
Atherosclerosis is the disease behind the disease. Most heart attacks, most ischemic strokes, and most cases of peripheral artery disease are not independent conditions with independent causes — they are different consequences of the same underlying process: the slow, silent accumulation of lipid-rich plaques in the walls of large and medium-sized arteries. Atherosclerosis begins decades before it causes symptoms and is often far advanced by the time a first cardiac event occurs.
Understanding what atherosclerosis is — how it starts, how it progresses, and what determines whether it causes a sudden, life-threatening event — is one of the most important things a person can know about cardiovascular health. It explains why cholesterol management, blood pressure control, and smoking cessation reduce heart attack and stroke risk. And it explains what medicine can do to slow, stabilize, and in some cases partially reverse arterial disease before a catastrophic event occurs.
What Is Atherosclerosis?
Atherosclerosis is a chronic inflammatory disease of the arterial wall. The word derives from the Greek: athero (gruel or porridge) and sclerosis (hardening) — an apt description of the soft lipid-rich core and hardened fibrous exterior of a fully developed plaque. It affects large and medium-sized arteries and involves the progressive accumulation of lipids, immune cells, and fibrous connective tissue in the innermost layer of the arterial wall.
The defining feature of atherosclerosis is not simply fat accumulating in arteries — it is an active, dynamic inflammatory process involving multiple cell types, signaling molecules, and structural changes that unfold over decades. This distinction matters because it means atherosclerosis is not purely a consequence of dietary fat intake; it is driven by complex interactions between lipid abnormalities, endothelial injury, immune activation, and smooth muscle cell behavior.
How Atherosclerosis Develops — Six Stages
Stage 1: Endothelial Injury and Dysfunction
Atherosclerosis does not begin with lipid deposition — it begins with endothelial dysfunction. Healthy endothelium produces nitric oxide, maintains a non-thrombotic surface, and regulates the traffic of cells and molecules between blood and the arterial wall.
Endothelial dysfunction is initiated by several converging factors. Hemodynamic stress — particularly turbulent flow at arterial branch points and bifurcations — causes mechanical stress on endothelial cells. This is why atherosclerosis preferentially forms at the coronary artery branch points, the carotid bifurcation, and the aortic bifurcation. Elevated LDL cholesterol, especially small, dense, and oxidized LDL, causes direct chemical injury. Hypertension amplifies mechanical shear stress. Cigarette smoke delivers hundreds of chemical compounds that damage endothelial function. Hyperglycemia from diabetes causes protein glycation and oxidative stress in endothelial cells.
Dysfunctional endothelium produces less nitric oxide, upregulates adhesion molecules (VCAM-1, ICAM-1, selectins) that attract circulating monocytes, and becomes more permeable to LDL particles.
Stage 2: LDL Infiltration and Oxidation
As endothelial permeability increases, LDL particles cross from the bloodstream into the subendothelial space. Once within the intima, LDL is oxidized to form oxidized LDL (oxLDL) by reactive oxygen species from resident cells. This modification is critical: oxLDL cannot be cleared by normal LDL receptors and instead activates further inflammatory signaling, stimulates more adhesion molecule expression, and attracts more monocytes to the developing lesion.
Stage 3: Macrophage Infiltration and Foam Cell Formation
Monocytes adhere to the activated endothelium, migrate into the intima, and differentiate into macrophages. These macrophages express scavenger receptors — particularly SR-A and CD36 — that avidly engulf oxLDL without the downregulation feedback that limits normal LDL receptor uptake. Macrophages continue to take up oxLDL until they are engorged with lipid droplets, becoming foam cells. These foam cells release cytokines (IL-1β, TNF-α, IL-6), proteases, and reactive oxygen species that perpetuate and amplify the local inflammatory environment — a self-reinforcing cycle that drives continued plaque progression.
Stage 4: The Fatty Streak
The accumulation of foam cells beneath the endothelium creates the earliest visible atherosclerotic lesion: the fatty streak — a flat, yellow discoloration in the arterial intima. Fatty streaks are found in the aortas of children as young as three to five years of age and in the coronary arteries of adolescents. In early stages they are potentially reversible; with ongoing risk factors they progress.
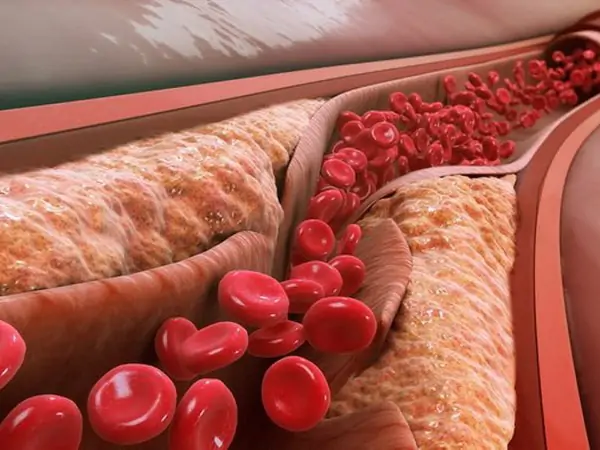
Stage 5: Fibrous Plaque Formation
As the lesion develops, smooth muscle cells from the tunica media migrate into the intima, proliferate, and secrete collagen. This collagen forms a fibrous cap over the lipid-rich necrotic core, creating an atherosclerotic plaque. The fibrous cap physically separates the pro-thrombotic contents of the lipid core from the flowing blood. A thick, collagen-rich fibrous cap is mechanically resistant and represents a stable plaque that can cause flow limitation but is unlikely to cause acute events. The structure of the fibrous cap — not the size of the plaque — is the primary determinant of acute event risk.
Stage 6: Vulnerable Plaque and Rupture
Vulnerable plaques are characterized by a large lipid-rich necrotic core, a thin fibrous cap (less than 65 micrometers), and dense macrophage infiltration at the plaque shoulder. Macrophages secrete matrix metalloproteinases (MMPs) that degrade collagen in the cap, thinning it and making it susceptible to mechanical disruption. A critically important and counterintuitive finding: the plaques most likely to rupture and cause acute events are not the most flow-limiting plaques — they are intermediate-sized, non-obstructive lesions with thin caps and large necrotic cores that would not even appear significant on a standard coronary angiogram.
When a vulnerable plaque ruptures, the lipid core — rich in tissue factor — is exposed to flowing blood. Tissue factor activates the coagulation cascade; platelets aggregate; a thrombus forms within seconds to minutes. A completely occlusive thrombus in a coronary artery causes a STEMI (ST-elevation myocardial infarction). A non-occlusive thrombus causes an NSTEMI or unstable angina.
A second mechanism — plaque erosion — involves loss of endothelial cells from the plaque surface without cap rupture, triggering thrombosis. Plaque erosion accounts for approximately 30 to 40 percent of acute coronary syndromes and is more common in younger patients and women.
Where Atherosclerosis Preferentially Develops
Atherosclerosis does not develop uniformly throughout the arterial tree. It preferentially affects sites of turbulent or oscillatory blood flow:
- Coronary arteries: proximal left anterior descending (LAD) is most commonly affected; supplies the anterior wall and apex of the left ventricle
- Carotid arteries: particularly the bifurcation and origin of the internal carotid; a major source of embolic ischemic stroke
- Aorta: especially the infrarenal segment; severe disease predisposes to aortic aneurysm
- Lower extremity arteries: superficial femoral artery is the most commonly affected segment in peripheral artery disease
- Renal arteries: ostial stenosis is the most common cause of atherosclerotic renovascular hypertension in older adults
Risk Factors and Their Mechanism
LDL cholesterol is the supply of the raw material that accumulates in arterial plaques. Each 1 mmol/L (~39 mg/dL) reduction in LDL is associated with approximately a 25 percent reduction in relative cardiovascular event risk in statin trials — the most robust pharmacological dose-response relationship in preventive cardiology.
Hypertension causes mechanical shear stress on endothelial cells, directly injuring the tunica intima and accelerating endothelial dysfunction. It also promotes smooth muscle proliferation and accelerates plaque rupture by increasing intraluminal pressure against the fibrous cap.
Cigarette smoking delivers hundreds of chemical compounds that damage endothelial cells, promote LDL oxidation, stimulate platelet aggregation, and increase fibrinogen levels — accelerating both plaque formation and thrombotic complications.
Diabetes causes chronic hyperglycemia that glycates LDL (making it more atherogenic), promotes endothelial dysfunction, and creates a pro-inflammatory, pro-thrombotic state. Insulin resistance drives atherogenic dyslipidemia: elevated triglycerides, low HDL, and elevated small dense LDL.
Lipoprotein(a) is an LDL-like particle with an additional apolipoprotein(a) protein. It is highly atherogenic and also promotes thrombosis by interfering with plasminogen activation. Lp(a) levels are genetically determined and do not respond to lifestyle changes — elevated Lp(a) is an independent cardiovascular risk factor that is underappreciated and under-screened in routine practice.
Can Atherosclerosis Be Reversed?
True plaque regression — a measurable reduction in plaque volume — is achievable with aggressive LDL lowering. Intravascular ultrasound (IVUS) imaging studies have demonstrated plaque volume regression in patients treated with high-intensity statins achieving LDL below 70 mg/dL. Adding PCSK9 inhibitors to achieve LDL levels well below 70 mg/dL produces even greater regression.
Clinically more important than volume reduction may be plaque stabilization: high-intensity statin therapy reduces the lipid core, increases fibrous cap thickness, reduces macrophage infiltration, and decreases inflammatory markers within plaques — all of which reduce rupture probability. These stabilization effects occur within months of starting treatment and precede measurable plaque volume reduction.
Prevention: The Evidence Base
The evidence for primary prevention rests on the same risk factor management that slows established disease: LDL control with statins (most evidence-based pharmacological intervention), blood pressure control to below 130/80 mmHg, smoking cessation (the fastest-acting intervention to reduce acute coronary event risk), Mediterranean dietary pattern (PREDIMED trial: ~30% reduction in major cardiovascular events in high-risk individuals), regular aerobic exercise (reduces LDL oxidation, improves endothelial function, raises HDL), and good glycemic control in diabetes.
For a detailed explanation of the cholesterol particles that drive atherosclerosis, see our article on what cholesterol is and why it is important. For the blood pressure mechanisms that accelerate endothelial injury, see our article on what blood pressure is and why it matters. For the underlying arterial structure where atherosclerosis develops, see our article on understanding arteries, veins, and capillaries.
The American Heart Association provides patient-oriented resources on atherosclerosis and coronary artery disease. The NIH National Heart, Lung, and Blood Institute offers in-depth information on atherosclerosis diagnosis, progression, and treatment. The CDC publishes data on coronary artery disease prevalence and prevention strategies.
Atherosclerosis is the silent architect of the majority of cardiovascular deaths in the modern world. Understanding it — as a process rather than a fixed anatomical lesion, as an inflammatory disease rather than simply a plumbing problem, and as one that begins in childhood and evolves over decades — fundamentally changes how cardiovascular risk should be understood and managed.
Atherosclerosis Symptoms: Why It Is Silent Until It Isn’t
The fundamental clinical challenge of atherosclerosis is that it produces no symptoms during the decades in which it is developing and progressing. The arterial lumen must narrow by approximately 70 percent before flow limitation is severe enough to cause exertional chest pain (stable angina). At lower levels of stenosis, blood flow at rest is unaffected; during exertion the demand exceeds supply, but often only just enough to cause symptoms the patient may attribute to deconditioning, indigestion, or musculoskeletal pain.
Acute symptoms — sudden chest pain, shortness of breath, arm or jaw pain, neurological symptoms of stroke — often represent the first clinical sign of atherosclerosis that has been present for 20 to 40 years. This is the fundamental argument for cardiovascular risk factor management in apparently healthy adults: by the time symptoms appear, the disease is advanced.
How Atherosclerosis Is Diagnosed
Several methods detect atherosclerosis before clinical events occur:
- Coronary artery calcium (CAC) score: CT scan detects calcified plaque in coronary arteries; a score above 100 indicates significant plaque burden; CAC scoring is the most evidence-supported tool for refining cardiovascular risk in intermediate-risk adults and guiding statin therapy initiation decisions
- Coronary CT angiography (CTA): visualizes both calcified and non-calcified plaque; provides information on stenosis severity and high-risk plaque features including low-attenuation plaque, positive remodeling, and spotty calcification
- Ankle-brachial index (ABI): ratio of ankle to arm systolic blood pressure; below 0.9 indicates peripheral artery disease; independently predicts cardiovascular mortality even in people without known heart disease
- Carotid intima-media thickness (CIMT): ultrasound measurement of arterial wall thickening; reflects generalized subclinical atherosclerotic burden
- Invasive coronary angiography: gold standard for defining coronary anatomy for revascularization; does not well characterize plaque volume or vulnerability — large non-obstructive plaques with rupture risk may appear insignificant on standard angiography
Frequently Asked Questions About Atherosclerosis
If atherosclerosis starts in childhood, is it inevitable?
The presence of early fatty streaks in childhood is nearly universal, but progression to clinically significant plaques is not. Progression depends on cumulative risk factor exposure over decades. Individuals who maintain low LDL, normal blood pressure, healthy weight, and never smoke throughout adulthood have dramatically lower atherosclerotic burden at any age than those who accumulate decades of exposure to multiple risk factors. Genetics matters, but modifiable factors determine the pace of disease progression far more than most people appreciate.
How is atherosclerosis different from arteriosclerosis?
Arteriosclerosis is a broader term referring to any stiffening or hardening of the arterial wall with aging, including simple loss of elasticity without plaque formation. Atherosclerosis is a specific type of arteriosclerosis involving inflammatory plaque in the intima. All atherosclerosis is arteriosclerosis; not all arteriosclerosis is atherosclerosis. The isolated systolic hypertension of older adults, driven by arterial stiffening without significant plaque, is technically arteriosclerosis but not necessarily atherosclerosis.
Can atherosclerosis cause symptoms other than heart attack and stroke?
Yes. Atherosclerosis in the coronary arteries causes stable angina (exertional chest pain from reversible ischemia) before it causes myocardial infarction. In the carotid arteries, it causes transient ischemic attacks (TIAs) — brief episodes of neurological dysfunction that serve as warning events before ischemic stroke. In the lower extremity arteries, it causes claudication (reproducible calf or thigh pain with walking that resolves with rest), critical limb ischemia, and in severe cases, limb-threatening gangrene. In the renal arteries, it causes renovascular hypertension and ischemic nephropathy. The manifestation depends entirely on which arterial bed is most affected.
What is the relationship between inflammation and atherosclerosis?
Inflammation is central to every stage of atherosclerosis — from the initial endothelial activation that allows LDL infiltration, to the macrophage-driven foam cell formation, to the MMP-mediated cap thinning that precedes plaque rupture, to the systemic inflammatory state associated with elevated cardiovascular risk. This is why high-sensitivity CRP (hsCRP) — a systemic marker of inflammation — is an independent predictor of cardiovascular events. The JUPITER trial demonstrated that rosuvastatin reduced cardiovascular events even in patients with low LDL but elevated hsCRP, suggesting inflammatory risk independent of LDL. Colchicine — an anti-inflammatory drug — has also shown cardiovascular event reduction in recent trials (COLCOT, LoDoCo2), providing direct evidence that targeting inflammation in atherosclerosis produces clinical benefit beyond LDL lowering.
Key Takeaways
- Atherosclerosis is a chronic inflammatory disease of the arterial intima — not simply lipid accumulation
- It begins in childhood with fatty streaks and progresses silently over decades before causing symptoms
- Six stages: endothelial dysfunction → LDL infiltration → macrophage foam cells → fatty streak → fibrous plaque → vulnerable plaque
- Vulnerable plaques (thin cap + large lipid core + macrophage infiltration) cause most acute events — not the largest, most flow-limiting plaques
- Plaque rupture exposes tissue factor → thrombus → MI or stroke within minutes
- Each 1 mmol/L LDL reduction → approximately 25% relative cardiovascular event reduction (statin trials)
- True plaque regression is achievable with aggressive LDL lowering; plaque stabilization (thicker cap, smaller lipid core) precedes volume regression
- PREDIMED trial: Mediterranean diet reduced major cardiovascular events by ~30% in high-risk adults
- Atherosclerosis is measurable before events occur: coronary calcium score, CTA, ABI are useful non-invasive tools
Atherosclerosis and Coronary Calcium Scoring: A Closer Look
The coronary artery calcium (CAC) score deserves special attention because it has become one of the most clinically actionable tools for detecting subclinical atherosclerosis in adults who do not yet have symptoms. The test uses a non-contrast CT scan to detect and quantify calcified plaque in the coronary arteries. Calcification is a late-stage feature of plaque development — it does not indicate instability, but it does indicate that significant atherosclerosis has occurred and has been present long enough to calcify.
A CAC score of zero (no detectable calcified plaque) is associated with a very low 10-year cardiovascular event rate — in the range of 1 to 2 percent even in patients with other risk factors. A score of zero can appropriately be used to defer statin initiation in intermediate-risk patients who are uncertain about starting medication, as it substantially reassigns them to lower risk. A score above 100 indicates significant plaque burden and generally supports initiating or intensifying preventive treatment regardless of calculated risk. A score above 400 indicates very high plaque burden and is associated with event rates comparable to those of patients with established coronary artery disease.
The CAC score provides risk information orthogonal to standard risk factors — it represents the actual anatomical consequence of lifetime exposure to those risk factors rather than just the risk factors themselves. Two patients with identical LDL, blood pressure, and smoking history may have dramatically different CAC scores, reflecting differences in genetic susceptibility, duration of risk factor exposure, and other unmeasured variables. This direct anatomical signal makes CAC a particularly powerful tool for personalizing treatment decisions in the 40–75 age range.
The Role of Anti-Inflammatory Therapy in Atherosclerosis
Given that inflammation drives every stage of atherosclerosis, targeting inflammation independently of LDL lowering has become an active therapeutic strategy. Two landmark trials have demonstrated that anti-inflammatory treatment reduces cardiovascular events in patients with established coronary artery disease:
The COLCOT trial (2019) randomized 4,745 patients who had recently experienced a myocardial infarction to colchicine 0.5 mg daily or placebo. Colchicine reduced the primary composite of cardiovascular death, MI, stroke, and urgent coronary revascularization by approximately 23 percent over a median follow-up of 22 months. This was in patients who were already on optimal background therapy with statins and antiplatelet agents.
The LoDoCo2 trial (2020) randomized 5,522 patients with stable coronary artery disease to colchicine 0.5 mg daily or placebo. Colchicine reduced the rate of the primary outcome (cardiovascular death, MI, ischemic stroke, or ischemia-driven coronary revascularization) by 31 percent. These results confirmed that the residual inflammatory risk in coronary artery disease patients — not adequately addressed by LDL lowering alone — can be meaningfully reduced with targeted anti-inflammatory therapy.
These trials do not change the primacy of LDL management but add a new dimension to secondary prevention: the recognition that atherosclerosis is an inflammatory disease means it may be amenable to treatment strategies that target the immune cell activity driving plaque progression and instability, independent of lipid pathways.
Atherosclerosis is ultimately a disease of lifelong risk factor accumulation that manifests as a series of preventable events. The science of plaque biology, plaque detection, and plaque stabilization has advanced remarkably over the past three decades — providing both tools to measure subclinical disease before events occur and treatments capable of slowing, stabilizing, and in some patients reversing the arterial changes that took decades to develop. The practical implication for any adult is the same: the earlier and more aggressively cardiovascular risk factors are managed, the lower the burden of atherosclerosis at any given age, and the lower the probability of being on the wrong side of a vulnerable plaque rupture.