MRI for cancer is one of the most powerful diagnostic tools in oncology — offering detailed images of soft tissue, brain, and organs without any ionizing radiation. Unlike CT, which uses X-rays, MRI uses a strong magnetic field and radiofrequency pulses to create contrast based on how water molecules behave in different tissues. This makes MRI uniquely suited for imaging the brain, spinal cord, prostate, rectum, breast, liver, and soft tissue tumors — areas where CT falls short.
MRI for cancer serves four main functions: detecting tumors that CT misses (particularly in the brain and posterior fossa), locally staging cancers where surgical planning depends on precise soft tissue margins (prostate, rectum), providing high-risk patients with radiation-free annual screening (breast, Li-Fraumeni syndrome), and monitoring treatment response where signal — not just size — reflects biology (rectal cancer complete response, brain pseudoprogression). For a complete overview of all imaging modalities used in oncology, see our guide to imaging tests for cancer.
How MRI Works for Cancer Detection
MRI places the patient inside a strong magnetic field (1.5 or 3 Tesla), which aligns hydrogen protons in water molecules throughout the body. When a radiofrequency pulse is applied, the protons are knocked out of alignment; as they relax back, they emit signals that vary by tissue type — producing natural contrast between fat, water, muscle, tumor, and blood vessels. No radiation is involved.
The main MRI sequences used in cancer imaging:
- T2-weighted: Water is bright. Ideal for soft tissue anatomy — the prostate’s zonal anatomy, rectal wall layers, edema surrounding brain tumors, liver lesions. Most cancer MRI protocols begin here.
- Diffusion-weighted imaging (DWI): Detects restriction of water movement. Highly cellular tumors — with tightly packed cells — restrict water diffusion and appear bright on DWI and dark on ADC (apparent diffusion coefficient) maps. The dominant sequence in prostate MRI; improves liver lesion detection.
- Dynamic contrast-enhanced (DCE) MRI: Rapid T1 sequence before, during, and after IV gadolinium — captures tumor blood supply kinetics. Key for breast MRI to detect cancer’s abnormal vascular enhancement pattern.
- T1 post-contrast: Gadolinium crosses the blood-brain barrier only where it is disrupted — by high-grade tumors or metastases — producing bright enhancement. Critical for brain tumor grading and metastasis detection.
Because MRI produces no ionizing radiation, it is safe for repeated imaging and for patients who need long-term surveillance — BRCA1/2 carriers, patients on active surveillance for low-risk prostate cancer, and children.
When Is MRI Better Than CT for Cancer?
Both CT and MRI are essential in oncology. The choice depends on the cancer type, clinical question, and what anatomy needs to be visualized.
| Cancer / Situation | Why MRI Is Preferred |
|---|---|
| Brain tumors (glioma, metastases, meningioma) | Far superior soft tissue contrast; detects posterior fossa lesions CT misses; essential for glioma grading and surgical planning |
| Prostate cancer (local staging, biopsy guidance) | mpMRI with PI-RADS scoring; targets biopsy to highest-risk zones; reduces unnecessary biopsies |
| Rectal cancer local staging | Shows depth of wall invasion (T stage), CRM distance, EMVI — critical for surgical planning and neoadjuvant therapy decisions |
| Breast cancer (high-risk screening; extent at diagnosis) | Detects multifocal disease and lobular carcinoma extent that mammography misses |
| Liver cancer (HCC in cirrhosis) | Hepatobiliary contrast agents improve HCC detection sensitivity to ~90% |
| Soft tissue sarcoma | Superior to CT for muscle and fascial invasion assessment; determines resectability |
| Bone marrow (myeloma, marrow infiltration) | Whole-body MRI far more sensitive than bone scan or CT for marrow disease |
| Spinal cord / leptomeninges | Only modality that reliably images spinal cord structure and leptomeningeal disease |
mpMRI for Prostate Cancer — What PI-RADS Means
Multiparametric MRI (mpMRI) of the prostate combines T2-weighted, diffusion-weighted, and dynamic contrast-enhanced sequences to characterize suspicious lesions before biopsy. Major urology guidelines now recommend mpMRI before any prostate biopsy in biopsy-naive men.
Results are reported using PI-RADS (Prostate Imaging Reporting and Data System) v2.1 — a standardized 1–5 scale developed by the American College of Radiology:
| PI-RADS | Description | Risk of Clinically Significant PCa |
|---|---|---|
| 1 | Highly unlikely malignant | Very low — no targeted biopsy typically |
| 2 | Unlikely malignant | Low — monitor with PSA; no targeted biopsy |
| 3 | Equivocal | ~20–30% — clinical judgment; often targeted biopsy |
| 4 | Likely malignant | ~60–80% — biopsy strongly recommended |
| 5 | Highly likely malignant | >90% — biopsy and clinical action warranted |
The PRECISION trial (NEJM 2018, n=500 men) found MRI-targeted biopsy detected clinically significant prostate cancer in 38% of men vs. 26% with standard systematic 12-core biopsy — while detecting 9% fewer clinically insignificant cancers. For PI-RADS 4–5 lesions, the biopsy is typically an MRI-TRUS fusion biopsy — MRI images overlaid onto real-time ultrasound to guide the needle precisely to the suspicious lesion. Men on active surveillance use serial mpMRI every 1–2 years to detect upgrading earlier than PSA alone. See the ACR PI-RADS page for the full reporting system.
Breast MRI — Who Needs It and What It Shows
Breast MRI is not routine screening for average-risk women. It is recommended for specific high-risk populations where its superior sensitivity justifies the higher cost, false-positive rate, and gadolinium requirement.
Who should get breast MRI screening (per ACS and NCCN):
- Known BRCA1 or BRCA2 gene mutation
- First-degree relative of a BRCA carrier who has not been tested
- Lifetime breast cancer risk >20% by risk models (Tyrer-Cuzick, BRCAPRO)
- Prior chest radiation at age 10–30 (e.g., Hodgkin lymphoma treatment)
- Li-Fraumeni (TP53), Cowden (PTEN), or Bannayan-Riley-Ruvalcaba syndromes
Annual breast MRI + annual mammography is the standard of care for these women — typically starting at age 25–30 for BRCA1 carriers. See the American Cancer Society breast MRI guidance for the full eligibility criteria.
What breast MRI finds that mammography misses:
- Sensitivity in high-risk women: 71–100% for MRI vs. 39–59% for mammography
- Invasive lobular carcinoma (ILC) — underestimated by mammography; MRI shows full extent
- Multifocal/multicentric disease at diagnosis — changes surgical planning in ~20–30% of cases
- Occult primary breast cancer presenting as axillary adenopathy with no visible primary on mammogram
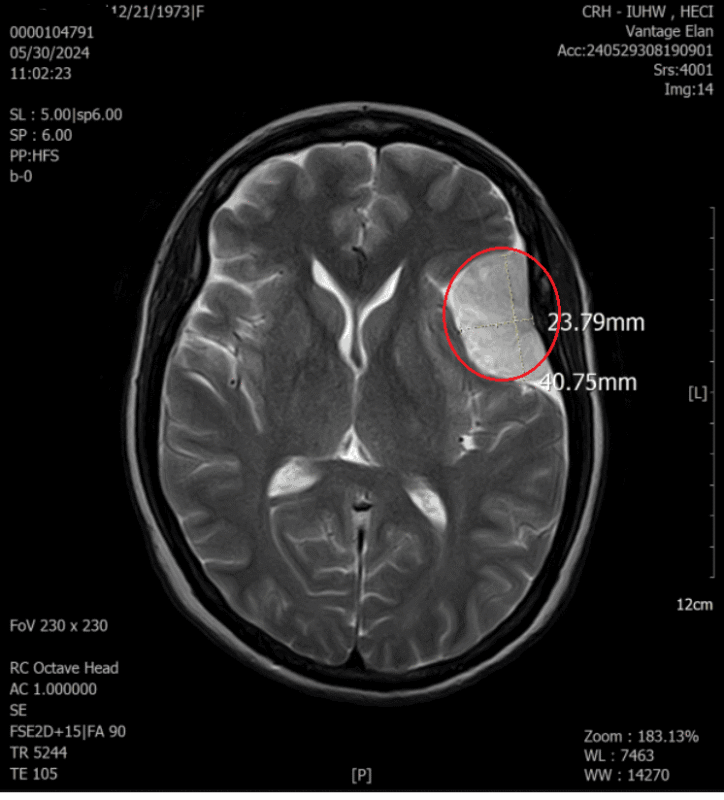
Brain Tumor MRI
For any suspected brain tumor, MRI is the imaging modality of choice. CT can detect large brain masses but misses small tumors in the posterior fossa (cerebellum, brainstem), cannot adequately characterize glioma extent, and does not show early leptomeningeal disease.
Standard brain tumor MRI protocol:
- T1 pre-contrast — anatomy, hemorrhage identification, fat
- T2/FLAIR — tumor infiltration beyond the visible mass, surrounding edema, white matter involvement
- DWI — high-grade tumor typically shows restricted diffusion; distinguishes abscess (ring-enhancing but restricted centrally) from tumor
- T1 post-gadolinium — enhancement = blood-brain barrier disruption = high-grade tumor or metastasis. Ring enhancement with central necrosis = characteristic glioblastoma (GBM) pattern.
Glioma grading (WHO 2021): Low-grade glioma (Grade 2) — T2/FLAIR bright, non-enhancing, associated with IDH mutation (better prognosis). High-grade GBM (Grade 4) — ring-enhancing with central necrosis, IDH-wildtype, worst prognosis.
Gadolinium-enhanced MRI detects brain metastases far more sensitively than CT — particularly lesions <1 cm and posterior fossa metastases. Brain staging MRI is standard at diagnosis for lung cancer, breast cancer, and melanoma. Pseudoprogression after radiation or checkpoint inhibitor therapy can mimic tumor growth on MRI — perfusion MRI helps distinguish true progression from treatment effect in up to 10% of immunotherapy patients who experience this phenomenon.
Rectal Cancer MRI — Why It Changes Surgery
MRI pelvis is the standard of care for rectal cancer local staging — recommended by NCCN, ESMO, and ASCO — because it directly answers the surgical question: can this tumor be completely removed with clear margins?
Key MRI measurements for rectal cancer:
- T stage: MRI evaluates depth of tumor invasion through rectal wall layers — T1 (submucosa) through T4 (adjacent organs)
- Circumferential resection margin (CRM): Distance from tumor edge to mesorectal fascia. CRM <1 mm = threatened margin = high local recurrence risk → indication for neoadjuvant chemoradiation before surgery
- EMVI (extramural vascular invasion): Tumor extending into perirectal vessels — predicts metastatic risk; visible on T2-weighted images
- mrTRG (MRI tumor regression grade): After chemoradiation, assesses residual viable tumor. mrTRG 1–2 = complete/near-complete response → these patients may be candidates for watch-and-wait, avoiding surgery and permanent colostomy
What to Expect During an MRI for Cancer
Before the MRI
- Metal screening: Pacemakers, cochlear implants, certain aneurysm clips, retained metal fragments may be contraindicated — always complete the screening questionnaire honestly. Modern pacemakers are increasingly MRI-conditional.
- Fasting: Not required for brain, prostate, or extremity MRI; some abdominal protocols require 4–6 hour fast to reduce bowel peristalsis artifact
- Gadolinium screening: eGFR check if contrast is planned, particularly for patients with kidney disease
During the MRI
- Lie flat on a narrow table that slides into the scanner bore (cylinder ~60–70 cm diameter)
- Loud rhythmic knocking and banging sounds — this is normal gradient coil switching; earplugs and headphones are provided
- Call button in hand at all times; intercom to speak with the technologist
- Breath-hold instructions for abdominal/pelvic imaging sequences
- IV gadolinium injection (if needed): minimal sensation; rare allergic reactions (<0.1%)
- Duration: 30–90 minutes depending on body part and protocol
Frequently Asked Questions
What can an MRI detect in cancer?
MRI can detect primary tumors in the brain, spinal cord, prostate, rectum, breast, liver, and soft tissues — with superior detail compared to CT for these locations. It can grade brain tumors (low vs. high grade), determine whether prostate cancer has spread beyond the gland, show whether rectal cancer threatens the surgical margin, and detect cancer in dense breast tissue. According to the National Cancer Institute, MRI can detect abnormalities as small as a few millimeters in appropriate tissue contexts. MRI does not image lung tumors or calcification well. A negative MRI does not rule out cancer — tissue biopsy remains the gold standard. For what happens after a suspicious MRI finding, see our biopsy for cancer guide.
Is MRI better than CT for cancer?
It depends on the cancer type and clinical question. MRI is superior for brain, prostate, rectal, breast, liver, bone marrow, and soft tissue tumor evaluation. CT is superior for lung cancer staging, emergency settings, detecting calcification, and most whole-body staging protocols due to speed and availability. Most oncology workups use CT first for staging, with MRI added when more detailed soft tissue information is needed. The two modalities complement rather than replace each other — and most solid cancer diagnoses benefit from both at different stages of workup and treatment.
Do you need contrast for a cancer MRI?
Many cancer MRI protocols use gadolinium contrast to detect blood-brain barrier breakdown (brain tumors, metastases), tumor vascularity (breast MRI DCE), and liver lesion characterization. Some protocols — including prostate mpMRI (in some centers) and bone marrow assessment — provide useful information without contrast. Whether you need contrast depends on what organ is being imaged and what question is being answered. If you have kidney problems (eGFR <30), discuss this with your radiologist — macrocyclic gadolinium agents (e.g., gadobutrol, gadoteridol) are considered lower risk than older linear agents per ACR 2023 contrast guidelines.
How long does an MRI for cancer take?
MRI takes 30–90 minutes depending on the body part and protocol. A brain MRI with contrast typically takes 30–45 minutes. Prostate mpMRI takes 45–60 minutes. Breast MRI takes 30–60 minutes. Whole-body or multi-region MRI can take 60–90 minutes. This is significantly longer than CT, which takes less than 5 minutes for a chest-abdomen-pelvis scan. If you need to lie still for this long and have concerns about claustrophobia or discomfort, discuss options with your provider before the appointment.
Who should get breast MRI for cancer screening?
Breast MRI screening is recommended for women with BRCA1 or BRCA2 mutations, first-degree relatives of confirmed BRCA carriers, lifetime breast cancer risk >20% by risk models (Tyrer-Cuzick, BRCAPRO), and those with a history of chest radiation between ages 10–30. The American Cancer Society recommends annual breast MRI alongside annual mammography for these groups, starting at age 25–30 for BRCA1 carriers. Women with average risk do not need breast MRI — the false-positive rate is too high and the marginal benefit over mammography too small. If you are unsure of your risk category, a risk assessment at your next cancer checkup can clarify eligibility.
Can MRI miss cancer?
Yes. MRI can miss small tumors (generally <5 mm), cancers in locations where MRI sensitivity is lower (lung, calcification-only DCIS in breast), and cancers without enough signal difference from surrounding tissue. A normal MRI does not rule out cancer. The clinical context — symptoms, blood tests, prior imaging — determines whether additional workup is needed. If you are experiencing concerning symptoms, our cancer symptoms checklist can help you organize what to discuss with a provider before or after imaging.
Sources & Further Reading
- NCI — MRI and Cancer Fact Sheet
- ACR — PI-RADS v2.1 (Prostate MRI Reporting System)
- American Cancer Society — Breast MRI Screening Guidance
- Ahmed HU et al. — PRECISION Trial (MRI-targeted vs. standard prostate biopsy), NEJM 2018
- WHO Classification of CNS Tumours 2021
- ACR Manual on Contrast Media 2023 (gadolinium and NSF)
- MERCURY Study — MRI and Rectal Cancer European Equivalence Study (CRM prediction)
- American Cancer Society Breast Cancer Screening Guidelines 2017
This article is for educational purposes only and does not constitute medical advice. MRI recommendations, preparation requirements, and results should be discussed with your treating physician or radiologist.