confers a lifetime colorectal cancer risk of 25–80% (depending on the specific gene) and also increases risk for endometrial, ovarian, gastric, urinary tract, and other cancers. Lynch syndrome tumors are typically mismatch repair-deficient (dMMR) / microsatellite instability-high (MSI-H), which means they respond to immunotherapy (pembrolizumab is FDA-approved as first-line for dMMR/MSI-H metastatic colorectal cancer). Universal tumor testing (MMR immunohistochemistry or MSI PCR) for Lynch syndrome is now recommended for all newly diagnosed colorectal cancers, regardless of age.
Familial adenomatous polyposis (FAP): FAP is caused by germline mutations in the APC gene and is characterized by hundreds to thousands of colorectal adenomatous polyps, with nearly 100% lifetime risk of colorectal cancer if the colon is not removed. FAP typically presents in the second and third decades of life with polyp development; colorectal cancer typically occurs by the fourth decade without prophylactic colectomy. Attenuated FAP (AFAP), caused by certain APC mutations, is a milder variant with fewer polyps (10–100) and later cancer onset. MUTYH-associated polyposis (MAP) is an autosomal recessive polyposis syndrome caused by biallelic mutations in MUTYH.
Genetic testing for hereditary colorectal cancer syndromes should be offered to patients with: colorectal cancer diagnosed before age 50, personal or family history of multiple colorectal cancers or Lynch-associated cancers, presence of ≥10 cumulative colorectal adenomas, or tumor that tests dMMR/MSI-H at any age. Genetic counseling before and after testing helps patients and their families understand results and implications for relatives.
Key Points About Colon Cancer
Colon cancer is a common but largely preventable and treatable malignancy when detected early through appropriate screening. Most colon cancers arise from adenomatous polyps over a period of 10 to 15 years — a slow progression that creates a wide window of opportunity for prevention through colonoscopy-based polypectomy. The five-year relative survival for localized colon cancer exceeds 90%; for metastatic disease, it drops to approximately 14%, underscoring why early detection through screening is so important. The molecular heterogeneity of colon cancer — with actionable alterations in RAS, BRAF, HER2, and MMR status now routinely assessed — means that metastatic colon cancer treatment is increasingly personalized to the tumor’s specific biology. For anyone at or approaching screening age, the most impactful action is scheduling a colonoscopy and completing subsequent surveillance at the recommended intervals. For anyone with symptoms that could indicate colorectal cancer — blood in stool, change in bowel habits, unexplained weight loss, or anemia — the most important action is prompt evaluation rather than watchful waiting.
Colorectal cancer remains among the most preventable of all major cancers. The adenoma-to-carcinoma progression, which typically takes ten to fifteen years, creates a long window during which colonoscopy — by finding and removing precancerous polyps — can interrupt cancer development entirely. This prevention opportunity is unique to colorectal cancer among gastrointestinal malignancies; most other GI cancers do not have an identifiable, removable precursor lesion that colonoscopy can address. Completing scheduled colonoscopies at the appropriate screening and surveillance intervals, and following through on diagnostic evaluation when symptoms arise, represent two of the most impactful individual-level actions for reducing colorectal cancer incidence and mortality. The five-year survival exceeds 90 percent when colorectal cancer is caught at Stage I — a figure that underscores the value of finding it before it produces symptoms rather than after.