Blood in stool is one of the most alarming things a person can see — and the overwhelming instinct is to attribute it to hemorrhoids. In most cases, that instinct is correct. Hemorrhoids are far more common than colorectal cancer, and they are the most common cause of rectal bleeding in adults.
The problem is that the instinct to self-diagnose, and to find a reassuring explanation, is also the most common reason colorectal cancer is diagnosed late. In published studies, 30 to 40 percent of patients eventually diagnosed with colorectal cancer had attributed their rectal bleeding to hemorrhoids for weeks or months before seeking evaluation. The hemorrhoid explanation is almost always plausible. It is also sometimes dangerously wrong.
The core issue: the symptoms of hemorrhoidal bleeding and colorectal cancer bleeding are clinically indistinguishable without evaluation. Bright red blood in the toilet, blood on toilet paper, blood coating the stool — these describe both internal hemorrhoids and left-sided colon cancer. There is no visible feature of the bleeding, seen by the patient, that reliably separates one from the other.
What Blood in Stool Can Mean — The Full List
Blood in stool has many causes, and the color and character of the blood provide useful clinical clues about where in the digestive tract it originated — though these clues are not reliable enough for patients to use as a basis for self-reassurance.
Bright red blood (from the rectum or left colon):
- Hemorrhoids — by far the most common cause of bright red rectal bleeding in adults
- Anal fissure — a tear in the anal canal; typically painful during defecation; bright red blood on toilet paper
- Rectal or sigmoid colon cancer
- Colorectal polyps (large, bleeding)
- Proctitis or colitis — IBD flares, infectious colitis, radiation-induced
- Diverticular bleeding — typically painless and can be massive; usually self-limited
Dark red or maroon blood (from the right colon or transverse colon):
- Diverticular bleeding
- Angiodysplasia (dilated blood vessels in the colon wall; more common in elderly patients)
- Right-sided colorectal cancer
Black, tarry stool (melena — from the upper gastrointestinal tract):
- Peptic ulcer (gastric or duodenal)
- Gastric cancer
- Esophageal varices
- Mallory-Weiss tear
No visible blood (occult bleeding — detected only by stool test):
- Colorectal cancer, particularly right-sided — the most important cause to screen for
- Large adenomatous polyps
- Gastric ulcer or gastric cancer
How Colon Cancer Causes Blood in Stool
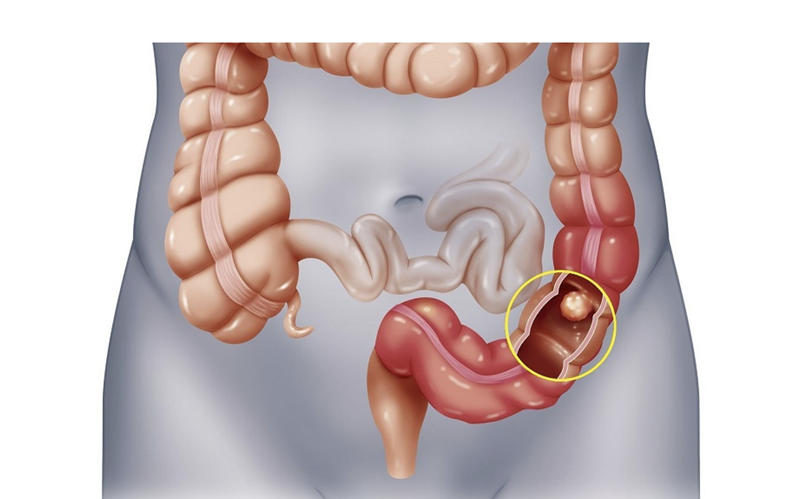
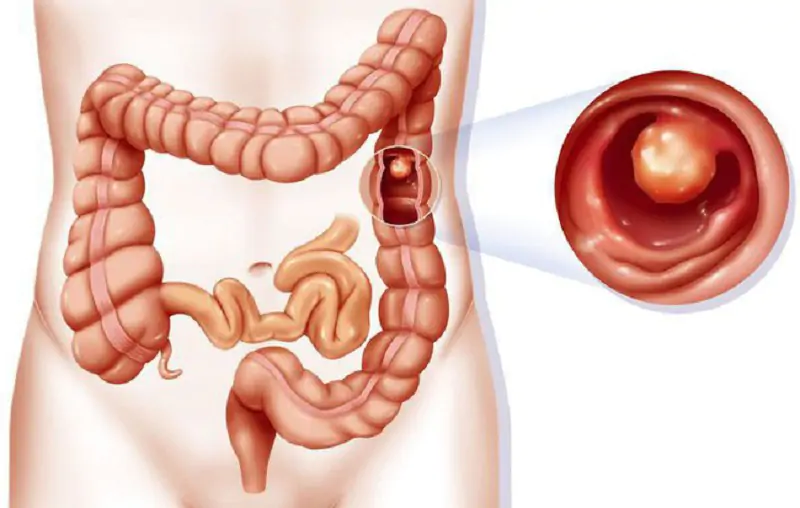
Colorectal cancers bleed because their tissue is abnormally fragile and highly vascular. As a tumor grows along the inner lining of the colon, the cancer tissue bleeds with the friction of stool passage — sometimes spontaneously. The bleeding pattern depends almost entirely on where in the colon the tumor is located.
Left colon and rectal cancer produce the visible bleeding that most people associate with colorectal cancer. The left colon — descending colon, sigmoid, and rectum — carries formed stool. When a tumor bleeds here, the blood is visible: bright red, coating the outside of the stool, appearing in the toilet bowl or on toilet paper. This bleeding is indistinguishable from internal hemorrhoidal bleeding without a direct look inside. Patients with left-sided cancer frequently have both hemorrhoids (common in the same population) and cancer — and the hemorrhoids provide a convincing explanation for bleeding that is actually coming from the tumor.
Right colon cancer produces a different presentation entirely — one that is arguably more dangerous precisely because it produces no visible blood. The right colon carries liquid stool. When a right-sided tumor bleeds, the blood disperses invisibly into that liquid content. The patient never sees blood in the toilet. There is nothing to trigger alarm.
What happens instead is the slow development of iron deficiency anemia. Weeks and months of invisible, chronic blood loss steadily deplete iron stores. The patient becomes fatigued — not ordinary tiredness, but a bone-deep heaviness that doesn’t improve with sleep. Eventually pallor, shortness of breath with light exertion, and palpitations follow. A routine blood count reveals low hemoglobin. The right colon cancer may have been bleeding invisibly for six months or more by the time the anemia is discovered.
Why Hemorrhoids Don’t Explain Away Rectal Bleeding
Blood in stool is never safe to attribute to hemorrhoids without evaluation. Colorectal cancer and internal hemorrhoids produce identical visible symptoms. The only way to confirm the source and exclude colorectal cancer is direct visualization — which means colonoscopy, not a physical exam.
Hemorrhoids are among the most common conditions in adults — approximately 75% of adults experience hemorrhoids at some point, with peak prevalence between ages 45 and 65. This is exactly the age range in which colorectal cancer incidence rises. The two conditions coexist in large numbers of patients.
When a patient with hemorrhoids notices rectal bleeding, the hemorrhoids are the most likely explanation. That probability is real. But the symptom profile of internal hemorrhoids and left-sided colorectal cancer is identical in every way that matters to the patient — bright red blood in the toilet, blood coating the stool, blood on toilet paper, occasional discomfort. There is no visible feature of the bleeding that distinguishes hemorrhoidal from cancer-associated blood.
Published studies consistently document that 30 to 40 percent of patients eventually diagnosed with colorectal cancer reported attributing their rectal bleeding to hemorrhoids before seeking evaluation. In some studies, the attribution delay was six months or longer. The most dangerous scenario is a patient who has both hemorrhoids and cancer — the hemorrhoids are real, the attribution is understandable, and the cancer grows in the background.
A physical examination does not resolve this. A doctor can perform a digital rectal examination and an anoscopy to examine the anal canal and distal rectum. These procedures identify hemorrhoids and anal fissures. They do not visualize the sigmoid colon, descending colon, ascending colon, or cecum — where colorectal cancers most commonly originate. Only a colonoscopy visualizes the entire colon.
Red Flags That Require Urgent Evaluation
Any new rectal bleeding in an adult warrants evaluation. These specific features make that evaluation more urgent:
- Age 45 or older with any new rectal bleeding: Per current USPSTF guidelines, colorectal cancer screening begins at 45; new rectal bleeding in this age group warrants colonoscopy
- Bleeding accompanied by unexplained weight loss: A combination that substantially raises the probability of malignancy
- Bleeding accompanied by significant change in bowel habits: Narrowing stools, new constipation alternating with diarrhea, or persistent diarrhea alongside bleeding
- Iron deficiency anemia in a man, or in a post-menopausal woman: The source must be identified; colonoscopy is indicated
- Family history of colorectal cancer in a first-degree relative: Raises baseline risk; any bleeding should be evaluated promptly
- Bleeding that changes in volume, frequency, or character: Hemorrhoids that have been stable for years but are now bleeding more frequently or heavily may have company in the colon
- Dark red or maroon blood rather than bright red: Suggests the source is higher in the colon than hemorrhoids can explain
- Black, tarry stool (melena): Upper gastrointestinal source; peptic ulcer and gastric cancer must be excluded urgently; requires upper endoscopy
What Evaluation Involves
Digital rectal examination: A gloved, lubricated finger examines the distal rectum and anal canal for hemorrhoids, masses, and fissures. Identifies hemorrhoids and rectal masses within reach. Does not examine the colon.
Anoscopy: A short instrument inserted into the anal canal provides direct visualization of internal hemorrhoids and fissures. Does not visualize the colon.
Colonoscopy: The gold standard for evaluating rectal bleeding in adults. A flexible scope examines the entire colon from rectum to cecum. Can identify polyps and cancers, perform biopsies, and remove lesions in the same procedure. In any adult over 45 with new rectal bleeding, colonoscopy is the appropriate evaluation.
CT colonography: An imaging alternative for patients who cannot safely undergo conventional colonoscopy. Has good sensitivity for large lesions but cannot biopsy or remove findings.
Iron Deficiency Anemia as a Colon Cancer Warning Sign
For right-sided colorectal cancer, blood in stool is an invisible symptom. The patient never sees it. The only evidence is the gradual development of iron deficiency anemia — which itself develops slowly enough that many patients adapt to it before a blood test reveals the truth.
Iron deficiency anemia produces a characteristic blood count: low hemoglobin, small red blood cells (low mean corpuscular volume), low ferritin, and often elevated platelets from reactive thrombocytosis. The fatigue and pallor develop over months, and patients often attribute them to stress, aging, or a demanding schedule.
In men of any age and in post-menopausal women, iron deficiency anemia has no physiological explanation — there is no monthly blood loss to account for it. When it appears without an obvious cause, the gastrointestinal tract is the primary source to investigate. Studies find that colonoscopy in this population reveals colorectal cancer in approximately 5–10% of cases and significant colorectal lesions — cancers plus large polyps — in approximately 20–30%.
The clinical imperative: do not treat the anemia without finding its source. Prescribing iron supplementation to a patient with iron deficiency anemia from a bleeding right-sided colon cancer delays a potentially curable diagnosis while the tumor continues to grow.
Frequently Asked Questions
Can I tell from the color of the blood whether it’s cancer?
Not reliably. Bright red blood usually comes from the rectum or left colon — where hemorrhoids and left-sided cancer both occur. Dark red or maroon blood suggests a source higher in the colon, where cancer but not hemorrhoids is the more likely cause. Black, tarry stool indicates upper gastrointestinal bleeding. Color gives probabilities, not diagnoses. The color of blood does not confirm or exclude cancer; evaluation does.
What if I’ve had hemorrhoids for years and this bleeding feels the same?
This is exactly the scenario in which delayed diagnosis most often occurs. Existing hemorrhoids provide a cognitive anchor — the bleeding “feels the same,” so the hemorrhoids must explain it. But colorectal cancer can grow in the background for years, causing the same bright red bleeding that has always been attributed to hemorrhoids. Any new or changed rectal bleeding, or rectal bleeding in a patient who has not had a recent colonoscopy, warrants evaluation.
Sources: Majumdar SR et al., J Gen Intern Med 1999; Ford AC et al., BMJ 2004; ACS Colorectal Cancer Screening Guidelines 2021; NICE NG12 Suspected Cancer 2023.
Other Causes of Blood in Stool: The Full Differential
Blood in stool has a wide differential diagnosis, and colorectal cancer accounts for a minority of cases — even though it is the diagnosis that must be excluded first. Understanding the full range of causes helps patients understand why colonoscopy is recommended even when a benign explanation seems likely on clinical grounds: without direct visualization, a structural source (including cancer) cannot be definitively excluded.
Bright red blood per rectum (hematochezia) most commonly reflects a lower GI source: hemorrhoids (most common cause), anal fissures, diverticular bleeding (common in older adults; typically painless and brisk), colorectal polyps, colorectal cancer, ischemic colitis, infectious colitis, and inflammatory bowel disease (Crohn’s disease or ulcerative colitis). Dark, tarry stool (melena) suggests an upper GI source — stomach or duodenum — including peptic ulcer disease, which is the most common cause of upper GI bleeding. Occult blood detected on fecal testing (FIT or gFOBT) represents microscopic bleeding not visible to the naked eye and covers the full range from benign to malignant sources.
For a comprehensive guide to which colon cancer symptoms — including rectal bleeding — are most clinically significant and how they relate to tumor location, see our article on colon cancer symptoms. For information on stool-based testing for colorectal cancer, including how the FIT test detects occult blood, see our guide to the stool test for colon cancer. For a complete overview of all available colorectal cancer screening options, see our article on colorectal cancer screening.
Iron Deficiency Anemia as a Manifestation of Colorectal Cancer
One important presentation of colorectal cancer — particularly right-sided (ascending colon) cancer — is iron deficiency anemia without visible rectal bleeding. Right-sided tumors tend to bleed slowly and intermittently, with blood mixing throughout the stool column and becoming invisible by the time it is passed. Patients may present to their primary care physician or hematologist with unexplained iron deficiency anemia (low hemoglobin, low ferritin, microcytic red blood cells on blood film), and the source of the iron loss is traced on colonoscopy to a right-sided tumor. Any iron deficiency anemia in a male of any age or in a postmenopausal woman, without a clear alternative explanation, should prompt colonoscopy to exclude colorectal cancer as the bleeding source.
Key Resources
- American Cancer Society — Signs and Symptoms of Colorectal Cancer
- NHS — Rectal Bleeding: Causes and When to See a Doctor
- National Cancer Institute — Colorectal Cancer
Lifestyle Factors and Colorectal Cancer Risk
Beyond screening, understanding the modifiable lifestyle factors that influence colorectal cancer risk provides patients with actionable prevention strategies that complement regular colonoscopy or stool-based testing programs. Colorectal cancer is one of the cancers most strongly linked to modifiable risk factors, and the evidence for several preventive behaviors is substantial enough to have influenced clinical guidelines.
Diet: A diet high in red and processed meat is one of the most consistently documented dietary risk factors for colorectal cancer. The International Agency for Research on Cancer (IARC) classifies processed meat (bacon, sausage, hot dogs, deli meats) as a Group 1 carcinogen for colorectal cancer, and red meat as a Group 2A probable carcinogen. The mechanism involves N-nitroso compounds, heme iron, and heterocyclic amines formed during high-temperature cooking. Conversely, diets high in dietary fiber — particularly from whole grains, legumes, fruits, and vegetables — are associated with reduced colorectal cancer risk, likely through effects on fecal transit time, gut microbiome composition, and fermentation of fiber to short-chain fatty acids (SCFAs) that promote colonocyte health.
Physical activity: Regular physical activity is associated with a 20–25% reduction in colorectal cancer risk in prospective cohort studies. The protective effect appears strongest for colon cancer compared to rectal cancer, and for vigorous activity compared to light activity. Physical activity may reduce colorectal cancer risk through effects on insulin resistance, inflammatory markers, prostaglandin synthesis, and bowel transit time. The ACS recommends at least 150–300 minutes of moderate-intensity activity or 75–150 minutes of vigorous activity per week for cancer prevention.
Body weight: Obesity — particularly central adiposity — is a significant colorectal cancer risk factor. Adipose tissue produces inflammatory cytokines and increases circulating insulin and insulin-like growth factor 1 (IGF-1), which promote colonic epithelial proliferation. Weight loss in overweight individuals is associated with reduced colorectal cancer risk, though the magnitude of risk reduction depends on the degree and duration of weight loss.
Alcohol: Alcohol consumption is associated with increased colorectal cancer risk in a dose-dependent manner. The ACS classifies alcohol as a Group 1 carcinogen for colorectal cancer; even moderate drinking (1–2 drinks/day) is associated with a measurable increase in risk. The mechanism involves acetaldehyde (a toxic alcohol metabolite), folate depletion (alcohol impairs folate absorption and metabolism), and oxidative stress.
Aspirin and NSAIDs: Regular aspirin use has been shown to reduce colorectal cancer incidence and mortality in observational studies and several randomized trials. The protective effect of aspirin on colorectal cancer is attributed to inhibition of cyclooxygenase-2 (COX-2), which mediates prostaglandin E2 synthesis — a key driver of colorectal tumor proliferation. However, USPSTF does not recommend aspirin specifically for colorectal cancer prevention because of the bleeding risk, and the decision to use aspirin should be based on the individual’s cardiovascular risk-benefit profile in consultation with their physician.
Talking to Your Doctor: Questions to Ask
When discussing colorectal cancer prevention, screening, or symptoms with your healthcare provider, being prepared with specific questions helps ensure that you get the information you need to make informed decisions. The following questions are relevant to most scenarios involving colorectal health.
About screening: What colorectal cancer screening test do you recommend for me, and why? Am I at average risk or higher risk? If higher risk, what earlier or more frequent screening schedule should I follow? My father/mother/sibling had colorectal cancer — how does that change my screening timeline?
About test results: My FIT/Cologuard/stool test came back positive — what exactly does this mean, and how quickly do I need a follow-up colonoscopy? My colonoscopy found a polyp — what type was it, what size, and what does this mean for my surveillance schedule? My biopsy showed CIN or dysplasia — what grade, and what is the recommended next step?
About symptoms: I’ve noticed rectal bleeding/blood in stool/bowel habit changes for the past few weeks — should I have a colonoscopy? I am 38 years old and have these symptoms — do my age and lack of risk factors affect whether I need a colonoscopy? My symptoms resolve and then return — is this pattern significant?
About prevention: Are there dietary or lifestyle changes that would meaningfully reduce my colorectal cancer risk? Should I take aspirin for colorectal cancer prevention given my personal risk profile? I have a family history of Lynch syndrome — should I have genetic counseling or germline testing?
Effective communication with your healthcare provider is one of the most important factors in colorectal cancer prevention and early detection. Do not minimize or normalize symptoms — describe them accurately, including when they started, their frequency, whether they are changing, and any associated symptoms. The brief time investment in a productive clinical conversation is vastly outweighed by the benefit of catching a colorectal cancer at an early, curable stage rather than a late, advanced one.
Colorectal cancer remains the second leading cause of cancer death in the United States when men and women are combined, accounting for approximately 52,550 deaths per year (ACS 2023 estimates). Despite these numbers, it is also one of the most preventable and treatable cancers when caught early. Stage I colorectal cancer has a 5-year relative survival rate of approximately 90%; Stage IV drops to approximately 14%. This dramatic survival gradient — from highly curable to largely incurable — underscores why screening, surveillance, and prompt evaluation of symptoms collectively represent the most impactful set of actions any individual can take to reduce their colorectal cancer risk. The tools available today — from FIT stool testing to colonoscopy to Cologuard to the Shield blood test — give patients and clinicians more options than ever to find and prevent colorectal cancer before it becomes life-threatening. Using them at the right time, and following through when results are abnormal, is the single most important factor determining individual outcomes.