
Cystoscopy is the gold standard procedure for directly examining the interior of the urinary bladder and urethra. While it is one of the most commonly performed urological procedures — ordered whenever blood appears in the urine, whenever bladder cancer is being monitored after treatment, or whenever irritative urinary symptoms cannot be explained — many patients approach it with significant anxiety because they do not know what to expect. Understanding what cystoscopy involves, why it is performed, and what it can and cannot detect helps patients comply with the evaluation timeline that gives bladder cancer the best chance of being found early.
What Is Cystoscopy and Why Is It Performed
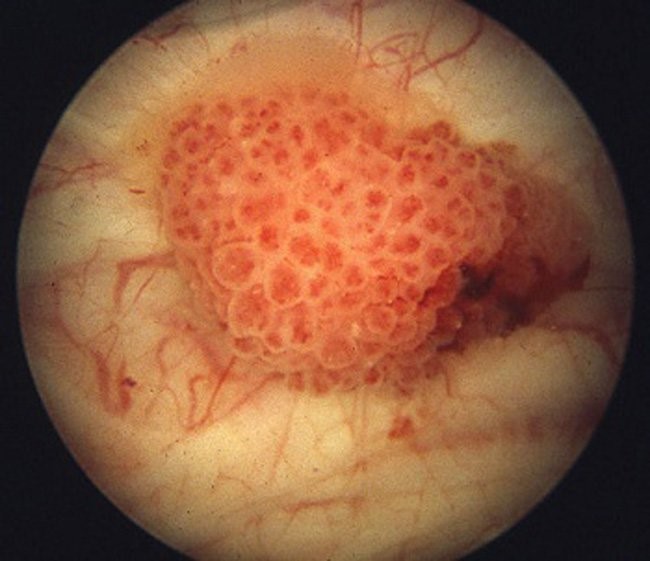
A cystoscope is a thin tube with a light source and a camera at its tip. Passed through the urethra into the bladder, it allows a urologist to directly visualize the entire interior surface of the bladder — the trigone, lateral walls, dome, anterior wall, and ureteral orifices. No other imaging test provides this direct mucosal view. CT scans and MRIs can show the bladder wall and detect large masses; they cannot show the fine surface detail, color, and texture of the urothelium that cystoscopy provides.
The most common indications for cystoscopy include:
- Gross hematuria (visible blood in the urine): Any episode in an adult requires bladder cancer exclusion via cystoscopy and CT urogram
- Microscopic hematuria (≥3 RBCs/HPF without infection): Same evaluation required
- Bladder cancer surveillance: Repeated cystoscopy every 3–12 months after cancer treatment
- Positive urine cytology without a visible lesion: Random biopsies and blue-light cystoscopy needed
- Recurrent UTIs: Assessment for structural causes (diverticula, stones, strictures)
- Suspected carcinoma in situ (CIS): Flat, diffuse cancer often invisible under white light
Flexible vs. Rigid Cystoscopy
Flexible Cystoscopy
Flexible cystoscopy is performed in an outpatient office using local anesthetic gel (intraurethral lidocaine) — no sedation required. The thin, pliable scope (approximately 15–17 French, or 5–5.7 mm) navigates the natural curves of the urethra with minimal discomfort. Most patients describe mild pressure and a brief burning sensation rather than sharp pain. Duration is typically 5–10 minutes. The procedure is diagnostic only — therapeutic instruments cannot be passed through the small working channel.
Rigid Cystoscopy
Rigid cystoscopy requires an operating room and anesthesia (general, spinal, or local). It provides a larger working channel for biopsy forceps, cauterization electrodes, stone-crushing instruments, ureteral stenting equipment, and the resection loop used for transurethral resection of bladder tumor (TURBT). Any tumor removal, formal biopsy, or therapeutic intervention within the bladder requires rigid cystoscopy. If a lesion is found on flexible diagnostic cystoscopy, the patient then returns for rigid cystoscopy and TURBT under anesthesia.
Blue-Light Cystoscopy and Narrow Band Imaging
Standard white-light cystoscopy has a known limitation: carcinoma in situ (CIS), the flat, diffuse high-grade cancer that progresses to muscle invasion in 40–83% of untreated cases, can appear as nothing more than subtle redness — invisible or indistinguishable from inflammation under white light.
Blue-Light Cystoscopy (BLC)
Blue-light cystoscopy uses hexaminolevulinate (Cysview in the US, Hexvix in Europe), instilled into the bladder 60 minutes before the procedure. Cancer cells preferentially accumulate protoporphyrin IX (PpIX) from the agent and fluoresce bright pink or red under blue light, while normal urothelium appears dark. FDA approved in May 2010, BLC detects 20–30% more CIS lesions than white-light alone and reduces the rate of residual tumor at repeat resection by approximately 16%. The AUA and EAU recommend BLC whenever CIS is suspected or when TURBT is performed for high-grade disease.
Narrow Band Imaging (NBI)
NBI requires no contrast agent. Instead, it filters white light to two narrow wavelength bands (415 nm blue and 540 nm green) that are selectively absorbed by hemoglobin. Cancer’s abnormal blood vessel patterns appear as dark brown or black structures against a pale background. Studies show detection rates comparable to BLC without the 60-minute preparation window.
Up to 15–40% of papillary bladder tumors and the majority of CIS lesions are missed at initial TURBT when only white-light cystoscopy is used. Blue-light cystoscopy significantly reduces these residual tumor rates — which is why high-volume bladder cancer centers now use it routinely for TURBT.
What to Expect Before, During, and After Cystoscopy
Before the Procedure
No special diet or bowel preparation is needed. A urine culture should be performed beforehand; any active UTI should be treated and resolved before proceeding. Prophylactic antibiotics may be given based on patient risk. The patient empties the bladder before arriving for flexible office cystoscopy.
During Flexible Office Cystoscopy
Intraurethral lidocaine gel is instilled and held 2–3 minutes. The lubricated scope is then introduced through the urethra. Sterile saline is continuously irrigated to distend the bladder and provide clear visualization. The urologist systematically inspects all surfaces: trigone, lateral walls, dome, anterior wall, and ureteral orifices. Any suspicious lesions are documented by location, size, and appearance. Most examinations complete in 5–10 minutes.
After the Procedure
Post-procedure dysuria (burning urination) and pink urine are common and typically resolve within 24–48 hours. Patients should drink 8+ glasses of water daily for 1–2 days. Seek prompt care for: fever above 38°C (100.4°F), chills, heavy bleeding, or inability to urinate — these may indicate UTI or urinary retention requiring treatment.
What Cystoscopy Can and Cannot Show
Cystoscopy shows: papillary urothelial tumors, CIS (with BLC), bladder stones, diverticula, trabeculation, inflammation, ureteral orifice position, urethral strictures.
Cystoscopy cannot show: upper urinary tract (kidneys, ureters — requires CT urogram), tumor depth and T-staging (requires biopsy/TURBT), lymph nodes and distant metastases (requires staging CT/MRI).
This is why the AUA hematuria guideline requires both CT urogram (upper tract) and cystoscopy (bladder interior). CT misses flat bladder tumors and CIS; cystoscopy misses renal cell carcinoma and upper tract urothelial tumors. Neither alone is sufficient.
Cystoscopy for Bladder Cancer Surveillance
For patients treated for non-muscle-invasive bladder cancer (NMIBC) with TURBT, cystoscopy is the primary surveillance tool. The AUA schedule:
- Year 1: Every 3 months (four cystoscopies)
- Year 2: Every 6 months
- Years 3–5: Annually
- After year 5: Low-risk patients (single, low-grade, small Ta, no recurrence) may be discharged; high-risk patients continue annual surveillance indefinitely
A critical scenario: positive urine cytology with negative white-light cystoscopy does not mean a false-positive cytology. It strongly suggests CIS, which may be flat and diffuse — invisible under white light. The appropriate response is BLC + random biopsies from all bladder quadrants, the bladder neck, and the prostatic urethra in men.
Risks and Complications of Cystoscopy
Cystoscopy is among the safest procedures in urology. Serious complication rate is less than 0.5% for diagnostic flexible cystoscopy.
- Common (>5%): Temporary dysuria, mild hematuria — resolves in 1–2 days
- Less common (1–5%): UTI (1–2%)
- Rare (<1%): Urethral injury, urinary retention, bladder perforation (almost exclusively from rigid scope/TURBT)
The 1–2% UTI risk is substantially lower than the risk of delayed bladder cancer diagnosis from avoiding the procedure. Prophylactic antibiotics reduce this risk further in high-risk patients.
How Cystoscopy Fits Into the Hematuria Evaluation Pathway
Per AUA hematuria guidelines, the complete evaluation pathway is:
- Urinalysis with microscopy: Confirms hematuria (≥3 RBCs/HPF = significant)
- Urine culture: Excludes UTI; if confirmed, treat and re-evaluate at 4–6 weeks
- Urine cytology: Screens for high-grade malignant cells; most sensitive for CIS
- CT urogram: Kidneys, ureters, and bladder wall; preferred upper tract imaging
- Cystoscopy: Direct bladder visualization; the only way to definitively exclude bladder cancer
The goal is to complete this evaluation promptly — within weeks, not months. Delays in bladder cancer diagnosis are associated with stage progression and worse outcomes. Never allow hematuria to go unevaluated because it appeared to resolve on its own.
Frequently Asked Questions About Cystoscopy
Is cystoscopy painful? Flexible office cystoscopy is not typically painful. Most patients describe mild pressure and brief burning as the scope passes through the sphincter. Lidocaine gel significantly reduces discomfort. Post-procedure burning resolves within 24–48 hours.
How long does it take? Diagnostic flexible cystoscopy: 5–10 minutes. Rigid cystoscopy with TURBT in the OR: 15 minutes to an hour or more, depending on tumor size and number.
What if they find something? A suspicious lesion found on flexible diagnostic cystoscopy leads to scheduling of rigid cystoscopy and TURBT under anesthesia, typically within 2–4 weeks. TURBT removes the tumor and provides tissue for pathological staging. If the tumor is confined to the urothelium or lamina propria, intravesical BCG or chemotherapy is given and surveillance begins. If the tumor has invaded the muscle, full staging and treatment planning begins.
For a complete guide to bladder cancer symptoms and what they look like before cystoscopy, or to understand the full treatment pathway after a cystoscopy finds a tumor, see our comprehensive bladder cancer guide. For hematuria from the kidney, see our article on blood in urine and kidney cancer.
Sources: American Urological Association — Hematuria Guidelines | Urology Care Foundation — Cystoscopy | Bladder Cancer Advocacy Network
Cystoscopy vs. Other Bladder Evaluation Tests
Patients referred for hematuria evaluation often ask why multiple tests are required when they might expect a single test to provide all the information. Understanding what each test contributes clarifies why the complete pathway — urinalysis, cytology, CT urogram, and cystoscopy — is necessary rather than redundant.
Cystoscopy vs. CT Urogram: A CT urogram is the imaging test of choice for the upper urinary tract — the kidneys, renal pelvis, and ureters. It detects renal cell carcinoma, upper tract urothelial carcinoma, kidney stones, and hydronephrosis. For the bladder, CT can detect larger masses but routinely misses flat lesions such as CIS and small papillary tumors smaller than 5–8 mm, particularly when the bladder is not adequately distended. Cystoscopy directly visualizes the bladder surface with a level of mucosal detail that no CT or MRI can replicate. A negative CT urogram of the bladder does not exclude bladder cancer.
Cystoscopy vs. Urine Cytology: Urine cytology analyzes cells shed from the urothelium into the urine sample and looks for high-grade malignant cells. It is an excellent screening test for high-grade bladder cancer and CIS — cells from these lesions are morphologically distinctive and recognized by pathologists with high accuracy. However, cytology has low sensitivity for low-grade papillary tumors (which shed cells that look nearly normal) and cannot localize where in the urinary tract the abnormal cells are coming from. A positive cytology without a visible lesion on cystoscopy should trigger blue-light cystoscopy and random biopsies — not reassurance. Cytology and cystoscopy are complementary, not interchangeable.
Cystoscopy vs. MRI (mpMRI of the bladder): Multiparametric MRI of the bladder is emerging as a staging tool for bladder cancer, particularly for assessing muscle invasion before deciding between bladder-sparing trimodality therapy and radical cystectomy. It is not used for initial bladder cancer diagnosis or for routine hematuria evaluation. Cystoscopy and TURBT remain the standard for diagnosis and T-staging.
Cystoscopy vs. Urine Biomarker Tests (NMP22, UroVysion FISH, BladderEDx): Several FDA-cleared urine biomarker tests are available as adjuncts to cystoscopy in bladder cancer surveillance. They detect specific proteins, chromosomal alterations, or methylation markers associated with urothelial carcinoma. These tests can increase detection sensitivity in surveillance patients, particularly between scheduled cystoscopies, but none replaces cystoscopy for diagnosis or surveillance. Current AUA guidelines reserve their use as adjuncts in selected situations, not as standalone surveillance tools.
Special Situations in Cystoscopy Practice
Cystoscopy After Positive Urine Cytology
Positive urine cytology is a significant finding that demands a thorough cystoscopic evaluation even when initial white-light cystoscopy appears normal. The pattern — malignant cells in the urine, no visible lesion in the bladder — is classic for carcinoma in situ, which may be flat, diffuse, and invisible under white light. The appropriate next step is blue-light cystoscopy (if not already performed) combined with a systematic random biopsy protocol: biopsies from the right lateral wall, left lateral wall, posterior wall, dome, trigone, and bladder neck, plus prostatic urethral biopsies in men. This approach identifies CIS that would otherwise be missed, allowing early intravesical BCG treatment before muscle invasion occurs.
Cystoscopy in Women
Women are significantly less likely to receive prompt cystoscopy evaluation after hematuria compared to men, despite having similar bladder cancer risk once evaluated. The most common reasons for delayed evaluation in women include hematuria attributed to UTI without confirmatory culture, menstrual contamination of urine samples, and the incorrect assumption that bladder cancer is primarily a disease of men. Any woman over 35 with gross hematuria not explained by confirmed bacterial infection should receive CT urogram and cystoscopy on the same timeline as a man with the same presentation. Age and gender do not modify the AUA hematuria guideline’s evaluation requirement.
Cystoscopy Under Anticoagulation
Patients on anticoagulants (warfarin, apixaban, rivaroxaban, dabigatran) who require cystoscopy present a management challenge. For diagnostic flexible cystoscopy alone — no biopsy anticipated — anticoagulation does not need to be interrupted because the procedure does not involve cutting or burning of tissue. If biopsy or TURBT is anticipated, anticoagulant management (bridging or temporary cessation) should be coordinated between the urologist and prescribing clinician. In patients on anticoagulants who develop hematuria, the AUA guideline is explicit: anticoagulants cause existing lesions to bleed earlier, not create new ones. The evaluation is required regardless of anticoagulation status.
Cystoscopy and Bladder Diverticula
A bladder diverticulum is an outpouching of the bladder wall where the muscular layer is absent — a structural defect, not a cancer. However, bladder cancer can develop within a diverticulum, and this is particularly dangerous because the absence of the muscle layer means a diverticular cancer cannot be staged as T2 (muscle invasion) and may instead spread directly to perivesical fat (T3) without crossing muscle. Thorough cystoscopic examination of any known diverticula — which requires repositioning and directing the cystoscope into the diverticular opening — is essential in any patient with hematuria and known diverticula.
Living With Bladder Cancer Surveillance Cystoscopy
For patients who have completed treatment for NMIBC and enter the surveillance phase, the cystoscopy schedule becomes a defining feature of their life for years — in some cases indefinitely. The psychological experience of this schedule is well studied. Patients consistently report high anxiety in the days and weeks before each surveillance cystoscopy, a phenomenon variously called “scopeophobia,” “cystoscopy anxiety,” or “bladder cancer scanxiety.” This anxiety peaks in the 1–2 weeks before the procedure and then resolves sharply after a clear result.
Several strategies help patients manage surveillance anxiety:
- Understanding that the procedure itself is brief and the discomfort manageable — first-time patients consistently rate post-procedure experience as less distressing than anticipated
- Scheduling cystoscopies at predictable intervals rather than allowing appointments to drift — irregular scheduling extends the period of uncertainty
- Between-appointment awareness: knowing which symptoms (new gross hematuria, worsening urgency, pelvic pain) should trigger an unscheduled call to the urologist rather than waiting for the next appointment
- Peer support through bladder cancer advocacy organizations — connecting with others on the same surveillance schedule normalizes the experience
Adherence to the surveillance cystoscopy schedule is not optional — it is the mechanism by which recurrences are caught before they progress to muscle invasion and require radical cystectomy. Patients who miss surveillance cystoscopies are more likely to present with higher-stage recurrences at the time of eventual detection. The inconvenience and anxiety of periodic cystoscopy is the cost of bladder preservation.
For a comprehensive overview of what triggers a cystoscopy referral, see our guide to bladder cancer symptoms and what they mean. To understand the full treatment pathway after cystoscopy finds a tumor, see our bladder cancer treatment guide. And for evaluation of blood in urine from the upper urinary tract, see our article on kidney cancer and blood in urine.
Preparing Your Questions for the Cystoscopy Appointment
Patients who come prepared with questions get more useful information from their cystoscopy appointment and better understand the next steps after the procedure. Useful questions to ask your urologist before or during the cystoscopy include:
- Will this be flexible or rigid cystoscopy, and will I be awake?
- Will blue-light cystoscopy (Cysview) be used? Is it available at this facility?
- If a lesion is found today, what happens next and how quickly?
- Should I hold any of my medications (anticoagulants, immunosuppressants) before the procedure?
- What is my surveillance schedule if this cystoscopy is clear?
- If my urine cytology was positive, what does a normal-appearing cystoscopy mean — do I still need random biopsies?
- When should I call after the procedure vs. go to urgent care?
The Bottom Line on Cystoscopy
Cystoscopy is a brief, well-tolerated procedure that provides information no other test can: a direct look inside the bladder. It is the only test that can definitively identify or exclude a bladder tumor, locate carcinoma in situ, and provide the tissue specimen needed for staging. For patients with blood in the urine, cystoscopy is not optional — it is the essential second step after CT urogram in the AUA hematuria pathway. For patients already treated for bladder cancer, it is the surveillance mechanism that separates early recurrence from late-stage diagnosis.
The anxiety that many patients feel about cystoscopy is understandable. But for the vast majority of patients, the experience is far less distressing than anticipated, the procedure is over in less than 10 minutes, and the information it provides can be lifesaving. Delaying or avoiding cystoscopy because of fear of the procedure is one of the most predictable and preventable reasons that bladder cancer is diagnosed at a later, harder-to-treat stage. If you have been referred for cystoscopy, the most important thing you can do for your health is to schedule and attend the appointment promptly.
What Happens to the Tissue After a Cystoscopy Biopsy
When a suspicious lesion is found during cystoscopy and a biopsy or TURBT is performed, the resected tissue is sent to a pathologist for histological analysis. The pathology report determines two critical facts: the grade of the tumor (low-grade vs. high-grade, which describes how abnormal the cells look and how aggressively the cancer is likely to behave) and the stage (Ta, T1, T2+, which describes how deep the cancer has grown into the bladder wall). Grade and stage together determine whether intravesical therapy alone is sufficient, whether adjuvant systemic chemotherapy is needed, or whether radical cystectomy is required. The accuracy of this pathology report depends on the quality and depth of the TURBT — superficial biopsies that do not include the detrusor muscle cannot rule out muscle invasion, and may require repeat resection (re-TURBT) 4–6 weeks later to confirm staging. This is a well-established quality standard in bladder cancer surgery: for any high-grade tumor, the TURBT specimen must include muscularis propria (detrusor muscle) to be considered an adequate resection for staging purposes.