
Radiation therapy is the use of high-energy ionizing radiation to damage the DNA inside cancer cells, preventing them from dividing and causing them to die. It is one of the most important and widely used treatments in oncology — more than half of all cancer patients receive radiation therapy at some point during their care, either as a primary treatment, in combination with surgery or chemotherapy, or to relieve symptoms.
Unlike chemotherapy, which circulates throughout the bloodstream to reach cancer cells anywhere in the body, radiation therapy is a local and regional treatment: it targets a specific area, making it particularly effective for tumors confined to one site, for treating tissue where cancer has been surgically removed, or for ablating a defined number of metastatic sites. This article covers how radiation therapy works, the different delivery techniques available today, how treatment is planned, and how side effects are prevented and managed. For an overview of how radiation fits within all treatment options, see the cancer treatment options guide.
How Radiation Therapy Works — Radiobiology
Radiation therapy deposits energy in tissue through ionization — removing electrons from atoms. This process creates reactive oxygen species (primarily hydroxyl radicals from water molecules) that cause double-strand DNA breaks, the most lethal form of DNA damage. Single-strand breaks are repaired efficiently by both normal and cancer cells; double-strand breaks are far harder to fix.
Cancer cells are particularly vulnerable because they divide more rapidly (placing them more often in vulnerable cell cycle phases) and because they typically have defective DNA repair pathways — the same mutations that drive cancer growth impair their ability to recover from radiation. Normal cells with intact repair mechanisms recover between treatment sessions, which is why radiation is almost always given in multiple fractions rather than as a single large dose.
The 4 Rs of Radiobiology
- Repair: Normal cells repair sublethal radiation damage between fractions more effectively than cancer cells — fractionation exploits this differential
- Repopulation: Both tumor and normal cells divide between fractions; overall treatment time must balance against tumor repopulation
- Redistribution: Radiation kills cells in radiosensitive phases (G2/M); surviving cells redistribute to more sensitive phases before the next fraction
- Reoxygenation: Hypoxic tumor cells are up to 3× more radioresistant than oxygenated cells; after radiation kills well-oxygenated cells, previously hypoxic cells reoxygenate — increasing the effect of subsequent fractions
Fractionation and the α/β Ratio
The α/β ratio describes how sensitive a tissue is to fraction size. Tumors with a low α/β ratio (prostate ~1.5–2 Gy; breast ~3–4 Gy) are more sensitive to larger fractions — making them ideal candidates for hypofractionation (fewer, larger fractions), which delivers equivalent or superior tumor control with equivalent or reduced late toxicity. Tumors with a high α/β ratio (~10 Gy; head and neck carcinomas) are relatively insensitive to fraction size, and conventional fractionation (1.8–2 Gy/fraction) is appropriate.
This radiobiology is why modern prostate cancer treatment now uses 5 SBRT fractions rather than 39–40 conventional fractions, and why whole breast irradiation is routinely completed in 15 fractions rather than 25.
Types of Radiation Therapy
IMRT / VMAT
Computer-optimized external beam; modulates thousands of beamlets to sculpt dose around the tumor. Standard for H&N, prostate, gynecologic, lung, and rectal cancers. VMAT delivers same dose in 3–10 min via rotating arc.
SBRT / SABR
3–5 high-dose fractions with stereotactic precision. 97.6% tumor control for early lung cancer (RTOG 0236); non-inferior for prostate (PACE-B); 5-yr OS 42.3% vs. 17.7% for oligomets (SABR-COMET).
Stereotactic Radiosurgery (SRS)
Single-fraction intracranial treatment. Gamma Knife (brain mets, AVM); CyberKnife. NCCTG N0574 (JAMA 2016): SRS alone vs. SRS + WBRT — no OS difference; WBRT worsens cognition. SRS alone now preferred for 1–3 brain mets.
Proton Therapy
Bragg peak: maximum dose at target depth, near-zero beyond. Reduces dose to distal normal tissue. Established benefit: pediatric tumors, base of skull, uveal melanoma. Not uniformly superior to IMRT for adult solid tumors.
Brachytherapy
Internal radioactive sources. LDR: permanent prostate seeds (I-125/Pd-103). HDR: temporary Ir-192 catheter for cervical cancer boost, breast APBI, endometrial. GEC-ESTRO: brachytherapy boost superior to EBRT-only for cervical cancer.
IGRT + Adaptive (MR-Linac)
Daily cone beam CT corrects for organ motion and setup variation before each fraction. MR-linac (Elekta Unity, ViewRay MRIdian) enables daily MRI-guided replanning — particularly valuable for H&N and abdominal tumors.
SBRT and Oligometastatic Disease
The SABR-COMET trial (Palma DA et al., *Lancet* 2019; 5-year update 2020) randomized patients with 1–5 metastatic sites to SABR (stereotactic ablative radiotherapy) versus palliative standard of care. At 5 years, overall survival was 42.3% vs. 17.7% — a potential paradigm shift suggesting that eliminating all identifiable metastatic sites with ablative RT may be curative in some patients with limited metastatic disease. This finding has generated multiple ongoing confirmatory trials. For more on the minimally invasive approach of SBRT, see the minimally invasive cancer treatment guide.
The Brain Metastasis Standard: SRS vs. WBRT
Radiation Planning — From Simulation to Treatment
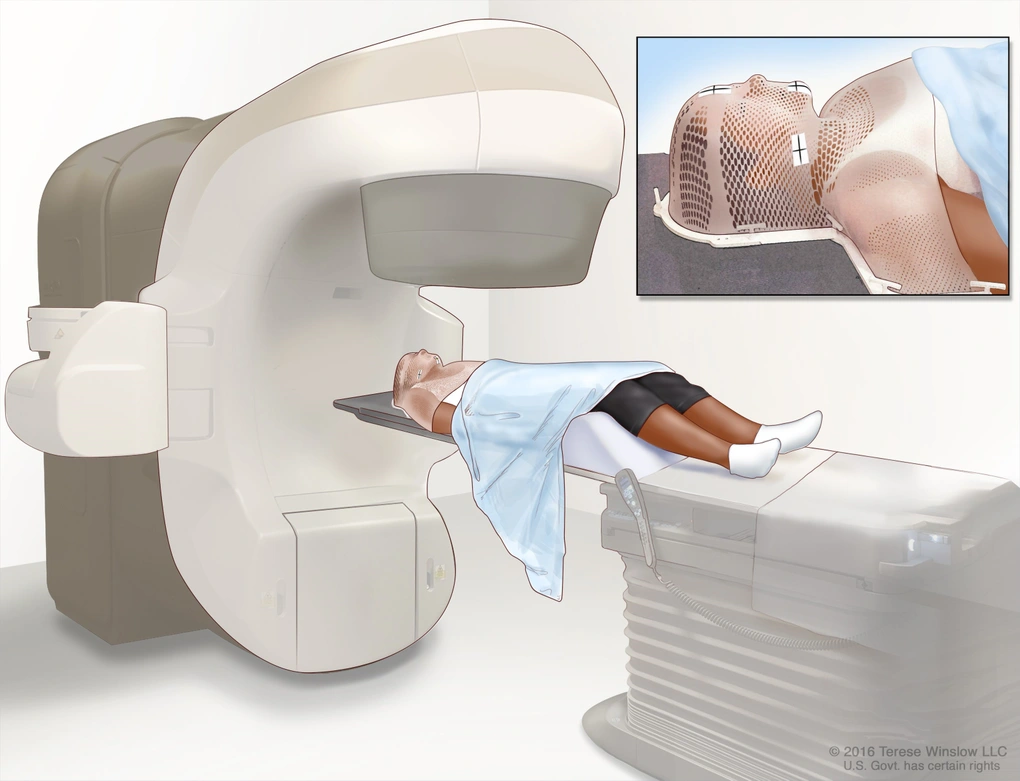
Every radiation therapy course begins with a CT simulation — a dedicated CT scan acquired with the patient in the exact treatment position, using custom immobilization devices: thermoplastic masks for head/neck and brain tumors; stereotactic body frames for SBRT; wing boards or breast boards for breast cancer. For lung and liver SBRT, 4D-CT captures tumor motion through the entire breathing cycle.
The radiation oncologist then defines treatment volumes based on the ICRU reporting framework:
- GTV (Gross Tumor Volume): Macroscopic tumor visible on imaging (CT, MRI, PET)
- CTV (Clinical Target Volume): GTV + margin for microscopic extension beyond what imaging shows
- ITV (Internal Target Volume): CTV + internal motion margin (breathing, organ filling)
- PTV (Planning Target Volume): ITV + setup uncertainty margin for daily positioning variation
The medical physicist creates the treatment plan through computer optimization — selecting beam angles, modulating intensity, and meeting dose constraints for Organs At Risk (OARs):
- Spinal cord: maximum dose ≤45–50 Gy
- Parotid glands (H&N RT): mean dose ≤26 Gy to preserve salivary function
- Lung: V20Gy ≤30% (percentage of lung receiving ≥20 Gy) to limit pneumonitis risk
- Rectum (prostate RT): V70Gy ≤20% to reduce late bleeding risk
After plan approval via Dose-Volume Histogram (DVH) review, treatment begins. Each daily visit takes 15–30 minutes total — the radiation beam is on for only 2–5 minutes. IGRT imaging confirms positioning before each fraction.
| Cancer Type | Fractionation Schedule | Key Evidence |
|---|---|---|
| Head & neck | 70 Gy / 35 fr (conventional, once daily) | RTOG 91-11: concurrent CRT superior larynx preservation |
| Breast (whole breast) | 40 Gy / 15 fr OR 26 Gy / 5 fr | START B (15 fr) 10-yr equivalent; FAST-Forward (5 fr) 5-yr non-inferior |
| Prostate (SBRT) | 36.25 Gy / 5 fr (every other day) | PACE-B: 5-yr DFS 95.8% vs. 94.8% conventional |
| Lung Stage I (SBRT) | 54 Gy / 3 fr OR 50 Gy / 5 fr | RTOG 0236: 97.6% 3-yr primary control |
| Stage III NSCLC (CRT) | 60–66 Gy concurrent with chemo | PACIFIC: 5-yr OS 42.9% with durvalumab consolidation |
| Rectal cancer (SCRT) | 25 Gy / 5 fr → systemic chemo → surgery | RAPIDO: pCR 28.4% vs. 14.3% long-course CRT |
| Cervical cancer | 45–50.4 Gy + weekly cisplatin → brachy boost | GEC-ESTRO: brachy boost superior to EBRT-only |
| Brain mets (SRS) | 15–24 Gy / 1 fr (Gamma Knife / CyberKnife) | NCCTG N0574: SRS alone preferred; WBRT worsens cognition |
Radiation Combined with Other Cancer Treatments
Radiation therapy is rarely used alone — it is most commonly integrated with chemotherapy (concurrent chemoradiation), surgery, or immunotherapy to achieve superior outcomes.
Concurrent Chemoradiation (CRT)
Cisplatin is the most widely used radiosensitizer. Its mechanism: cisplatin impairs cancer cells’ ability to repair radiation-induced DNA double-strand breaks, increasing cell kill beyond either treatment alone. Key concurrent CRT regimens:
- Head and neck SCC: Cisplatin 100 mg/m² every 3 weeks × 3 (or weekly 40 mg/m²) concurrent with 70 Gy; RTOG 91-11 showed superior larynx preservation with concurrent vs. sequential chemotherapy-then-RT or RT alone
- Cervical cancer: Weekly cisplatin 40 mg/m² concurrent with 45–50.4 Gy EBRT → intracavitary brachytherapy boost; standard of care since the 1999 NCI clinical announcement across five simultaneous trials
- Stage III unresectable NSCLC: Concurrent CRT (carboplatin + paclitaxel weekly or cisplatin + etoposide) followed by 12 months durvalumab (PACIFIC trial): 5-year OS 42.9% vs. 33.4%; median OS 47.5 months vs. 29.1 months
- Rectal cancer: Capecitabine or 5-FU concurrent with 45–50.4 Gy (long-course); or short-course 25 Gy/5 fractions followed by FOLFIRINOX → surgery (RAPIDO: pCR 28.4% vs. 14.3%)
Radiation After Surgery
Post-operative radiation reduces local recurrence by treating microscopic residual disease. Key applications:
- Breast-conserving surgery (lumpectomy): whole breast RT achieves equivalent long-term survival to mastectomy (NSABP B-06)
- Post-mastectomy RT (PMRT): standard when ≥4 lymph nodes involved, T3/T4 tumor, or positive margins
- Prostate: salvage RT to prostate bed after radical prostatectomy for biochemical failure
For more on how radiation integrates with surgical decisions and the combined modality approach, see the cancer surgery guide. See also the cancer treatment overview for how all modalities work together.
Side Effects of Radiation Therapy
Radiation side effects divide into acute effects (during treatment and up to 90 days after — reflect rapidly dividing normal cell injury; generally reversible) and late effects (more than 90 days after treatment, sometimes years later — reflect vascular damage and fibrosis; may be permanent).
Acute Side Effects by Site
- Head and neck: Oral mucositis (painful mouth sores, peaks at weeks 3–5 of a 7-week course); xerostomia (dry mouth — IMRT parotid-sparing at mean dose ≤26 Gy significantly reduces this); dysphagia (swallowing exercises during treatment preserve function); skin dermatitis
- Breast: Radiation dermatitis (redness, skin irritation, and moist desquamation in skin folds; gentle washing and aqueous creams); fatigue (graded exercise recommended by ACSM)
- Thoracic: Radiation pneumonitis (cough, dyspnea developing 1–6 months after thoracic RT; prevented by keeping V20Gy <30%; treated with prednisone 60 mg/day × 6-week taper); esophagitis during concurrent CRT
- Pelvis: Acute radiation proctitis (loose stools, urgency, rectal bleeding — resolves within weeks after RT); urinary symptoms during prostate RT (frequency, urgency, dysuria — managed with alpha-blockers)
- Brain: Cerebral edema (dexamethasone during WBRT); fatigue; hair loss only within the radiation field
Late Radiation Effects
- Xerostomia: Permanent salivary gland damage from high-dose H&N RT; IMRT parotid sparing reduces grade 2+ xerostomia significantly
- Radiation fibrosis: Progressive fibrosis in irradiated soft tissue — lung fibrosis, breast tissue changes, limb lymphedema with nodal RT
- Osteoradionecrosis: Mandibular bone necrosis after H&N RT >60 Gy — precipitated by dental extraction; require dental clearance before RT; treated with hyperbaric oxygen and surgical debridement
- Brain radiation necrosis: Occurs in ~5% after radiosurgery; bevacizumab reduces MRI changes and neurologic symptoms; advanced MRI (perfusion, spectroscopy) and PET distinguish from tumor recurrence
- Hypothyroidism: Common after neck irradiation; annual TSH monitoring recommended indefinitely
- Cardiac effects: Late coronary artery disease after left-sided breast RT and mediastinal RT (Hodgkin lymphoma); modern techniques (deep inspiration breath-hold, cardiac-sparing IMRT) minimize cardiac dose
- Secondary malignancy: Small but real risk (~0.2% at 10 years); higher concern in younger patients and larger treatment volumes
Frequently Asked Questions
- Timmerman R et al. — RTOG 0236 (SBRT for inoperable early NSCLC); JAMA 2010
- Brand DH et al. — PACE-B (prostate SBRT vs. conventional RT); Lancet Oncology 2019
- Palma DA et al. — SABR-COMET (SABR for oligometastatic disease); Lancet 2019; 5-yr update 2020
- Brown PD et al. — NCCTG N0574 (SRS vs. SRS + WBRT for brain mets); JAMA 2016
- Antonia SJ et al. / Spigel DR et al. — PACIFIC (durvalumab after CRT for Stage III NSCLC); NEJM 2017; JCO 2022
- Haviland JS et al. — START B (40 Gy/15 fr breast hypofractionation); Lancet Oncology 2013
- Murray Brunt A et al. — FAST-Forward (26 Gy/5 fr breast); Lancet 2020
- Bahadoer RR et al. — RAPIDO (short-course RT + chemotherapy for rectal cancer); Lancet Oncology 2021
- Pötter R et al. — GEC-ESTRO (brachytherapy boost for cervical cancer); Radiotherapy & Oncology 2011
- National Cancer Institute — Radiation Therapy to Treat Cancer
- ASTRO — RT Answers — Patient Information
This article is for educational purposes only and does not constitute medical advice. Discuss all radiation therapy decisions with your radiation oncology team.