The human body contains approximately 60,000 miles of blood vessels — enough to circle the Earth more than twice. Laid end to end, they form a network that reaches every living cell in the body, delivering oxygen and nutrients while removing carbon dioxide and metabolic waste. Yet this vast network is not a uniform system of tubes. It is organized into three fundamentally different vessel types — arteries, capillaries, and veins — each with a distinct structure precisely matched to its function.
Understanding how these three types of blood vessels differ, what each one does, and how diseases affect them provides essential context for understanding blood pressure, cholesterol, heart disease, and nearly every other cardiovascular health topic. When a doctor talks about arterial stiffening, venous insufficiency, or capillary damage from diabetes, these are specific structural and functional changes in three different vessel categories that each have concrete consequences.
Arteries: The Pressure Vessels
Arteries carry blood away from the heart. In the systemic circulation, this means carrying oxygenated blood under high pressure to every organ and tissue in the body. The defining challenge for arteries is pressure — the left ventricle generates peak systolic pressures of 120 mmHg or more with each contraction. The arterial wall must withstand this pressure without rupturing while maintaining smooth, continuous forward flow to downstream organs.
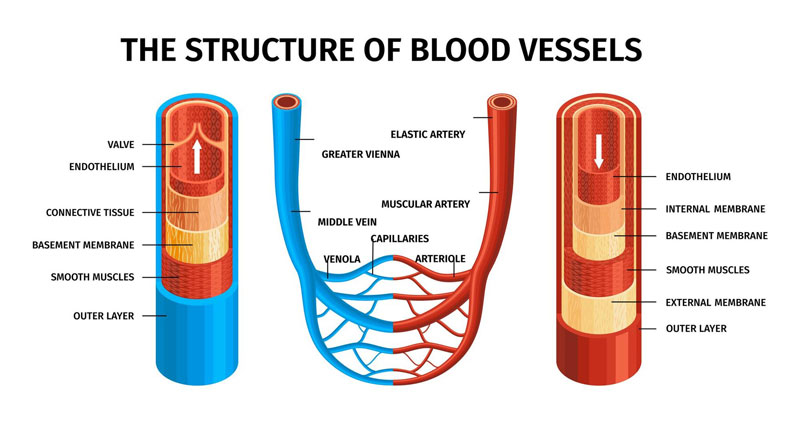
The Three-Layer Arterial Wall
All arteries and veins share a three-layer wall structure, though the relative thickness and composition of each layer varies dramatically by vessel type and location.
Tunica intima is the innermost layer, lining the vessel lumen. It consists of a single layer of endothelial cells resting on a basement membrane. The endothelium is far more than a passive lining — it is a metabolically active tissue that secretes nitric oxide (a potent vasodilator), prostacyclin (prevents platelet aggregation), and other vasoactive substances that continuously regulate blood flow. Healthy endothelium is the first line of defense against thrombosis and atherosclerosis. When damaged — by high blood pressure, oxidized LDL, cigarette smoke, or elevated blood glucose — this protective function is compromised, initiating the cascade that leads to arterial disease.
Tunica media is the middle and thickest layer in arteries. It consists of smooth muscle cells interspersed with elastic fibers and collagen. The smooth muscle controls vasoconstriction and vasodilation — the active changes in vessel diameter that regulate blood pressure and distribute flow to different organ beds. Sympathetic stimulation contracts smooth muscle (vasoconstriction); nitric oxide and parasympathetic stimulation promote relaxation (vasodilation).
Tunica adventitia is the outermost layer, composed primarily of collagen and elastic fibers. It provides structural support and anchors the vessel to surrounding connective tissue. In large arteries, the adventitia also contains the vasa vasorum — tiny blood vessels that feed the outer layers of the arterial wall itself.
Elastic Arteries: The Windkessel Effect
The largest arteries — the aorta, pulmonary trunk, and their major branches — are called elastic arteries because their tunica media contains abundant elastic fibers. This elasticity serves a critical function called the Windkessel effect. When the heart contracts, it ejects blood in a pulse — a rapid pressure wave. Rather than transmitting this sharp pulse directly to downstream vessels, the elastic aorta expands to absorb some of the kinetic energy. During diastole, the aorta recoils, pushing blood forward even while the heart is relaxing. This smooths the pressure wave, converting pulsatile flow from the heart into more continuous flow reaching downstream organs.
Arterial stiffening — which occurs naturally with aging as elastic fibers fragment and are replaced by collagen — raises systolic blood pressure while leaving diastolic pressure relatively unchanged: a stiffer aorta cannot absorb the systolic pulse wave as effectively, transmitting more pressure directly to downstream vessels.
Muscular Arteries and Arterioles
Muscular (distributing) arteries supply specific organs — femoral, renal, coronary, cerebral, and others. Their tunica media is dominated by smooth muscle rather than elastic tissue, giving them the ability to constrict or dilate substantially in response to neural and hormonal signals. The smallest arteries, called arterioles, are the master regulators of blood pressure. Small changes in arteriolar diameter produce large changes in resistance to blood flow. Total peripheral resistance — which together with cardiac output determines blood pressure — is primarily determined by arteriolar tone. The medications used to treat hypertension largely work by reducing arteriolar constriction.
The Coronary Arteries
The coronary arteries supply blood to the myocardium itself. The left anterior descending (LAD) artery supplies the anterior wall and interventricular septum; the left circumflex (LCx) supplies the lateral wall; the right coronary artery (RCA) supplies the inferior wall and, in most people, the sinoatrial and atrioventricular nodes.
One anatomical detail makes the coronary arteries unique: they are perfused primarily during diastole, not systole. During ventricular contraction, intramyocardial pressure compresses the coronary vessels within the heart muscle. During diastole, when the myocardium relaxes, coronary perfusion resumes. This is why tachycardia reduces coronary perfusion time and why conditions that reduce diastolic pressure can impair coronary blood flow.
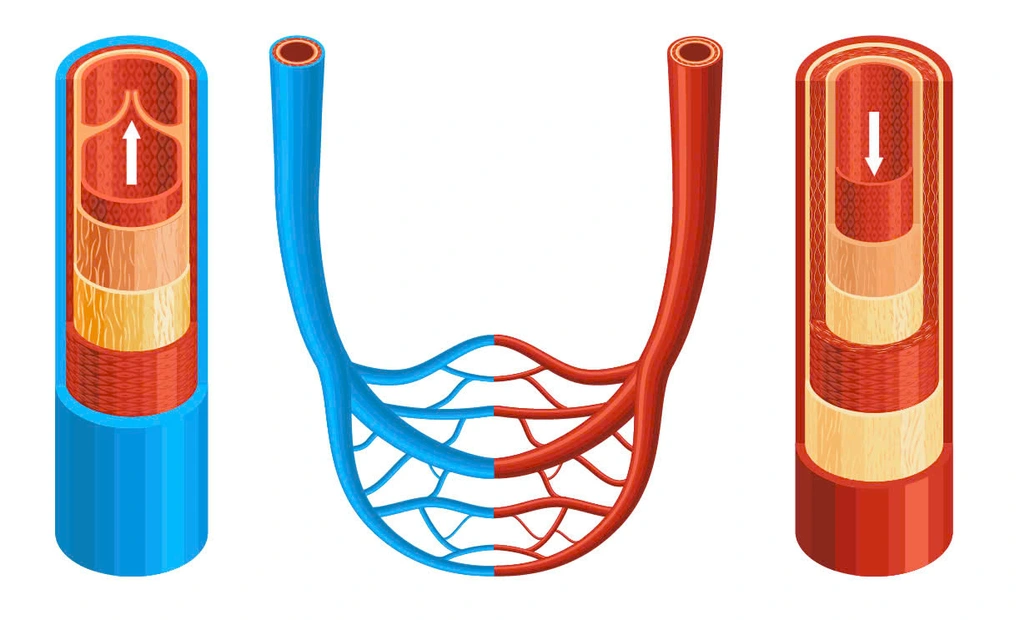
Capillaries: Where Exchange Happens
Capillaries are the smallest and most numerous blood vessels, and the only ones where the actual purpose of the circulatory system is fulfilled: the exchange of oxygen, carbon dioxide, nutrients, and waste products between blood and tissue cells. Every cell in the body is within approximately 100 micrometers of a capillary — close enough for oxygen to diffuse before the cells’ metabolic demands are unmet.
A capillary wall is remarkably thin — just a single layer of endothelial cells on a thin basement membrane, with a total wall thickness of approximately 0.5 to 1 micrometer. There is no tunica media or tunica adventitia. The lumen diameter (5 to 10 micrometers) is barely wider than a red blood cell (7 to 8 micrometers); red blood cells must deform to squeeze through, a requirement that actually enhances hemoglobin exposure to the capillary wall and facilitates gas exchange. Despite being individually tiny, the total capillary surface area in an adult human body is estimated at approximately 6,000 square meters.
Three Types of Capillaries
Continuous capillaries have endothelial cells connected by tight junctions, forming a nearly complete barrier. Small molecules (water, glucose, oxygen) can cross; most large molecules cannot. Found in muscle, skin, and lung. In the brain, continuous capillaries are supplemented by astrocyte foot processes to form the blood-brain barrier — the most restrictive capillary in the body.
Fenestrated capillaries have small pores in the endothelial cells that allow rapid exchange of water and small solutes. Found in tissues with high filtration or secretory demands: kidney glomeruli, intestinal villi, and endocrine glands.
Sinusoidal capillaries have large gaps between endothelial cells, allowing passage of large proteins and even blood cells. Found in the liver, bone marrow, and spleen — places where blood cells are produced, destroyed, or filtered.
Starling Forces: Fluid Movement at Capillaries
Fluid moves between the capillary and the interstitial space based on the balance between hydrostatic pressure (pushing fluid out) and oncotic pressure (pulling fluid in via plasma proteins, primarily albumin). At the arterial end of a capillary, hydrostatic pressure exceeds oncotic pressure and fluid is filtered out, carrying nutrients. At the venous end, hydrostatic pressure has fallen and fluid is partially reabsorbed. The lymphatic system picks up excess filtered fluid and returns it to the venous circulation. Disruption of these forces — by low albumin, elevated venous pressure in heart failure, or lymphatic obstruction — causes edema.
Veins: The Return System
Veins carry blood back to the heart under much lower pressure than arteries — typically 5 to 15 mmHg at the venule level versus 120/80 mmHg in the aorta. Their walls reflect this: the tunica media is thinner with less smooth muscle and fewer elastic fibers. This makes veins more compliant — they can accommodate large changes in blood volume with minimal change in pressure.
At rest, approximately 64 percent of the total circulating blood volume resides in the venous compartment. When the body needs to increase cardiac output rapidly — during exercise or hemorrhage — venoconstriction (sympathetic activation of venous smooth muscle) can rapidly shift this blood volume into the central circulation, increasing venous return.
Venous Valves and Return Mechanisms
Against gravity, blood in the leg veins must travel approximately 1.5 meters upward from the feet to the heart. Venous valves — crescent-shaped folds of tunica intima — are found in medium and large veins of the limbs, preventing backflow between contractions of the skeletal muscle pump. When leg muscles contract during walking, they compress surrounding veins and propel blood upward; when muscles relax, the valves close to prevent retrograde flow.
The respiratory pump provides a second mechanism: during inspiration, falling intrathoracic pressure draws blood into the thoracic vena cava and right atrium. Deep breathing during exercise facilitates venous return and cardiac output through this mechanism.
Deep and Superficial Veins
Veins in the limbs are organized into deep and superficial systems. Deep veins (femoral, popliteal, iliac) accompany the major arteries and carry the bulk of venous return — they are the primary site of deep vein thrombosis (DVT). Superficial veins (great saphenous, basilic, cephalic) lie in the subcutaneous tissue and are frequently used for IV access. Perforating veins connect the two systems with one-way valves; when venous valve function is lost, superficial veins become chronically dilated and tortuous: varicose veins.
What Ages Blood Vessels and What Protects Them
Blood vessels change throughout life. Arterial stiffening progresses as elastic fibers degrade and are replaced by collagen. Endothelial cells accumulate oxidative damage and produce less nitric oxide, creating a more pro-inflammatory, prothrombotic state. Atherosclerotic plaque builds in arterial walls over decades of exposure to LDL cholesterol, hypertension, and inflammatory signals. Venous valve function may deteriorate, particularly in people who spend long hours standing or sitting.
Modifiable factors strongly influence how quickly these changes occur. Blood pressure control protects the endothelium and reduces mechanical stress on arterial walls. LDL cholesterol management reduces the supply of the particle that initiates plaque formation. Not smoking removes one of the most potent direct chemical injurers of endothelial cells. Regular aerobic exercise generates shear stress on vessel walls that upregulates endothelial nitric oxide production — probably the most physiologically direct way to maintain vascular endothelial function. Blood glucose control protects the capillary endothelium from the glycation damage that underlies diabetic retinopathy, nephropathy, and neuropathy.
For a comprehensive overview of the numbers that track cardiovascular and vascular health, see our guide to heart health numbers every adult should know. For context on how blood pressure directly affects arterial structure and function, see our article on what blood pressure is and why it matters. For how cholesterol drives arterial disease, see our article on what cholesterol is and why it is important.
The American Heart Association provides patient-friendly resources on how the heart and blood vessels work. The NIH National Heart, Lung, and Blood Institute explains the structure and function of the cardiovascular system in depth. The CDC offers population-level data on heart and vascular disease prevalence and prevention.
Arteries, capillaries, and veins are not interchangeable tubes — each is an engineered solution to a different physiological problem. Understanding what each one does, how it is structured, and how disease disrupts its function turns the vocabulary of cardiovascular medicine from jargon into a coherent picture of how the circulatory system works and what it takes to keep it healthy.
The Vascular Spectrum: Arterial, Venous, and Capillary Disease
Understanding the three vessel types clarifies why cardiovascular disease takes so many different clinical forms. Arterial disease predominantly involves the accumulation of atherosclerotic plaque in the arterial intima — driven by high LDL cholesterol, hypertension, and endothelial injury. This process produces coronary artery disease, peripheral artery disease, carotid artery stenosis, and aortic aneurysm — all manifestations of the same underlying arterial pathology in different locations. The common thread is elevated LDL, endothelial damage, and the cascade from oxidized LDL to foam cells to plaque that takes decades to accumulate but can rupture in an instant.
Venous disease follows a different mechanism: valve dysfunction, venous stasis, and hypercoagulability drive deep vein thrombosis (DVT) and chronic venous insufficiency. Varicose veins result from superficial venous valve failure. Pulmonary embolism results when a deep venous clot breaks free and travels to the pulmonary circulation, where it can obstruct blood flow through the lungs. The risk factors for venous disease — prolonged immobility, dehydration, cancer, inherited clotting disorders, pregnancy — are largely different from those of arterial disease, reflecting the different pathophysiology. DVT prevention during long-haul travel or hospitalization involves compression stockings, hydration, anticoagulation in high-risk patients, and regular leg movement rather than cholesterol-lowering or blood pressure treatment.
Capillary disease — most prominently seen in diabetes — results from endothelial damage in the smallest vessels. Chronic hyperglycemia causes glycation of proteins, oxidative stress, and abnormal pericyte function in capillary walls. The consequences are microvascular: retinopathy (capillaries in the retina leak and proliferate abnormally), nephropathy (glomerular capillaries are damaged, causing proteinuria and progressive kidney failure), and peripheral neuropathy (capillaries supplying peripheral nerves are damaged, impairing nerve function). Good blood glucose control is primarily aimed at preventing capillary damage — the microvascular complications of diabetes that occur silently over years before manifesting as vision loss, kidney failure, or sensory loss in the feet.
Frequently Asked Questions About Blood Vessels
Do arteries always carry oxygenated blood?
In common usage, yes — but in anatomical terms, no. The defining characteristic of an artery is that it carries blood away from the heart, not that it carries oxygenated blood. The pulmonary arteries carry deoxygenated blood from the right ventricle to the lungs for oxygenation. Conversely, the pulmonary veins carry oxygenated blood from the lungs back to the left atrium — making them the only veins in the body that carry oxygenated blood.
Why do arteries not have valves while veins do?
Arteries maintain continuous forward flow because they operate under positive pressure from the heart throughout the cardiac cycle. There is no risk of retrograde flow in a vessel maintained under positive arterial pressure. Veins operate under much lower pressure, where gravity can cause retrograde flow in the limbs between heartbeats; valves prevent this. Large thoracic veins do not need valves because the pressure gradient from thoracic suction during inspiration is sufficient to ensure forward flow without valvular assistance.
How does exercise improve vascular health?
Regular aerobic exercise produces beneficial effects on blood vessels through several mechanisms. Increased blood flow during exercise generates shear stress on the endothelium, which upregulates eNOS (endothelial nitric oxide synthase) gene expression — meaning the endothelium produces more nitric oxide not just during exercise but at rest. This improves baseline endothelial function, reduces arterial stiffness, and lowers resting blood pressure over time. Exercise also reduces inflammatory markers associated with endothelial dysfunction and plaque progression, and the skeletal muscle pump action during exercise dramatically improves venous return.
What is the pulse you feel in your wrist?
The radial pulse at the wrist is the pressure wave generated by the left ventricle’s systolic ejection, transmitted through the elastic arterial tree to the radial artery. You are not feeling individual blood cells moving past — you are feeling the pressure wave that travels through the arterial wall at approximately 5 to 10 meters per second (much faster than the actual blood flow velocity, which is a few centimeters per second in large arteries). The pulse wave velocity — how fast this pressure wave travels — is an independent measure of arterial stiffness; stiffer arteries transmit the pulse wave faster.
Key Takeaways
- Three vessel types: arteries (away from heart, high pressure), capillaries (exchange), veins (toward heart, low pressure, high volume)
- Arterial walls have three layers (intima, media, adventitia); capillaries have only a single endothelial layer; veins have thinner media than arteries of comparable size
- Elastic arteries (aorta) smooth pulsatile flow via the Windkessel effect; arterioles control total peripheral resistance, which determines blood pressure
- Capillaries are the only site of gas and nutrient exchange; three types — continuous, fenestrated, sinusoidal — match different tissue exchange needs
- Veins hold approximately 64% of circulating blood volume; venous return to the heart depends on the skeletal muscle pump, respiratory pump, and venous tone
- Arterial disease = plaque (atherosclerosis); venous disease = stasis/thrombosis/valve failure; capillary disease = microangiopathy (primary concern in diabetes)
- Best vascular protectors: blood pressure control, LDL management, no smoking, regular aerobic exercise, blood glucose control
How Blood Vessels Are Assessed in Clinical Practice
Several non-invasive and minimally invasive tools allow clinicians to assess the structure and function of arteries, veins, and capillaries directly, providing objective evidence of vascular health that goes beyond standard blood tests.
Ankle-brachial index (ABI): The ratio of systolic blood pressure measured at the ankle to that measured at the arm. A normal ABI is 1.0 to 1.4; a value below 0.9 suggests peripheral artery disease (narrowed arteries in the legs due to atherosclerosis); values above 1.4 suggest arterial calcification. The ABI is a simple bedside test that has significant predictive value for overall cardiovascular risk — low ABI is a strong independent predictor of cardiovascular mortality, even in people without known heart disease.
Carotid intima-media thickness (CIMT): Ultrasound measurement of the thickness of the inner two layers (intima and media) of the carotid arteries. Increased CIMT reflects early subclinical atherosclerosis and is associated with higher cardiovascular risk. Used in research and in some clinical settings to refine cardiovascular risk assessment in intermediate-risk patients.
Venous Doppler ultrasound: Used to evaluate venous flow patterns and detect DVT, venous insufficiency, and venous valve incompetence. Compressibility of the vein is the primary criterion for ruling out DVT — a non-compressible vein indicates thrombus.
Coronary CT angiography (CTA): Uses contrast-enhanced computed tomography to visualize the coronary arteries and detect stenosis, plaque burden, and high-risk plaque features non-invasively. Provides information beyond the coronary calcium score, including the presence and composition of non-calcified plaque.
Pulse wave velocity (PWV): A direct measure of arterial stiffness — the speed at which the pressure wave generated by each heartbeat travels through the arterial tree. Higher PWV indicates stiffer arteries. PWV is an independent predictor of cardiovascular events and is increasingly used as a research and clinical endpoint for interventions targeting arterial stiffness.
These assessments complement standard risk factor measurement (blood pressure, cholesterol, glucose) by providing direct evidence of whether vascular changes have occurred — the anatomical and functional counterpart to the physiological numbers tracked by routine cardiovascular screening.