Bladder cancer is the fourth most common cancer in men in the United States, with approximately 83,000 new cases diagnosed annually and about 17,000 deaths per year. The bladder is a hollow muscular organ in the lower pelvis that stores urine until it is expelled during urination. Bladder cancer overwhelmingly arises from the urothelial cells — the specialized cells lining the inner surface of the bladder, ureters, and renal pelvis. The central challenge of bladder cancer is not just treating it, but managing a disease with an exceptionally high recurrence rate: even after successful initial treatment, more than half of all patients will develop a recurrence in the bladder within five years, requiring lifelong surveillance cystoscopy.
Types of Bladder Cancer
Urothelial carcinoma (formerly transitional cell carcinoma, TCC) accounts for 90 to 95 percent of all bladder cancers in the United States. It may grow as papillary (frond-like) tumors that project into the bladder lumen, or as flat lesions including carcinoma in situ (CIS) — particularly dangerous because CIS appears flat and unremarkable on standard white-light cystoscopy while carrying a high rate of progression to muscle-invasive disease.
Squamous cell carcinoma accounts for approximately 5 percent of US bladder cancers and is more common in regions where Schistosoma haematobium infection causes chronic bladder inflammation. In the US, it is associated with chronic bladder irritation from long-term catheterization, recurrent infections, and bladder stones.
Adenocarcinoma (<2%) may arise from the urachal remnant at the bladder dome or from glandular metaplasia of the urothelium. Small cell neuroendocrine carcinoma of the bladder is rare but extremely aggressive, treated similarly to small cell lung cancer with platinum-based chemotherapy.
Risk Factors for Bladder Cancer
Smoking is the single most important modifiable risk factor, responsible for an estimated 50 percent of bladder cancer cases in men and 25 to 30 percent in women. Risk is approximately 3 to 4 times that of non-smokers. Carcinogens in tobacco smoke — particularly aromatic amines and polycyclic aromatic hydrocarbons — are concentrated in the bladder during urine storage. After stopping smoking, risk declines gradually, but even former smokers retain elevated risk for decades.
Occupational chemical exposures: Aromatic amines (benzidine, beta-naphthylamine, 4-aminobiphenyl) used in the dye, rubber, leather, and printing industries cause bladder cancer after a latency period extending up to 40 to 45 years. Truck drivers (diesel exhaust), hairdressers, and aluminum smelter workers have elevated documented risks.
Cyclophosphamide chemotherapy is metabolized to acrolein — a direct urothelial carcinogen that accumulates in the bladder. Mesna prevents this risk when co-administered with high-dose cyclophosphamide. Pelvic radiation therapy increases bladder cancer risk 2 to 4 times, with a latency of 10 to 20 years. Chronic bladder irritation from long-term indwelling catheters increases squamous cell carcinoma risk.
Non-muscle-invasive (Ta/T1/CIS): ~90%+ 5-year survival • Muscle-invasive (T2–T4): ~50% • Metastatic: ~8%. The high recurrence rate of NMIBC (50–70% within 5 years) makes lifelong surveillance cystoscopy essential even after successful treatment.
Symptoms of Bladder Cancer
Hematuria (blood in the urine) is the cardinal symptom — classically painless and intermittent. Any episode of gross hematuria in an adult warrants cystoscopy and upper tract imaging. The intermittency of tumor-related hematuria creates dangerous false reassurance. Irritative voiding symptoms — urgency, frequency, dysuria — are characteristic of carcinoma in situ (CIS) and are frequently misattributed to cystitis. Recurrent irritative symptoms without infection in a patient with smoking history should prompt cystoscopy. Flank pain occurs when a bladder tumor obstructs the ureteral orifice, causing hydronephrosis.

Diagnosis
Cystoscopy is the gold standard — a thin camera passed through the urethra directly visualizes the bladder interior, identifying papillary tumors and flat erythematous areas suggesting CIS. Blue-light cystoscopy uses hexaminolevulinate (a photosensitizer preferentially taken up by tumor cells, which then appear bright pink under blue light) to dramatically improve detection of CIS and flat tumors missed under white light. CT urogram stages MIBC and evaluates the entire urothelial tract for synchronous upper tract tumors (present in 3–5% of bladder cancer patients). TURBT (transurethral resection) is both diagnostic and therapeutic for NMIBC — the resected specimen provides histological type, grade, and the critical staging determination of whether muscularis propria is invaded. Urine cytology is highly sensitive for high-grade tumors and CIS but poor for low-grade papillary tumors.
Staging: NMIBC vs. MIBC
The most critical staging distinction is whether the tumor invades the muscularis propria:
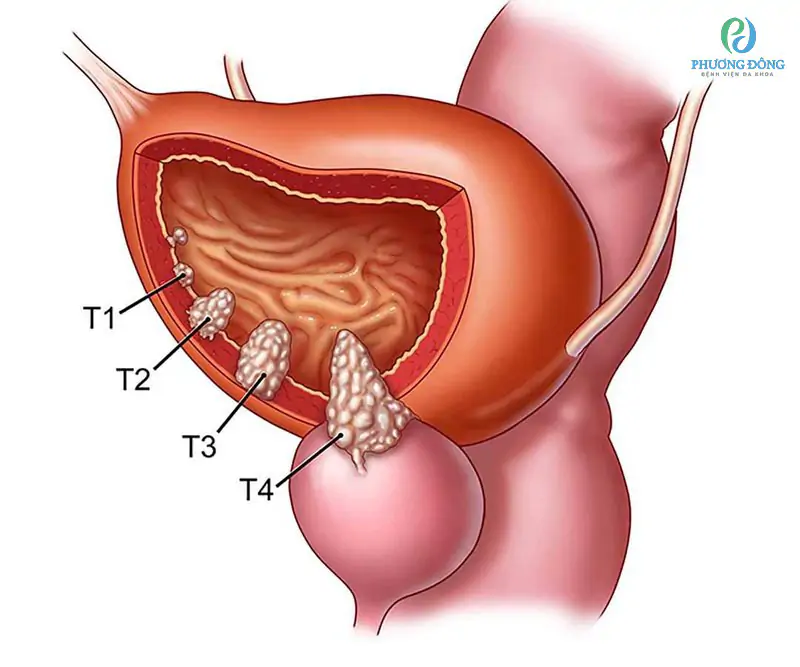
- CIS (Tis): flat, high-grade; does not invade; high progression risk
- Ta: non-invasive papillary tumor confined to urothelium
- T1: invades lamina propria but not muscle — these three stages = NMIBC
- T2: invades muscularis propria — begins MIBC; requires different treatment pathway
- T3–T4: extends into perivesical fat or adjacent organs
- N1–3: lymph node metastasis; M1: distant metastasis (lung, liver, bone, lymph nodes)
Treatment of NMIBC
TURBT removes the visible tumor; re-TURBT at 4–6 weeks is performed for T1 tumors (residual disease found in 33–80% of cases). Intravesical BCG (Bacillus Calmette-Guérin) immunotherapy — instilled directly into the bladder through a catheter — is the most effective treatment for high-risk NMIBC (T1, high-grade Ta, CIS), reducing recurrence ~30–40% and progression ~25% compared to TURBT alone. Intravesical chemotherapy (mitomycin C, gemcitabine) is used for lower-risk NMIBC; a single post-TURBT instillation reduces recurrence from residual implanted cells. Pembrolizumab was FDA-approved in 2020 for BCG-unresponsive high-risk NMIBC with CIS (KEYNOTE-057; ~40% complete response rate), offering an alternative to cystectomy for BCG-refractory disease.
Treatment of MIBC
Neoadjuvant cisplatin-based chemotherapy (GC or ddMVAC) followed by radical cystectomy is the standard of care for eligible MIBC patients. Neoadjuvant chemotherapy reduces death risk ~8% by treating micrometastatic disease before surgery. Radical cystectomy removes the entire bladder plus surrounding organs (prostate and seminal vesicles in men; uterus, ovaries, and anterior vaginal wall in women) along with extensive pelvic lymph node dissection. Urinary diversion after cystectomy uses a bowel segment: ileal conduit (stoma into external appliance), orthotopic neobladder (voiding through urethra; requires catheterization training, B12 monitoring), or continent cutaneous diversion (catheterized pouch through abdominal wall).
Trimodality therapy (TMT) — maximal TURBT + concurrent chemoradiation — achieves 5-year OS of 50–60% for MIBC in specialized centers with bladder preservation, though ongoing surveillance is required.
Treatment of Metastatic Bladder Cancer
Enfortumab vedotin + pembrolizumab (EV-302/KEYNOTE-A39) became the new first-line standard in 2024, with ORR 68% and median OS 31.5 months versus 16.1 months for gemcitabine + cisplatin — a landmark improvement over the 30-year standard. FGFR inhibitors: approximately 15–20% of bladder cancers harbor FGFR3 mutations; erdafitinib is FDA-approved for platinum-refractory FGFR-altered bladder cancer. Other second-line options include sacituzumab govitecan and pembrolizumab.
Surveillance After Bladder Cancer Treatment
NMIBC requires lifelong surveillance cystoscopy: every 3 months for year 1, every 6 months for year 2, then annually — indefinitely. The high recurrence rate (50–70% within 5 years) means surveillance is not optional and should never be stopped based on multiple consecutive negative cystoscopies alone. Upper tract imaging is performed periodically to detect upper urinary tract recurrences.
Bladder cancer shares the presentation of hematuria with kidney and upper tract urothelial cancers. Our article on blood in urine from kidney cancer explains why the evaluation of hematuria must include both cystoscopy (for bladder) and CT urogram (for upper tract). For comparison with renal malignancies, see our guides to kidney cancer symptoms and renal cell carcinoma.
Sources: National Cancer Institute — Bladder Cancer | American Cancer Society — Bladder Cancer | Bladder Cancer Advocacy Network
Understanding BCG Therapy — Why a Tuberculosis Vaccine Treats Bladder Cancer
One of the most counterintuitive treatments in oncology is the use of BCG (Bacillus Calmette-Guérin) — a live attenuated strain of Mycobacterium bovis originally developed as a tuberculosis vaccine — as the primary immunotherapy for high-risk non-muscle-invasive bladder cancer. Understanding why BCG works helps patients appreciate both the treatment’s remarkable effectiveness and its side effect profile.
BCG is instilled directly into the bladder through a urinary catheter and retained for approximately 2 hours before being voided. When BCG comes into contact with the urothelium, it is taken up by bladder cells and triggers a powerful local innate and adaptive immune response. This immune response — characterized by recruitment of CD4+ T cells, NK cells, neutrophils, and macrophages into the bladder wall — kills any residual cancer cells through a combination of direct cytotoxicity and cytokine-mediated tumor rejection. BCG essentially converts the bladder into an immunologically active microenvironment hostile to tumor growth.
The standard BCG induction course consists of weekly instillations for 6 consecutive weeks. Maintenance BCG — additional instillation courses at 3 months, 6 months, and then every 6 months for 1 to 3 years — has been shown to significantly improve the duration of BCG’s protective effect compared to induction alone. The SWOG 8507 trial demonstrated that 3-year maintenance BCG substantially reduced disease progression compared to no maintenance.
Side effects of BCG are related to the local immune response: urinary symptoms (frequency, urgency, dysuria, hematuria) are expected and typically resolve within a few days of each instillation. Systemic BCG infection (BCGosis) is a rare but serious complication occurring when BCG enters the systemic circulation, typically through traumatic catheterization or active hematuria at the time of instillation. BCGosis presents with high fever, systemic sepsis, and can affect the lungs, liver, and other organs; it requires prolonged antituberculous antibiotic therapy. BCG should not be instilled in patients with traumatic catheterization, gross hematuria, active urinary tract infection, or significantly immunocompromised patients.
The BCG Shortage and Alternative Intravesical Agents
Periodic worldwide BCG shortages — caused by manufacturing disruptions, vaccine demand, and supply chain issues — have forced urologists to develop and implement alternative intravesical treatment strategies. During shortage periods, alternative agents include:
- Gemcitabine + docetaxel sequential intravesical therapy: emerging evidence supports this combination as an alternative to BCG for high-risk NMIBC, with similar recurrence-free survival rates in comparative studies at specialized centers
- Mitomycin C: the most widely used alternative intravesical chemotherapy; most effective as a single immediate post-TURBT instillation for low-intermediate risk disease
- Hyperthermic intravesical chemotherapy (HIVEC): mitomycin C delivered at elevated temperature (40–44°C) using a device to heat the drug within the bladder, improving drug penetration into the urothelium; approved in Europe; used in the US on a compassionate basis
- TAR-200 (gemcitabine-releasing intravesical device): a sustained-release gemcitabine device implanted into the bladder at cystoscopy that continuously releases drug over weeks; being evaluated in Phase 3 trials for BCG-unresponsive NMIBC
Bladder Preservation With Trimodality Therapy
Radical cystectomy — while the most effective curative treatment for MIBC — is a major surgery with significant morbidity, a prolonged recovery, and a permanent change in body function from urinary diversion. For patients who wish to preserve their bladder, trimodality therapy (TMT) offers a genuine alternative with comparable long-term survival outcomes when applied to appropriately selected patients.
The ideal candidate for TMT has a single, small MIBC tumor (<5 cm), no CIS elsewhere in the bladder, no hydronephrosis (which would suggest deep muscle or ureteral involvement), adequate bladder capacity, and has undergone complete or near-complete TURBT of the visible tumor. Concurrent chemotherapy — typically cisplatin or 5-FU + mitomycin C — radiosensitizes the tumor during external beam radiation. Long-term results from Harvard, Princess Margaret, and other specialized TMT programs show 5-year bladder-intact survival of 40 to 50 percent with overall survival comparable to cystectomy series.
The critical ongoing requirement for TMT patients is surveillance cystoscopy every 3 months for the first 2 years, then every 6 months. Muscle-invasive recurrence in a preserved bladder — detected early — can be managed with salvage cystectomy. Late bladder recurrences that remain non-muscle-invasive can be treated with TURBT and intravesical therapy. The bladder preserved by TMT is functional in the majority of patients, though late radiation effects (radiation cystitis, reduced capacity, occasional obstructive uropathy) affect a subset over many years.
Molecular Targets and Biomarkers in Bladder Cancer
Bladder cancer has one of the highest somatic mutation rates of any solid tumor, reflecting the chronic carcinogenic exposure from urine constituents. This high mutational burden has several clinical implications:
FGFR alterations (mutations or fusions of FGFR1, FGFR2, or FGFR3) occur in approximately 15 to 20 percent of urothelial carcinomas, enriched in low-grade NMIBC and in luminal-papillary MIBC. Erdafitinib, a pan-FGFR tyrosine kinase inhibitor, is FDA-approved for platinum-refractory FGFR2/3-altered urothelial carcinoma, with an objective response rate of approximately 40 percent in biomarker-selected patients — substantially better than chemotherapy in the same setting. Testing for FGFR alterations (by tumor molecular profiling) should be considered at recurrence after platinum-based chemotherapy to identify erdafitinib-eligible patients.
PD-L1 expression is used for patient selection in some pembrolizumab and atezolizumab trials, though its predictive value is imperfect. High tumor mutational burden (TMB) independently predicts immunotherapy response in bladder cancer, as it does across multiple tumor types.
Nectin-4 is the target of enfortumab vedotin (EV) — an antibody-drug conjugate that delivers monomethyl auristatin E (MMAE), a microtubule inhibitor, directly to Nectin-4-expressing tumor cells. Nectin-4 is expressed in nearly all urothelial carcinomas, which is why EV achieves high response rates in an unselected population. The combination with pembrolizumab appears to produce synergistic immune activation, explaining the dramatic outcomes improvement seen in the EV-302 trial compared to chemotherapy alone.
Psychosocial Impact of Bladder Cancer and Cystectomy
Bladder cancer has a profound impact on quality of life that extends far beyond the physical effects of treatment. The chronic nature of NMIBC — with its lifelong surveillance requirement, frequent cystoscopies, and constant recurrence anxiety — creates what patients often describe as “scanxiety”: the recurring anxiety before each surveillance cystoscopy about whether the cancer has returned.
For patients who undergo radical cystectomy, the psychological adjustment involves accepting permanent changes in bodily function, body image, and sexual function. Men who undergo radical cystectomy have high rates of erectile dysfunction (from neurovascular bundle disruption) and anejaculation (from prostatectomy). Women may experience vaginal dryness, dyspareunia, and body image concerns related to the cystectomy. Sexual health counseling, pelvic floor rehabilitation, and, where appropriate, pharmacological or device-based management of sexual dysfunction are important components of post-cystectomy care that are often underutilized.
Ostomy support is essential for patients with ileal conduit urinary diversions. Certified wound, ostomy, and continence (WOC) nurses provide pre-operative education, help with stoma siting, and ongoing post-operative management of stoma-related complications. Patient-to-patient peer support through the United Ostomy Associations of America (UOAA) connects cystectomy patients with others who have navigated the same experience.
Upper Tract Urothelial Carcinoma and Its Relationship to Bladder Cancer
Urothelial carcinoma does not occur only in the bladder. The same cell type — the urothelial cell — lines the renal pelvis and ureter (upper urinary tract), and cancer can arise from these locations as well. Upper tract urothelial carcinoma (UTUC) accounts for approximately 5 percent of all urothelial malignancies and is more common in men, in smokers, and in patients with hereditary conditions such as Lynch syndrome (hereditary mismatch repair deficiency).
UTUC is clinically related to bladder cancer in several important ways. Patients with UTUC have a 30 to 50 percent lifetime risk of developing a bladder cancer, making bladder surveillance essential after UTUC treatment. Conversely, patients with bladder urothelial carcinoma have a 3 to 5 percent risk of synchronous or subsequent UTUC, which is why CT urogram (evaluating the upper tracts) is included in the standard bladder cancer workup. Aristolochic acid nephropathy — associated with herbal medicines containing Aristolochia plants, particularly prevalent in Taiwan and parts of East Asia — causes a specific UTUC pattern with bilateral upper tract involvement.
Treatment of UTUC differs from bladder cancer. Radical nephroureterectomy (removal of the kidney, ureter, and a bladder cuff) is the standard curative treatment. Nephron-sparing approaches (endoscopic ablation of the upper tract tumor) are reserved for patients with bilateral disease or solitary kidneys where radical surgery would leave them dialysis-dependent. Adjuvant nivolumab is FDA-approved for UTUC with certain high-risk features after nephroureterectomy, based on the CheckMate 274 trial data for urothelial carcinoma post-resection.
Bladder Cancer in Women — Diagnostic Delays and Disparities
Bladder cancer is significantly less common in women than in men, which contributes to a well-documented pattern of diagnostic delay. Women with hematuria are more commonly attributed to gynecological causes — menstrual contamination, urinary tract infection, or urethral pathology — without prompt cystoscopic evaluation. Studies have consistently shown that women present with bladder cancer at a more advanced stage on average than men, a disparity that partly reflects delayed diagnosis.
A woman with painless gross hematuria deserves exactly the same cystoscopy and CT urogram as a man with the same presentation. Menstrual contamination should be excluded (urine collected after menstruation ends, or with a tampon in place), but should not be used as a reason to defer urothelial evaluation in a woman with persistent or recurrent hematuria. Urologists and primary care physicians should apply the same index of suspicion for bladder cancer in women with unexplained hematuria as they do in men of similar age and smoking history.
Diet, Lifestyle, and Bladder Cancer Prevention
While no dietary intervention has proven to prevent bladder cancer in randomized trials, several observational associations are worth noting:
- Hydration: higher fluid intake reduces urinary carcinogen concentration in the bladder, theoretically reducing urothelial exposure time; some studies show reduced bladder cancer risk with higher daily water intake
- Cruciferous vegetables: compounds in broccoli, cabbage, and Brussels sprouts (isothiocyanates) have shown bladder cancer risk reduction in observational studies, possibly through carcinogen detoxification pathways
- Arsenic: arsenic in drinking water is a well-established bladder carcinogen in endemic regions; home water filtration for arsenic is advisable in affected areas
- Smoking cessation: the single most impactful lifestyle intervention; reduces ongoing carcinogen exposure to the urothelium immediately; long-term risk reduction accumulates over years
Patients who have been treated for bladder cancer and who continue to smoke have substantially higher recurrence rates than those who quit. Smoking cessation support — including pharmacotherapy (varenicline, bupropion, nicotine replacement) and behavioral counseling — should be actively offered to all bladder cancer patients who smoke, not simply mentioned as a recommendation. The recurrence reduction from quitting is among the most powerful risk-modifying interventions available to the patient themselves.
Bladder cancer is a chronic disease that demands a chronic management strategy — regular surveillance, prompt attention to new symptoms, smoking cessation, and ongoing communication with a urological oncology team. Patients who understand their disease, maintain surveillance adherence, and advocate for timely evaluation of any new hematuria give themselves the best chance of long-term disease control.