Numbness is one of the most universally experienced physical symptoms — familiar to anyone who has sat in one position too long or slept on an arm. In these ordinary situations, brief pressure on a nerve or its blood supply produces temporary numbness that resolves immediately with movement. But when numbness is persistent, progressive, affects both extremities symmetrically, involves color changes, or appears suddenly in a new part of the body, it can signal a problem with the circulation that requires medical evaluation. Poor blood flow to peripheral nerves — whether from narrowed arteries, venous congestion, vasospasm, or acute obstruction — produces nerve ischemia that manifests as numbness, tingling, and in severe cases, weakness and paralysis. Understanding how circulation causes numbness, what conditions are responsible, how circulatory numbness is distinguished from neurological causes, and when it constitutes an emergency helps ensure that this common symptom receives appropriate attention.
How Poor Circulation Causes Numbness
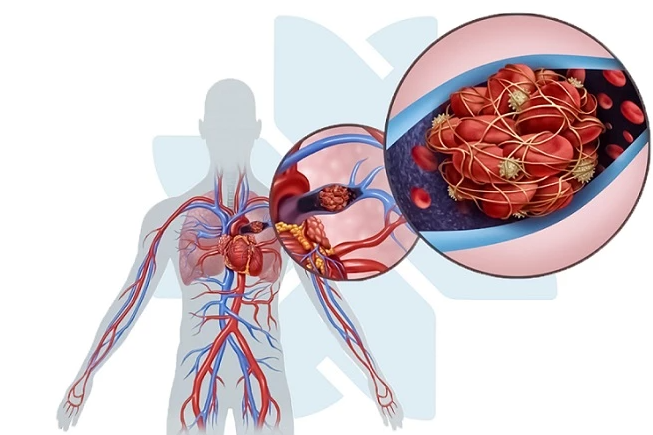
The peripheral nerves that carry sensation from the skin and limbs to the brain depend on an uninterrupted blood supply to function normally. This blood supply arrives through tiny vessels called the vasa nervorum — the blood vessels of the nerves — which run alongside and penetrate the nerve trunks to deliver oxygen and glucose to the nerve cells and their axons. When blood flow through the vasa nervorum is reduced by arterial disease, vasospasm, venous congestion, or external compression, the nerve tissue becomes ischemic: it receives insufficient oxygen to maintain normal electrical activity. The result is impaired nerve conduction, which the brain interprets as numbness, tingling (paresthesia), or in more advanced ischemia, pain and weakness.
This mechanism distinguishes circulatory numbness from mechanical nerve compression — though the two can overlap. Venous congestion contributes to numbness through a different pathway: edema — fluid accumulation in the tissue around the nerves — can mechanically compress adjacent nerve structures, reducing their function. This is one mechanism through which chronic venous insufficiency and deep vein thrombosis produce numbness and heaviness in the affected limb beyond the direct effects of venous pressure.
Circulatory Causes of Numbness
Peripheral arterial disease (PAD) is one of the most important circulatory causes of lower extremity numbness. As atherosclerotic plaques narrow the iliac, femoral, popliteal, or tibial arteries, the reduction in blood flow reduces the oxygen delivered to the muscles, skin, and nerves of the leg and foot. Numbness in the feet, along with coldness and pallor, is a common feature of significant PAD. In typical presentations, numbness accompanies claudication — cramping pain in the calf or thigh with walking. In atypical presentations — particularly in diabetic patients with coexistent peripheral neuropathy — numbness may be the predominant symptom without prominent claudication pain. Critical limb ischemia produces severe and persistent numbness, rest pain, and skin breakdown, representing an urgent vascular situation requiring revascularization.
Raynaud’s phenomenon produces transient digital numbness during vasospastic episodes. When the digital arteries go into spasm in response to cold or emotional stress, blood flow to the fingers is abruptly reduced, producing the characteristic pallor (white phase) followed by cyanosis (blue phase). During these phases, the fingers are not only cold and discolored but also numb — the numbness reflecting transient ischemia of the digital nerves. The numbness resolves with the reactive hyperemia (red phase) as vasospasm releases and blood returns.
Deep vein thrombosis (DVT) causes numbness through venous congestion and edema. The obstructed venous outflow elevates venous pressure throughout the affected limb, producing swelling, warmth, and pain, and the resulting edema can compress adjacent sensory nerves, producing numbness. DVT-related numbness is typically unilateral, associated with calf pain, swelling, and redness, and occurs in the context of risk factors such as recent immobility, surgery, or malignancy. Chronic venous insufficiency produces chronic venous hypertension with edema and a sensation of heaviness and numbness in the legs that is worse with prolonged standing and better with leg elevation.
Thoracic outlet syndrome, caused by compression of the brachial plexus or subclavian artery between the first rib and clavicle, produces numbness and tingling in one arm and hand. The neurogenic form — brachial plexus compression — is the most common and produces numbness and tingling often worsened by overhead arm position or sustained reaching. The arterial form produces coldness and numbness of the entire hand, sometimes with color changes, and can cause distal embolization from thrombosis within the subclavian artery.
When Numbness Signals an Emergency
Acute arterial occlusion is the most serious and urgent circulatory cause of numbness. When an artery supplying a limb is suddenly blocked — by an embolus from the heart (in atrial fibrillation or following MI), thrombosis at an atherosclerotic plaque, or trauma — the result is acute limb ischemia. The classic presentation involves the six Ps: Pain (sudden severe limb pain), Pallor (pale, mottled skin), Paresthesia (numbness), Paralysis (inability to move the limb), Pulselessness (absent pulses distal to the occlusion), and Poikilothermia (cold limb). The development of numbness and especially paralysis indicates severe ischemia of the nerves and muscles that will produce irreversible damage within hours without revascularization. Any sudden onset of limb pain with numbness and absent pulses requires calling 911 immediately.
Sudden onset of numbness affecting one side of the face, one arm, or one leg — particularly when accompanied by facial drooping, arm weakness, or speech difficulty — must be treated as a stroke or transient ischemic attack (TIA) until proven otherwise. The FAST acronym (Face drooping, Arm weakness, Speech difficulty, Time to call 911) applies equally to sudden unilateral numbness as a stroke symptom. Immediate evaluation with possible thrombolysis within the treatment window can prevent permanent neurological damage.
Non-Circulatory Causes to Rule Out
The most common cause of bilateral foot numbness in adults over 50 is peripheral neuropathy — damage to peripheral nerves from metabolic, toxic, or nutritional causes rather than from ischemia. Diabetic peripheral neuropathy, which affects up to 50 percent of patients with long-standing diabetes, produces a classic stocking-and-glove distribution of numbness, tingling, and burning pain that begins in the toes and feet and gradually ascends. It is a direct result of the metabolic effects of hyperglycemia on nerve cells and their myelin sheaths, not a circulatory problem, though it can coexist with PAD in the same patient.
Vitamin B12 deficiency produces ascending numbness, loss of proprioception, and gait instability. Carpal tunnel syndrome — compression of the median nerve at the wrist — produces numbness and tingling in the thumb, index, middle, and part of the ring finger, classically worse at night and during activities that flex the wrist. These non-circulatory causes respond to specific treatments (glycemic control, B12 replacement, wrist splints and surgical release) that differ entirely from vascular interventions.
Key Features That Help Identify the Cause
Several features reliably distinguish circulatory from non-circulatory numbness. Positional or transient numbness that resolves immediately with movement is almost always benign mechanical nerve compression. Bilateral, symmetric numbness in the feet in a stocking-and-glove distribution suggests peripheral neuropathy rather than a circulatory cause. Unilateral numbness in an entire extremity — especially with accompanying coldness, color changes, or absent pulses — points to a vascular cause.
The accompanying features are diagnostically important. Numbness with the triphasic color changes (white-blue-red) of Raynaud’s, triggered by cold or stress, is virtually diagnostic of Raynaud’s phenomenon. Numbness with exertional leg pain (claudication) suggests PAD. Numbness with unilateral leg swelling, warmth, and calf pain suggests DVT. Numbness with overhead arm activity in a young person suggests thoracic outlet syndrome. Nighttime hand numbness relieved by shaking the wrist suggests carpal tunnel syndrome rather than a circulatory cause.
Evaluation and Treatment
When a circulatory cause of numbness is suspected, evaluation begins with pulse assessment — palpating the radial, femoral, popliteal, dorsalis pedis, and posterior tibial pulses — which immediately identifies absent or diminished pulses indicating arterial disease. The ankle-brachial index (ABI) is the first-line screening test for PAD. For suspected DVT, duplex ultrasound of the lower extremity veins is the diagnostic standard. Nerve conduction studies and electromyography (EMG) distinguish peripheral neuropathy from circulatory numbness. Blood tests — fasting glucose, HbA1c, vitamin B12, and TSH — identify metabolic and nutritional causes of peripheral neuropathy.
Treatment of circulatory numbness depends on the underlying vascular cause. For PAD: smoking cessation, statin therapy, antiplatelet therapy, supervised exercise rehabilitation, and revascularization for limb-threatening ischemia. For Raynaud’s: calcium channel blockers (nifedipine, amlodipine) and behavioral trigger avoidance. For DVT: therapeutic anticoagulation with a direct oral anticoagulant or warfarin to prevent propagation and embolization. For venous insufficiency: graduated compression stockings and leg elevation. For thoracic outlet syndrome: physical therapy for the neurogenic form, with surgery reserved for severe or refractory cases. For acute arterial occlusion: emergency catheter-directed thrombolysis or surgical thromboembolectomy within six hours of symptom onset is essential for limb salvage.
Frequently Asked Questions
How do I know if my foot numbness is from poor circulation or nerve damage?
Circulatory numbness from PAD is usually accompanied by coldness, pallor, or absent pulses in the foot, and may be associated with cramping leg pain when walking. Neuropathic numbness from diabetes or B12 deficiency typically affects both feet equally in a stocking distribution, is not accompanied by pulse changes or color changes, and may be accompanied by burning or pins-and-needles sensations. In clinical practice, the two conditions frequently coexist in diabetic patients, where both should be evaluated. An ankle-brachial index (ABI) measures circulation; nerve conduction studies measure nerve function — together they provide a complete picture.
Can poor circulation cause permanent numbness?
Yes, if left untreated. Prolonged nerve ischemia from severe PAD or critical limb ischemia can cause permanent nerve damage that does not fully resolve even after blood flow is restored. This is one reason why prompt treatment of significant circulatory numbness is important. In contrast, mild transient numbness from Raynaud’s episodes or early venous insufficiency does not typically cause permanent nerve damage because blood flow is only intermittently reduced, not continuously absent. The duration and severity of ischemia determines whether nerve damage is reversible or permanent.
Should I be worried if my arm goes numb when I sleep on it?
Not usually. Positional arm numbness that occurs when pressure is placed on a nerve or its blood supply — such as sleeping on an arm or crossing the legs for extended periods — is benign mechanical compression and resolves within seconds to minutes of changing position. The concern arises when numbness persists after repositioning, occurs without an obvious positional cause, is accompanied by weakness, involves a limb that looks pale or feels cold, or occurs suddenly in a new distribution. If arm numbness is also waking you from sleep specifically in the hand (especially the thumb and first two fingers), carpal tunnel syndrome is a common cause worth evaluating.
Is sudden hand numbness always an emergency?
Sudden hand numbness is not always an emergency, but it must be taken seriously until a benign cause is established. If the numbness is on both hands, associated with tingling around the mouth, and occurred during a period of rapid or anxious breathing, hyperventilation-induced numbness is a likely cause — not a vascular emergency. If the numbness is on one hand or one side of the body, came on abruptly without a positional explanation, and is accompanied by weakness, facial drooping, or speech difficulty, it must be treated as a stroke or TIA and 911 called immediately. If one hand is suddenly cold, pale, and pulseless with pain, acute arterial occlusion requires emergency vascular care.
For context on related circulation symptoms, see our article on cold hands and feet circulation causes. For information on leg swelling that often accompanies circulatory numbness, see leg swelling and heart health. For cardiovascular reference values relevant to circulatory assessment, see heart health numbers every adult should know.
The American Heart Association provides information on peripheral artery disease as a common circulatory cause of leg numbness. The National Heart, Lung, and Blood Institute explains PAD symptoms, risk factors, and diagnosis. The CDC provides population data on PAD prevalence and its relationship to cardiovascular risk.
Numbness is a symptom that ranges from trivially common to life-threatening depending on its cause. The transient numbness of a briefly compressed nerve is benign; the sudden numbness of an acutely occluded artery or a stroke is an emergency requiring immediate intervention. Between these extremes lies a broad spectrum of circulatory causes — PAD, Raynaud’s, DVT, venous insufficiency, thoracic outlet syndrome — that are diagnosable with systematic evaluation and treatable with targeted interventions. Persistent, progressive, or sudden numbness — particularly when accompanied by coldness, color changes, weakness, or loss of pulses — deserves prompt medical evaluation rather than watchful waiting.
Numbness in Specific Populations and Contexts
Diabetic patients deserve particular attention in any discussion of numbness and circulation because they are vulnerable to both peripheral neuropathy and peripheral arterial disease simultaneously — a combination that is clinically dangerous. Diabetic peripheral neuropathy eliminates the protective pain sensation that would normally alert a patient to tissue injury, pressure ulcers, or worsening ischemia. When this insensate neuropathy coexists with PAD-related reduced blood flow, the result is a foot that cannot feel pain and cannot heal wounds effectively — the pathological substrate for the diabetic foot complications that lead to amputation. Patients with diabetes who have foot numbness should have regular comprehensive foot examinations including ABI measurement, monofilament sensory testing, and examination of pulses, skin integrity, and nail condition.
Older adults are disproportionately affected by both PAD and peripheral neuropathy, and their numbness is frequently attributed to “normal aging” rather than investigated systematically. While some reduction in vibratory sense and fine touch occurs with age, significant bilateral foot numbness, unilateral limb numbness, or numbness accompanied by weakness or other neurological symptoms should not be dismissed as aging changes. The prevalence of PAD increases sharply after age 65, and undetected PAD in older adults contributes to functional decline, falls from impaired proprioception and balance, and ultimately limb-threatening ischemia that might have been prevented with earlier intervention.
Athletes and physically active individuals can develop numbness from a different set of circulatory causes. Effort-induced compartment syndrome — increased pressure within the fascial compartments of the lower leg during sustained exercise — compresses both the muscles and the nerves within the compartment, producing numbness and weakness during exertion that resolves with rest. Popliteal artery entrapment syndrome, in which an abnormally positioned or hypertrophied medial head of the gastrocnemius muscle compresses the popliteal artery during foot plantar flexion, causes exertional foot numbness and claudication-like symptoms in young, active individuals who would not otherwise be expected to have PAD. These exercise-related vascular syndromes should be considered in physically active patients with exertional lower extremity numbness who lack traditional cardiovascular risk factors.
The Relationship Between Circulation and Nerve Health Over Time
The relationship between circulatory health and peripheral nerve health is bidirectional and long-term. Chronic mild reduction in peripheral blood flow — from early PAD or small vessel disease — can impair the metabolic function of peripheral nerves before causing frank ischemic symptoms. This vascular contribution to peripheral neuropathy may explain why some patients with peripheral neuropathy lack the typical risk factors for purely metabolic neuropathy (no diabetes, normal B12, no alcohol use) but have evidence of subclinical vascular disease on more detailed evaluation.
Conversely, peripheral neuropathy can impair the regulation of peripheral blood flow through its effects on autonomic nerve fibers that control vasomotion. Autonomic neuropathy — a component of diabetic neuropathy — impairs the normal vasoconstriction that redistributes blood away from the skin in response to postural changes, producing postural hypotension. It also impairs the normal vasodilatory response to skin injury that promotes healing, contributing to the impaired wound healing of diabetic feet beyond the direct effects of hyperglycemia and ischemia. This interplay between nerve function and vascular regulation underscores the importance of treating both conditions simultaneously in patients who have both peripheral neuropathy and vascular disease.
Protecting nerve health through circulatory optimization is a key goal in the management of PAD and other vascular conditions. Early revascularization of significant arterial disease — before permanent nerve damage occurs — can reverse circulatory numbness and prevent the progression to irreversible neuropathy. Similarly, aggressive cardiovascular risk factor modification that slows atherosclerosis progression protects both the limb arteries and the nerves they supply. The shared substrate of vascular risk — smoking, diabetes, hypertension, hyperlipidemia — drives both PAD and the small vessel disease that contributes to peripheral neuropathy, making comprehensive risk factor management the foundation of long-term nerve and circulatory health.
Vasculitis and Rare Vascular Causes of Numbness
Vasculitis — inflammation of blood vessel walls — can cause numbness through ischemia of the small vessels supplying peripheral nerves (vasa nervorum), producing a clinical pattern called mononeuritis multiplex: sudden, painful numbness in the distribution of a specific peripheral nerve, followed by additional nerve involvement in a stepwise, asymmetric pattern that distinguishes it from the symmetric polyneuropathy of diabetes or B12 deficiency. Vasculitis-associated mononeuritis multiplex occurs in the context of systemic conditions including polyarteritis nodosa, granulomatosis with polyangiitis (formerly Wegener’s), ANCA-associated vasculitis, cryoglobulinemia (associated with hepatitis C), and rheumatoid vasculitis. The sudden, painful onset and asymmetric pattern should distinguish it from chronic metabolic neuropathy.
Cold agglutinin disease is a rare cause of circulatory numbness in which an IgM antibody causes red blood cells to agglutinate when exposed to cold temperatures. In the small vessels of the distal extremities, where blood cools as it approaches the skin surface, this agglutination can produce transient microvascular occlusion, manifesting as Raynaud’s-like color changes, numbness, and livedo reticularis (a net-like purplish skin discoloration). Cold agglutinin disease may be primary (idiopathic, often in older adults) or secondary to lymphoma, mycoplasma pneumonia, or Epstein-Barr virus infection. Cryoglobulinemia — precipitation of abnormal immunoglobulins in cold temperatures within small vessels — produces similar findings with the addition of purpura (small purple spots under the skin from leakage of blood through damaged vessel walls).
Subclavian steal syndrome occurs when significant stenosis of the subclavian artery proximal to the origin of the vertebral artery causes retrograde flow in the vertebral artery to supply the arm at the expense of the posterior brain circulation. Patients experience symptoms of posterior cerebral ischemia (dizziness, visual disturbance, drop attacks) triggered by arm exercise, along with arm fatigue and occasionally numbness in the arm. It is typically discovered during evaluation of vertebrobasilar symptoms and is confirmed by demonstrating a significant blood pressure difference between the two arms (more than 15-20 mmHg) and retrograde vertebral flow on duplex ultrasound. Subclavian artery revascularization (stenting or surgical bypass) resolves the steal physiology and symptoms.
Raynaud’s phenomenon associated with connective tissue disease — particularly systemic sclerosis — can cause persistent numbness of the fingers between episodes as the underlying small vessel structural damage progresses. Unlike primary Raynaud’s, where normal vessel function is restored between episodes, secondary Raynaud’s in scleroderma is associated with progressive loss of capillary density and fixed structural narrowing of digital arteries. This means that between acute vasospastic episodes, baseline blood flow to the fingers remains reduced, producing persistent baseline numbness that reflects continuous mild digital nerve ischemia. Nailfold capillaroscopy — microscopic examination of the capillaries at the nailfold — reveals the characteristic pattern of giant capillaries, hemorrhages, and avascular areas that distinguish scleroderma-related from primary Raynaud’s and should be performed in all patients with suspected secondary Raynaud’s.