
Blood in the urine is the most common symptom of bladder cancer, present in approximately 85 percent of patients at the time of diagnosis. Yet for many patients, that blood — often painless, often brief, often followed by days or weeks of completely normal urine — does not feel like an emergency. This perception is one of the most dangerous misunderstandings in urological oncology. Understanding what bladder cancer symptoms truly look like, and which features make them more suspicious, can shorten the path to diagnosis and change outcomes.
Blood in the Urine — The Cardinal Symptom
Hematuria is classically painless. This is the most important distinguishing feature. UTI-related hematuria is accompanied by burning, urgency, and frequency. Kidney stone hematuria is accompanied by severe, colicky flank pain. Bladder cancer hematuria, in contrast, often appears without any other symptom — the urine simply changes color, and there is no pain at all. Painless hematuria is a red flag for urinary tract malignancy, and it demands investigation regardless of the patient’s age, gender, or other clinical characteristics.
It is typically intermittent. The tumor bleeds when a small blood vessel on its surface ruptures, then stops temporarily as a clot forms or the vessel seals. The patient may see red or cola-colored urine for one or two days, and then nothing for weeks — followed by another episode. This on-off pattern creates powerful false reassurance. In fact, the intermittency is a characteristic feature of tumor bleeding, not evidence of a benign cause. Every recurrence should be evaluated with the same urgency as the first episode.
It can be gross or microscopic. Gross hematuria is visible to the naked eye — the urine appears pink, red, orange, brown, or cola-colored. As little as one milliliter of blood per liter of urine is enough to produce visible discoloration. Microscopic hematuria is detected only on urinalysis (≥3 RBCs per high-power field). Both types warrant evaluation. The quantity of blood does not determine the risk — even trace gross hematuria demands investigation.
Any blood in the urine in an adult — gross or microscopic, painless, even if it resolved — requires CT urogram and cystoscopy. Antibiotics are not an appropriate first response unless a urine culture confirms bacterial infection. One evaluation can catch bladder cancer before it invades the muscle wall.
Irritative Voiding Symptoms — Urgency, Frequency, Dysuria
Some bladder cancer presentations are dominated by irritative voiding symptoms — a pattern particularly characteristic of carcinoma in situ (CIS). Urinary urgency (sudden compelling need to urinate), frequency (needing to urinate more than 8 times/day with small volumes), and dysuria (burning urination) can all occur from the constant bladder wall irritation caused by diffuse CIS — without gross hematuria.
This is the clinical trap: CIS produces irritative symptoms that are indistinguishable from cystitis or overactive bladder, without the visible blood that alerts patients and clinicians to something more serious. A patient with CIS may be treated repeatedly for UTI or OAB while the cancer progresses untreated toward muscle invasion. The key trigger for suspicion: irritative voiding symptoms persisting despite negative urine cultures and antibiotic trials, particularly in a patient over 50 with a smoking history. Urine cytology and cystoscopy with blue-light evaluation should be performed.
Pelvic Pain, Flank Pain, and Advanced Symptoms
Pelvic or suprapubic pain is not typical of early bladder cancer. It suggests either a very large tumor or muscle-invasive/locally advanced disease. Flank pain occurs when a tumor obstructs the ureteral orifice, causing hydronephrosis (distension of the renal pelvis and ureter). New hydronephrosis in a bladder cancer patient is a staging-relevant finding associated with more advanced disease.
Leg swelling (lymphedema) can occur when pelvic lymph node metastases compress the iliac veins and lymphatics draining the lower extremities.
Carcinoma In Situ — The Silent, High-Risk Lesion
Carcinoma in situ (CIS) is a flat, high-grade urothelial cancer confined to the surface epithelium that spreads as a diffuse redness difficult to see under white-light cystoscopy. Despite being histologically early, CIS progresses to muscle-invasive disease in 40 to 83 percent of untreated cases. It is not the indolent low-grade papillary tumor that recurs but rarely progresses — it is the lesion that most urgently requires aggressive intravesical BCG therapy and close surveillance.
Symptomatically, CIS presents with urgency, frequency, and dysuria, often without gross hematuria. Urine cytology is the most sensitive diagnostic test for CIS because the high-grade malignant cells are shed in large numbers into the urine. Any patient with positive urine cytology without a visible bladder lesion on white-light cystoscopy should undergo blue-light cystoscopy (using hexaminolevulinate photodynamic imaging, which makes CIS appear bright pink) and random bladder biopsies to find the CIS.
Why Bladder Cancer Symptoms Are Misattributed
Hematuria attributed to UTI: approximately half of patients with bladder cancer who present with hematuria receive a UTI diagnosis and antibiotic treatment without cystoscopy. The correct protocol: treat any confirmed UTI, then re-evaluate urine at 4–6 weeks after antibiotic completion. If hematuria persists or there is no confirmed infection, CT urogram and cystoscopy are indicated regardless of the initial clinical impression. Never prescribe a second antibiotic course for unexplained hematuria.
Irritative symptoms attributed to OAB or IC: women in particular are at risk for overactive bladder or interstitial cystitis misdiagnosis when irritative voiding symptoms are the presenting feature of CIS. Any OAB or IC diagnosis in a patient over 50 with a smoking history, without a cystoscopy having been performed, should be questioned. BPH misdiagnosis in older men: any man with new hematuria, even in the context of known BPH, requires bladder cancer evaluation — BPH does not explain hematuria conclusively.
Evaluation for Bladder Cancer Symptoms
- Urinalysis with microscopy: confirms hematuria; evaluates for pyuria
- Urine culture: excludes UTI; negative culture removes UTI from differential
- Urine cytology: most sensitive for high-grade tumors and CIS; positive cytology = investigate thoroughly
- CT urogram: evaluates kidneys, ureters, and bladder simultaneously; identifies upper tract tumors and bladder lesions
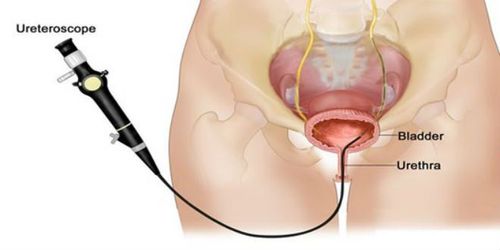
- Cystoscopy: gold standard direct visualization; allows biopsy of suspicious areas
- Blue-light cystoscopy: improves CIS detection 20–30% over white light; recommended when CIS is suspected
When to See a Doctor
- Any gross hematuria in an adult — evaluation within 1–2 days; same-day if passing clots or unable to urinate
- Microscopic hematuria without confirmed UTI — cystoscopy and CT urogram within 2 weeks
- Irritative voiding symptoms (urgency, frequency, dysuria) not resolving after antibiotics — cystoscopy with urine cytology
- Hematuria recurring after antibiotic treatment — CT urogram + cystoscopy (do not repeat antibiotics)
- New flank pain with hematuria — CT urogram promptly to exclude ureteral obstruction
- Pelvic pain, leg swelling, bone pain in a patient with known bladder cancer — urgent re-staging
Never allow hematuria to go unevaluated because it resolved on its own. For the complete evaluation protocol and treatment overview, see our bladder cancer guide. For the hematuria evaluation pathway covering both bladder and kidney causes, see our article on blood in urine from kidney cancer. And for comparison with kidney cancer symptom patterns, see our guide to kidney cancer symptoms.
Sources: National Cancer Institute — Bladder Cancer | American Cancer Society — Bladder Cancer | Bladder Cancer Advocacy Network
How Bladder Cancer Symptoms Differ by Histological Type
Not all bladder cancers present identically, and understanding how symptoms differ by tumor type helps explain why some bladder cancers are caught early while others are not:
Low-grade papillary urothelial carcinoma (the most common type) grows as visible frond-like projections into the bladder lumen. It almost always causes hematuria by virtue of its blood vessels being directly exposed to urine flow. Low-grade papillary tumors rarely cause irritative symptoms (because they do not inflame the entire urothelium), and they rarely produce constitutional symptoms (because they rarely metastasize). The symptom pattern is typically isolated, painless, intermittent gross hematuria — sometimes with a background of microscopic hematuria between grossly bloody episodes. These tumors, if found early, are managed effectively with TURBT and intravesical therapy, but they recur frequently, which is why surveillance is lifelong.
High-grade papillary urothelial carcinoma produces the same hematuria as low-grade papillary tumors but may additionally cause irritative symptoms from the more aggressive local tissue reaction it provokes. High-grade tumors have a substantially higher rate of muscle invasion (20–40%) than low-grade tumors (1–3%), and patients with high-grade disease should be aware that the stakes of prompt treatment and surveillance are considerably higher.
Carcinoma in situ (CIS) — as discussed in detail above — produces primarily irritative voiding symptoms without visible hematuria, and it may appear normal under white-light cystoscopy. Its flat, aggressive, diffuse nature makes it the most dangerous early-stage bladder cancer variant.
Muscle-invasive bladder cancer (MIBC) by definition has grown through the urothelium and lamina propria into the muscular bladder wall. At this stage, symptoms are more continuous and severe: persistent hematuria (rather than intermittent), pelvic pressure or pain, more pronounced urinary urgency, and potentially new flank pain from ureteral involvement. Some patients with MIBC at diagnosis have been symptomatic for many months but attributed their symptoms to benign causes.
Gender Differences in Bladder Cancer Symptom Recognition
Bladder cancer affects men three times more often than women, but this epidemiological fact has an unintended clinical consequence: hematuria in women is less likely to be immediately attributed to bladder cancer, leading to longer diagnostic delays. Multiple published studies have documented that women with bladder cancer are diagnosed at a more advanced stage than men with the same presenting symptoms, and that a greater proportion of female hematuria cases receive antibiotics as first-line treatment without imaging.
The reasons are not difficult to understand. Hematuria in women is far more commonly caused by UTI than in men — a single uncomplicated bacterial cystitis is common and easily recognized. Menstrual contamination can produce a false positive hematuria on urinalysis. And the symptom of dysuria and urgency — which in bladder CIS may represent the presenting feature — is among the most common gynecological and urological complaints in women, attributed to OAB, IC, urethral syndrome, or atrophic vaginitis. All of these realities make it easier to miss bladder cancer in women, not harder.
The standard of care is clear: any woman over 40 with gross hematuria not explained by confirmed bacterial infection, or with persistent irritative voiding symptoms without a UTI, should receive the same cystoscopy and CT urogram evaluation that a man with the same presentation would receive. Age and gender should not reduce the index of suspicion for urinary tract malignancy in the evaluation of hematuria.
Bladder Cancer Symptoms in Patients With Prior Pelvic Radiation
Patients who received pelvic radiation therapy — for prostate cancer, cervical cancer, rectal cancer, or other pelvic malignancies — face a unique challenge: radiation cystitis, a late side effect of pelvic radiation, produces hematuria and irritative voiding symptoms that can be clinically identical to bladder cancer symptoms. Radiation cystitis typically manifests 6 months to several years after radiation and reflects radiation-induced obliterative endarteritis of bladder blood vessels — producing friable, easily bleeding urothelium.
The clinical dilemma is that pelvic radiation also increases the risk of bladder cancer (urothelial carcinoma and occasionally sarcomas) by 2 to 4 times, with a latency period of 10 to 20 years. A patient with a history of pelvic radiation who develops hematuria may have radiation cystitis, bladder cancer, or both. The evaluation pathway is the same: cystoscopy and CT urogram. Cystoscopy in radiation cystitis shows diffuse telangectasias (dilated blood vessels) and mucosal friability; bladder cancer appears as a distinct lesion or flat erythematous area. These can coexist, and biopsies are taken from any suspicious area.
Patients with known radiation cystitis should not assume that new or worsening hematuria is simply a recurrence of their existing condition — any change in the pattern of hematuria (new onset, increased frequency, change in character) should prompt re-evaluation for secondary bladder malignancy.
Bladder Cancer Symptoms in Patients on Anticoagulants
Patients taking anticoagulants (warfarin, rivaroxaban, apixaban, dabigatran) who develop hematuria often have the bleeding attributed to their blood-thinning medication without further investigation. This is a clinical error. Anticoagulants lower the threshold at which an existing lesion bleeds — but they do not create lesions. A patient on anticoagulants who develops gross hematuria may be experiencing the first sign of a bladder tumor that the anticoagulation caused to bleed earlier than it would have otherwise. The AUA guideline is explicit: anticoagulant use does not eliminate the need for urothelial evaluation with cystoscopy and CT urogram. The evaluation should be performed in coordination with the prescribing clinician to ensure the anticoagulant is managed appropriately around the procedure.
Living With Bladder Cancer Symptom Surveillance
For patients already diagnosed with and treated for bladder cancer, the ongoing monitoring for recurrence creates a recurring psychological challenge: every 3 months (for year 1), a cystoscopy appointment approaches, bringing with it a surge of anxiety about whether the cancer has returned. This experience — sometimes called “surveillance anxiety” or “scanxiety” — is among the most consistently reported quality-of-life impairments in NMIBC patients, who may face this cycle for the rest of their lives.
Understanding that between-appointment symptoms can also signal recurrence helps patients stay vigilant without constant anxiety. The symptoms to watch for between scheduled cystoscopies:
- Any new gross hematuria, even a single episode — report and schedule an unplanned evaluation; do not wait for the next scheduled cystoscopy
- New irritative voiding symptoms (urgency, frequency, dysuria) more severe than before, or occurring where they were previously absent
- New pelvic discomfort, flank pain, or back pain
- New constitutional symptoms: significant unexplained weight loss, fatigue disproportionate to activity level
Surveillance-detected recurrences — found at a scheduled cystoscopy while still confined to the urothelium — are managed with TURBT and return to the surveillance schedule. Between-schedule recurrences that produce symptoms often present at a more advanced stage. Maintaining consistent surveillance while also staying attuned to interval symptoms gives bladder cancer patients the best chance of catching any recurrence at its earliest, most treatable stage.
Risk Factors That Raise the Suspicion Threshold
Knowing which patients are at highest risk for bladder cancer helps clinicians and patients themselves recognize when hematuria or irritative symptoms demand faster investigation:
Tobacco smoking is the single most important modifiable risk factor for bladder cancer, responsible for approximately 50 percent of cases in men and 30 percent in women. Cigarette smoke contains polycyclic aromatic hydrocarbons and aromatic amines that are excreted by the kidneys and concentrate in the urine, bathing the bladder urothelium in carcinogenic compounds for decades. The risk is dose-dependent and persists for 20 years or more after smoking cessation, though it declines substantially with time. Any smoker or former smoker with gross hematuria should be assumed to have bladder cancer until proven otherwise.
Occupational exposures to aromatic amines historically occurred in rubber, textile, paint, printing, and chemical manufacturing industries. Workers with these exposures — even from decades earlier, given the long latency of urothelial carcinogenesis — carry elevated lifetime risk. Occupational history should be taken in all patients evaluated for hematuria.
Cyclophosphamide exposure (a chemotherapy drug used for lymphoma, leukemia, and autoimmune conditions) causes a distinctive hemorrhagic cystitis during treatment due to the urotoxic metabolite acrolein, and it also carries a long-term risk of bladder cancer. Patients with a history of cyclophosphamide therapy represent a high-risk population in whom any hematuria requires bladder cancer evaluation.
Chronic indwelling urinary catheters and recurrent urinary tract infections — common in patients with spinal cord injuries or neurogenic bladder — are associated with squamous cell carcinoma of the bladder rather than the usual urothelial (transitional cell) carcinoma. Squamous cell carcinoma in this context is more often muscle-invasive at diagnosis because irritative symptoms and hematuria may be attributed to chronic catheter irritation for a long time before suspicion arises.
Aristolochic acid nephropathy, caused by herbs containing aristolochic acid (found in some traditional herbal supplements), causes both kidney injury and an exceptionally high rate of upper urinary tract urothelial carcinoma, with secondary bladder involvement. This is of particular concern for patients from East Asia and the Balkans who have used herbal remedies.
What Happens During a Bladder Cancer Evaluation Appointment
Many patients are uncertain about what to expect when they are referred to a urologist for hematuria evaluation. Understanding the typical sequence of events reduces anxiety and helps patients prepare for questions they will be asked:
The urologist will take a detailed history: the character and timing of the hematuria, smoking history, occupational exposures, prior urinary tract problems, any medications (especially anticoagulants and cyclophosphamide), and family history. A urinalysis is performed — if it shows bacterial infection, treatment is given and urinalysis is repeated after completion. Urine cytology is sent to evaluate for shed malignant cells. A CT urogram is ordered to examine the kidneys, ureters, and bladder — this requires an intravenous iodinated contrast injection, so patients with contrast allergies or impaired kidney function require special preparation or alternative imaging. Cystoscopy is then performed in the office under local anesthesia — a thin flexible camera is passed through the urethra into the bladder, and the entire bladder lining is visually inspected. The procedure typically takes 5–10 minutes. If a lesion is found, it is biopsied under general anesthesia in the operating room (TURBT). Most patients have CT urogram and cystoscopy completed within 2–4 weeks of referral — the entire diagnostic pathway from first hematuria to diagnosis typically spans 4–8 weeks at centers with good access.
The Bottom Line on Bladder Cancer Symptoms
Bladder cancer is one of the most common urological cancers, and it is also one of the most detectable at an early stage — but only if patients and clinicians respond appropriately to its earliest signals. A single episode of painless gross hematuria is enough. Persistent irritative voiding symptoms after negative UTI cultures are enough. Neither symptom should be explained away with antibiotics, watchful waiting, or reassurance without cystoscopy and upper tract imaging. The diagnostic tools exist, they work, and they can identify bladder cancer at a stage when it is confined to the lining of the bladder and curable with minimal treatment. The most common reason patients arrive at diagnosis with muscle-invasive or metastatic disease is not that their cancer was biologically aggressive from the start — it is that the earliest symptoms were not evaluated with sufficient urgency. That delay is the part of the bladder cancer story most worth changing.
For a full discussion of treatment approaches from TURBT to radical cystectomy to immunotherapy, visit our comprehensive bladder cancer guide. For kidney cancer symptom comparisons and the workup of upper tract hematuria, see our kidney cancer symptoms guide and our article on blood in urine and kidney cancer.