Coronary artery disease is the most common form of heart disease and the leading cause of death in the United States and worldwide. Approximately 18.2 million adults in the United States are living with coronary artery disease, and approximately 805,000 Americans experience a heart attack each year — one every 40 seconds. Yet despite its prevalence, coronary artery disease remains widely misunderstood: many people believe it develops suddenly in late life, requires no intervention until symptoms appear, or affects only men. None of these assumptions are accurate.
Coronary artery disease is almost always the clinical expression of atherosclerosis in the coronary arteries — a process that begins decades before any symptoms develop and progresses in ways substantially influenced by modifiable risk factors. Understanding what coronary artery disease is, how it causes the symptoms and events it does, and what medicine can do to diagnose, treat, and prevent it is essential for any adult managing cardiovascular health.
What Is Coronary Artery Disease?
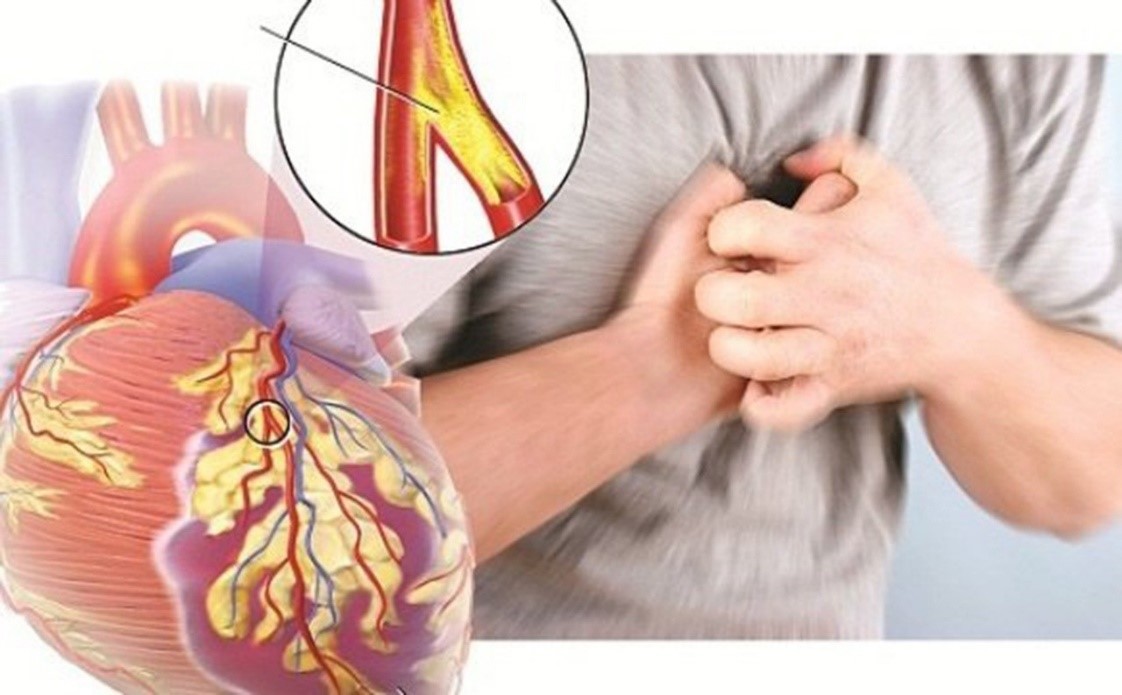
Coronary artery disease is the narrowing or obstruction of the coronary arteries — the vessels that supply oxygenated blood directly to the heart muscle (myocardium). The heart contracts approximately 100,000 times per day and requires a constant supply of oxygen and nutrients. Unlike skeletal muscle, which can tolerate brief periods of oxygen deprivation, cardiac muscle begins to die within 20 to 40 minutes of complete ischemia — making coronary occlusion one of the most time-sensitive emergencies in medicine.
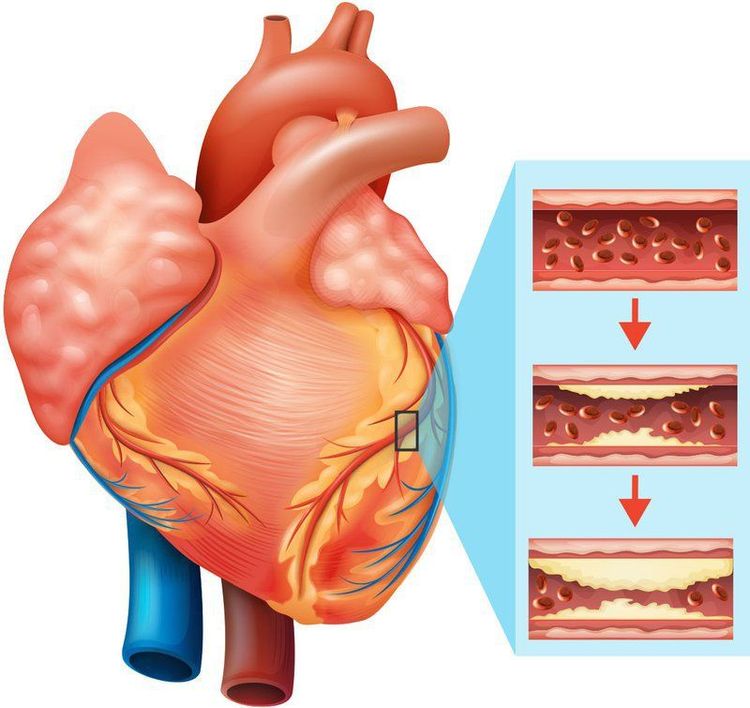
In coronary artery disease, atherosclerotic plaque accumulates in the walls of the coronary arteries over years and decades, progressively narrowing the lumen and reducing blood flow capacity. The consequences range from no symptoms (in early or mild disease) to exertional chest pain (in moderate disease) to sudden death from acute myocardial infarction (in severe disease with plaque rupture).
How Coronary Artery Disease Causes Symptoms
Stable Angina
Stable angina occurs when a coronary artery has narrowed by approximately 70 percent or more. At rest, blood supply is still adequate. During physical exertion, emotional stress, or cold exposure — conditions that increase the heart’s oxygen demand — supply cannot keep pace with demand, producing myocardial ischemia.
The classic symptom is substernal chest pressure or tightness that may radiate to the left arm, jaw, neck, or back — often accompanied by shortness of breath and diaphoresis. Stable angina is characteristically predictable: it occurs at a consistent threshold of exertion, lasts 2 to 10 minutes, and resolves promptly with rest or sublingual nitroglycerin.
Not all stable angina presents classically. Women, patients with diabetes (whose autonomic neuropathy may blunt pain perception), and older adults are more likely to experience atypical symptoms: jaw pain, epigastric discomfort, fatigue, or exertional dyspnea without chest pain. These presentations are frequently misattributed to non-cardiac causes, delaying appropriate evaluation.
Acute Coronary Syndromes
Acute coronary syndromes (ACS) occur when a coronary plaque ruptures or erodes, triggering thrombus formation that acutely reduces or completely obstructs blood flow. Unlike stable angina — driven by the chronic degree of stenosis — ACS is driven by the acute instability of a plaque.
STEMI (ST-elevation myocardial infarction) results from complete coronary occlusion by thrombus. Myocardial cells begin dying within 20 to 40 minutes; extensive damage may be irreversible by 6 hours. Every minute of delay from symptom onset to reperfusion represents additional myocardial loss — hence the target of door-to-balloon time within 90 minutes.
NSTEMI (non-ST elevation MI) results from a partial, non-occlusive thrombus. Blood flow is severely reduced but not completely interrupted. Some myocardial cells die (reflected by troponin elevation), but the infarct is not transmural.
Unstable angina is characterized by new-onset angina, angina at rest, or a significant worsening of previously stable angina. Biomarkers (troponin) are not elevated, but the unstable plaque carries high short-term risk of progressing to STEMI.
Approximately 20 to 30 percent of myocardial infarctions produce no classic symptoms — this is called silent MI. Silent MI is more common in women, elderly adults, and individuals with diabetes. Despite the absence of symptoms, silent MI carries the same long-term prognostic implications as symptomatic MI.
The Three Coronary Arteries
Left Anterior Descending (LAD): supplies the anterior wall and apex of the left ventricle and the anterior interventricular septum. Proximal LAD occlusion before its major septal branches affects a large territory and is historically called the “widowmaker” for its high mortality if not reperfused rapidly.
Left Circumflex (LCx): supplies the lateral wall of the left ventricle. In the approximately 15% of patients with a dominant LCx, it also supplies the inferior wall and the SA/AV nodes.
Right Coronary Artery (RCA): in approximately 70% of adults (right-dominant circulation), supplies the inferior wall of the left ventricle, the right ventricle, the SA node, and the AV node. Inferior STEMI from RCA occlusion can cause bradycardia, heart block, and right ventricular infarction with very different hemodynamic implications than anterior MI.
Diagnosing Coronary Artery Disease
Functional Testing
- Exercise stress test (EST): treadmill ECG monitoring; sensitivity ~68%, specificity ~77% for obstructive CAD; preferred when resting ECG is normal and patient can exercise
- Stress echocardiography: identifies regional wall motion abnormalities from ischemia; higher sensitivity and specificity than ECG alone; also assesses valve function and LV function
- Nuclear perfusion imaging (SPECT/PET): regional perfusion defects indicate ischemia or scar; can quantify the percentage of myocardium at risk
Anatomic Testing
- Coronary CT angiography (CTA): non-invasive; excellent negative predictive value (>99%) for ruling out significant coronary stenosis; characterizes plaque type beyond stenosis severity
- Invasive coronary angiography (ICA): gold standard for defining coronary anatomy; fractional flow reserve (FFR ≤0.80) can assess whether a given stenosis is physiologically significant before stenting
Medical Treatment of Coronary Artery Disease
Antiplatelet therapy: aspirin 75–100 mg daily for all established CAD. After ACS or PCI, dual antiplatelet therapy (aspirin + a P2Y12 inhibitor: clopidogrel, ticagrelor, or prasugrel) for 6–12 months prevents stent thrombosis and recurrent events.
High-intensity statins: indicated for all CAD patients regardless of baseline LDL. Target LDL below 70 mg/dL for most; below 55 mg/dL for very high-risk patients. Statins also stabilize plaques, reduce inflammation, and improve endothelial function.
Beta-blockers: reduce heart rate and myocardial oxygen demand; provide mortality benefit post-MI (particularly with reduced ejection fraction) and symptom relief in stable angina.
ACE inhibitors or ARBs: reduce cardiac remodeling post-MI; recommended in all post-MI patients, particularly those with reduced ejection fraction, hypertension, or diabetes.
Nitrates: sublingual nitroglycerin for acute angina; long-acting nitrates for prophylaxis in patients with frequent angina. Nitrate-free periods are recommended to prevent tolerance.
Revascularization: PCI and CABG
PCI (Percutaneous Coronary Intervention) involves balloon angioplasty and drug-eluting stent deployment. It is the treatment of choice for STEMI (door-to-balloon ≤90 minutes) and for high-risk NSTEMI. For stable CAD, PCI provides symptom relief but does not reduce MI or mortality in patients with stable single-vessel disease on optimal medical therapy.
CABG (Coronary Artery Bypass Graft Surgery) creates new routes for blood flow to the myocardium using internal mammary artery and saphenous vein grafts. CABG is preferred over PCI for left main coronary artery disease, multivessel disease in patients with diabetes, three-vessel disease with complex anatomy, or multivessel disease with significantly reduced left ventricular function — scenarios where CABG provides more complete revascularization and better long-term survival.
Secondary Prevention After CAD Diagnosis
A CAD diagnosis initiates lifelong secondary prevention. High-intensity statins, antiplatelet therapy, blood pressure control (target <130/80 mmHg), and ACE inhibition are the pharmacological pillars. Cardiac rehabilitation reduces all-cause mortality by approximately 20 percent and is recommended for all post-MI patients. Smoking cessation reduces recurrent event risk by 30 to 50 percent within the first year — the fastest modifiable intervention available. Depression following MI independently predicts worse outcomes and should be screened for and treated in comprehensive cardiac care.
For a detailed explanation of the atherosclerosis process that underlies CAD, see our article on what is atherosclerosis. For the cholesterol management strategies central to CAD prevention and treatment, see our article on what cholesterol is and why it is important. For the blood pressure management that reduces both CAD progression and acute event risk, see our article on what blood pressure is and why it matters.
The American Heart Association provides comprehensive patient resources on heart attack recognition, treatment, and prevention. The NIH National Heart, Lung, and Blood Institute offers evidence-based information on coronary heart disease diagnosis and management. The CDC publishes data on coronary artery disease prevalence, mortality, and prevention.
Coronary artery disease is serious and life-threatening — but it is not inevitable, not untreatable, and not beyond the reach of prevention. The same risk factors that drive atherosclerosis in the coronary arteries are modifiable, and the interventions that modify them substantially reduce the risk of the events that make coronary artery disease so deadly.
Coronary Artery Disease in Women: The Diagnostic Gap
CAD in women has historically been underdiagnosed, undertreated, and underrepresented in clinical trials. Several factors contribute. First, women present with atypical symptoms more frequently than men — fatigue, dyspnea, nausea, jaw pain, and back pain rather than classic substernal chest pressure. These symptoms are more often attributed to anxiety, gastrointestinal problems, or musculoskeletal conditions. Second, women develop CAD approximately 7 to 10 years later than men on average, with estrogen providing relative cardiovascular protection through its effects on endothelial function and lipid metabolism before menopause. Third, certain CAD variants — including spontaneous coronary artery dissection (SCAD), microvascular angina, and plaque erosion rather than rupture — are more common in women and may not show clearly on coronary angiography designed to detect stenosis.
The clinical consequence is that women experiencing ACS are more likely to have longer symptom-to-presentation times and to receive less timely and less aggressive treatment than men with similar presentations. Current guidelines now explicitly address sex-specific considerations in CAD diagnosis and management, recognizing that equal care requires accounting for these biological and presentation differences.
Life After a Heart Attack: What Recovery Looks Like
Recovery from myocardial infarction involves several overlapping phases. In the immediate hospital phase (days 1–3), treatment focuses on reperfusion, hemodynamic stabilization, and initiation of guideline-directed medical therapy — statins, dual antiplatelet therapy, beta-blockers, and ACE inhibitors. Early mobilization is encouraged when clinically appropriate.
The post-discharge phase (weeks 1–6) involves medication adjustment, gradual return to activity, and enrollment in cardiac rehabilitation. The first 30 days after MI carry the highest risk of recurrent events — strict adherence to medications and avoidance of strenuous activity without clearance is essential during this period.
The long-term phase (months to years) centers on lifelong secondary prevention: maintaining LDL targets, blood pressure targets, antiplatelet therapy, and lifestyle modifications. Cardiac rehabilitation, if completed, improves exercise capacity, reduces anxiety and depression, and reduces mortality by approximately 20 percent. Most patients can return to prior levels of activity and work within 4 to 6 weeks after uncomplicated MI with appropriate medical clearance.
Frequently Asked Questions About Coronary Artery Disease
Can coronary artery disease be reversed?
Established structural narrowing of coronary arteries cannot be physically reversed by lifestyle or medication — the plaque does not disappear. However, atherosclerosis progression can be arrested and plaques can be stabilized, reducing the risk of rupture. High-intensity statin therapy has been shown to cause measurable regression of plaque volume on IVUS imaging. The clinical priority after CAD diagnosis is not reversal of existing anatomy but prevention of acute events — which is achievable through optimal medical therapy and risk factor control.
What is the difference between angina and a heart attack?
Angina is reversible myocardial ischemia — the heart muscle is oxygen-deprived but not dying. Angina symptoms resolve within minutes when demand drops (rest) or blood flow improves (nitroglycerin). A heart attack (MI) involves irreversible myocardial cell death — the blood supply is completely or nearly completely interrupted long enough for cells to die. If chest pain does not resolve within 10–15 minutes with rest and nitroglycerin, emergency evaluation is needed immediately.
What triggers a heart attack if atherosclerosis develops slowly over decades?
The acute trigger is plaque rupture or erosion — the sudden instability of a previously stable plaque, followed by thrombus formation within minutes. Triggers that can precipitate plaque rupture include intense physical exertion (particularly in sedentary people), severe emotional stress, systemic inflammation from infection, cocaine or stimulant use, cold exposure, and early morning hours (when sympathetic tone and blood pressure are highest). This is why MI clusters in the early morning hours, on Mondays, and in winter months in population-level data.
What is the SYNTAX score and why does it matter for treatment decisions?
The SYNTAX score is a grading system that quantifies the complexity of coronary artery disease based on the number of coronary lesions, their location, and specific lesion characteristics (bifurcation involvement, total occlusion, calcification, etc.). A higher SYNTAX score indicates more complex, anatomically difficult coronary disease. In multiple clinical trials, patients with high SYNTAX scores had better outcomes with CABG than with PCI — the score is now routinely used in multidisciplinary heart team discussions to guide the choice between PCI and bypass surgery in patients with multivessel disease.
Key Takeaways
- CAD = atherosclerotic narrowing of coronary arteries; the most common cause of death globally
- Two mechanisms: chronic demand ischemia (stable angina from ≥70% stenosis) and acute supply failure (ACS from plaque rupture + thrombus)
- STEMI = complete occlusion; door-to-balloon time ≤90 minutes is the target; every minute of delay = more myocardial loss
- Women more often present atypically (fatigue, dyspnea, jaw pain); diagnosis is frequently delayed
- Primary treatment: high-intensity statins, antiplatelet therapy, beta-blockers, ACE inhibitors, risk factor control
- PCI preferred for STEMI and some high-risk ACS; CABG preferred for left main, multivessel disease with diabetes, complex 3-vessel disease
- Cardiac rehabilitation after MI reduces mortality ~20%; smoking cessation reduces recurrent events 30–50%
- Secondary prevention after a CAD diagnosis is lifelong — the diagnosis is not an endpoint but the beginning of a structured, evidence-based risk reduction program
Risk Factors for Coronary Artery Disease
CAD shares its risk factors with atherosclerosis, because CAD is atherosclerosis in the coronary arteries. The risk factors can be divided into major modifiable risk factors — those that respond directly to lifestyle and medical intervention — and non-modifiable risk factors that inform risk assessment but cannot be changed.
Major modifiable risk factors:
- LDL cholesterol: the primary modifiable driver; each 39 mg/dL (~1 mmol/L) LDL reduction from statin therapy reduces relative cardiovascular event risk by ~25%
- Hypertension: doubles CAD risk at sustained levels above 140/90 mmHg; even Stage 1 hypertension (130–139/80–89) is associated with meaningfully higher risk
- Cigarette smoking: increases CAD risk 2–4 times; dose-dependent; risk begins to fall within weeks of cessation
- Diabetes: 2–4 times higher CAD risk; treats the disease as equivalent to having established CAD in many risk frameworks
- Physical inactivity: associated with 1.5–2 times higher CAD risk; exercise reduces risk through multiple mechanisms
- Obesity: particularly central adiposity; raises blood pressure, LDL, glucose, and inflammatory markers simultaneously
- Low HDL cholesterol: independently associated with increased CAD risk; low HDL is a component of atherogenic dyslipidemia
Non-modifiable risk factors:
- Age: risk increases progressively; majority of CAD events occur after age 60
- Male sex / post-menopausal female: men have higher CAD rates at younger ages; women’s risk approaches men’s after menopause
- Family history: premature CAD in a first-degree relative (father/brother before 55; mother/sister before 65) is a significant independent risk factor, reflecting genetic variants in LDL metabolism, inflammatory response, and plaque biology
- Elevated lipoprotein(a): genetically determined; levels >50 mg/dL are associated with substantially higher CAD risk; not responsive to lifestyle changes
Understanding Your Coronary Risk
The ACC/AHA Pooled Cohort Equations estimate 10-year risk of a major atherosclerotic cardiovascular event (MACE) — defined as nonfatal MI, nonfatal stroke, or cardiovascular death. The calculator uses age, sex, race, total cholesterol, HDL cholesterol, systolic blood pressure, treatment status, diabetes status, and smoking status. A 10-year MACE risk below 5% is considered low; 5–7.5% is borderline; 7.5–20% is intermediate; above 20% is high.
For patients in the borderline to intermediate risk range (5–20% 10-year risk), additional testing can refine treatment decisions. Coronary artery calcium (CAC) scoring is the most evidence-supported risk-enhancing tool in this range: a CAC score of zero substantially lowers risk in an intermediate-risk patient (can defer statin initiation); a CAC score above 100 elevates it (supports statin initiation). Other risk-enhancing factors recognized in current guidelines include elevated Lp(a), elevated hsCRP, ankle-brachial index below 0.9, and metabolic syndrome.
For very high-risk patients — those with established ASCVD (prior MI, stroke, or established PAD) — the risk calculator is not needed because the decision to use high-intensity statin therapy and aspirin is already evidence-based and guideline-supported. Risk stratification tools are most valuable in the primary prevention setting, where the decision about when to start medication involves weighing benefits against long-term side effect exposure.
Coronary Artery Disease and Mental Health
The relationship between CAD and mental health is bidirectional and clinically significant. Depression is present in approximately 20 to 30 percent of patients following a myocardial infarction — three times the prevalence in the general adult population. Post-MI depression independently predicts worse cardiovascular outcomes: increased risk of recurrent MI, higher all-cause mortality, reduced adherence to medications and rehabilitation programs, and poorer quality of life. The mechanisms are multiple: depression activates the hypothalamic-pituitary-adrenal axis (raising cortisol and sympathetic tone), promotes platelet hyperreactivity, and generates systemic inflammation — all of which increase the risk of acute plaque events.
Anxiety is also common after a cardiac event, often manifesting as health anxiety about symptoms (fear that any chest sensation is a warning of another heart attack) and avoidance of physical activity — the opposite of the recommended cardiac rehabilitation approach. Comprehensive cardiac care programs include mental health screening and access to psychological support as standard components, recognizing that successful secondary prevention requires not just pharmacological and behavioral intervention but addressing the psychological impact of what is often a life-altering event.
For patients and families navigating a CAD diagnosis, the key message is that effective treatment is available, the evidence base for risk reduction is strong, and survival after MI — with appropriate secondary prevention — is substantially better today than it was even two decades ago. CAD is a chronic condition requiring ongoing management, not a terminal sentence.
Advances in cardiology over the past three decades have transformed coronary artery disease from a near-inevitably fatal condition to a highly manageable chronic disease for most patients. High-sensitivity troponin assays detect myocardial injury earlier and more precisely. Coronary CTA allows non-invasive plaque characterization. PCSK9 inhibitors achieve LDL reductions of 50 to 60 percent beyond statins. Newer antiplatelet agents reduce stent thrombosis rates below one percent. These advances make early detection and guideline-directed therapy more powerful than ever before — and underscore why regular risk assessment and timely intervention matter so much.