Heart Failure: Symptoms, Causes, and Monitoring
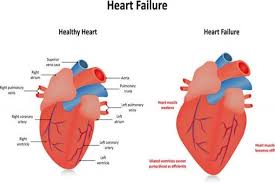
Heart failure is a clinical syndrome in which the heart cannot pump enough blood to meet the body’s metabolic demands, or can do so only at the cost of abnormally elevated filling pressures. It is not a disease in itself but rather the final common pathway of many cardiac and non-cardiac conditions — coronary artery disease, hypertension, valvular disease, cardiomyopathies, and others — that progressively impair the heart’s ability to function as an effective pump. It affects approximately 6.7 million Americans and is the leading cause of hospitalization in adults over age 65, with 1 million new diagnoses each year and a 5-year mortality rate comparable to many common cancers.
Despite its severity, heart failure is a condition in which the right management makes a dramatic difference in both survival and quality of life. The pharmacological toolkit for heart failure with reduced ejection fraction is among the most evidence-supported in all of cardiology — multiple drug classes have demonstrated 20 to 40 percent mortality reductions in randomized trials, and patients who receive optimal medical therapy can live for years or decades with well-controlled symptoms and acceptable function. Understanding heart failure — its types, symptoms, causes, and the monitoring practices that keep patients stable — is essential for the millions of Americans living with this condition and the family members who support them.
The Two Main Types of Heart Failure — HFrEF and HFpEF
Heart failure is classified into two primary phenotypes based on the left ventricular ejection fraction (LVEF) — the percentage of blood ejected from the left ventricle with each heartbeat, measured by echocardiography:
Heart failure with reduced ejection fraction (HFrEF) — historically called systolic heart failure — is defined as LVEF below 40 percent. The heart muscle contracts weakly and ejects insufficient blood with each beat, leading to reduced cardiac output and compensatory mechanisms (elevated heart rate, neurohormonal activation) that ultimately prove harmful if sustained. HFrEF most commonly results from coronary artery disease (prior myocardial infarction destroying myocardium), dilated cardiomyopathy (diffuse myocardial weakening from various causes), or longstanding uncontrolled hypertension or valvular disease. HFrEF has the largest evidence base for pharmacological treatment — four drug classes have demonstrated mortality benefit: ACE inhibitors/ARBs or ARNIs (sacubitril-valsartan), beta-blockers, mineralocorticoid receptor antagonists (spironolactone, eplerenone), and SGLT2 inhibitors (empagliflozin, dapagliflozin).
Heart failure with preserved ejection fraction (HFpEF) — historically called diastolic heart failure — is defined as LVEF 50 percent or above, with symptoms and signs of heart failure and evidence of abnormal cardiac filling pressures or diastolic dysfunction. In HFpEF, the heart muscle contracts normally (normal or near-normal LVEF) but is stiff and does not relax properly during diastole, requiring higher pressures to fill the ventricle. This elevated filling pressure backs up into the pulmonary circulation, causing pulmonary congestion and dyspnea. HFpEF is strongly associated with hypertension, obesity, diabetes, atrial fibrillation, and advancing age, and is now the most prevalent heart failure phenotype in developed countries. SGLT2 inhibitors (empagliflozin in the EMPEROR-Preserved trial, dapagliflozin in the DELIVER trial) are the first drug class to demonstrate significant cardiovascular outcome reduction specifically in HFpEF — a landmark development in a condition that had lacked proven disease-modifying therapy for decades.
A third category — heart failure with mildly reduced ejection fraction (HFmrEF), LVEF 40 to 49 percent — represents an intermediate group with characteristics of both phenotypes and increasing evidence supporting HFrEF-type pharmacotherapy.
Causes of Heart Failure — The Conditions That Damage the Pump
Coronary artery disease is the most common cause of HFrEF in developed countries. Myocardial infarction kills cardiomyocytes — which cannot regenerate — leaving a scar of non-contractile tissue that reduces overall systolic function. Large anterior MIs (involving the LAD territory) can produce immediate severe LV dysfunction. Multiple smaller infarctions over years produce cumulative myocardial loss. Even without overt MI, chronic coronary ischemia (hibernating myocardium) can cause diffuse contractile dysfunction that improves with revascularization.
Hypertension is the most common cause of HFpEF and a major contributor to HFrEF. Chronic pressure overload causes left ventricular hypertrophy (thickened walls), which initially compensates for the increased load but eventually leads to diastolic stiffness, reduced relaxation, and ultimately systolic dysfunction when compensatory mechanisms fail. The “hypertensive heart” progresses from LV hypertrophy to diastolic dysfunction to overt heart failure over a trajectory measured in decades — making blood pressure control the primary HFpEF prevention strategy.
Valvular heart disease — particularly aortic stenosis (pressure overload) and mitral regurgitation (volume overload) — causes heart failure through distinct hemodynamic mechanisms depending on the valve involved. Severe aortic stenosis requires the left ventricle to generate very high pressures to open the stiff aortic valve, producing concentric hypertrophy that eventually fails. Severe mitral regurgitation imposes chronic volume overload as blood regurgitates back into the left atrium with each systole, eventually leading to eccentric hypertrophy and systolic dysfunction. Timely valve intervention (surgical or transcatheter) before irreversible myocardial damage occurs is critical for preserving long-term cardiac function.
Cardiomyopathies are primary diseases of the heart muscle itself, distinct from those caused by coronary disease, hypertension, or valvular disease. Dilated cardiomyopathy (diffuse LV enlargement and systolic dysfunction) can be idiopathic, viral (post-myocarditis), genetic (familial dilated cardiomyopathy from mutations in sarcomere or cytoskeletal proteins), toxic (alcohol, anthracycline chemotherapy, cocaine, methamphetamine), or metabolic (thyroid disease, iron overload). Hypertrophic cardiomyopathy (asymmetric septal hypertrophy with diastolic dysfunction and potential LVOT obstruction) is a genetic condition that can cause heart failure, arrhythmias, and sudden cardiac death. Infiltrative cardiomyopathies (cardiac amyloidosis, cardiac sarcoidosis) deposit abnormal material in the myocardium, causing progressive restrictive physiology and heart failure.

Symptoms of Heart Failure — Recognizing the Signs of Congestion and Low Output
Heart failure symptoms arise from two primary mechanisms: congestion (fluid accumulation due to elevated cardiac filling pressures) and low cardiac output (insufficient blood delivery to organs and tissues). Most patients have a combination of both, with one often predominating.
Dyspnea (shortness of breath) is the most common and often most distressing heart failure symptom. It occurs because elevated left heart filling pressures transmit backward to the pulmonary veins, causing fluid transudation into the pulmonary interstitium and alveoli (pulmonary congestion). Even mild pulmonary congestion significantly increases the work of breathing, producing breathlessness with exertion that gradually limits activity as heart failure progresses. In advanced heart failure, dyspnea occurs at rest.
Orthopnea — dyspnea when lying flat — is highly specific for heart failure. When patients lie supine, fluid redistributes from the lower extremities into the central circulation, increasing preload and pulmonary congestion. Most heart failure patients learn to sleep with multiple pillows to elevate their upper body and reduce orthopneic symptoms; the number of pillows required (two-pillow orthopnea, three-pillow orthopnea) provides a practical index of severity.
Paroxysmal nocturnal dyspnea (PND) — sudden severe breathlessness that awakens the patient from sleep, typically 1 to 3 hours after lying down — is another highly specific heart failure symptom. PND reflects the gradual fluid redistribution and pulmonary congestion that develops after lying down for a period, eventually severe enough to produce acute dyspnea requiring the patient to sit up or go to a window for relief.
Peripheral edema — swelling of the ankles, feet, and lower legs — results from elevated systemic venous pressure that promotes fluid transudation into the interstitial space. Pitting edema (which retains an indentation when pressed) is the characteristic finding. Severe heart failure produces edema extending to the thighs, abdomen (ascites), and scrotum. Rapid weight gain (2 to 3 pounds over one to two days) reflecting fluid retention precedes visible edema by hours to days, which is why daily weight monitoring is so critical.
Fatigue and exercise intolerance reflect reduced cardiac output — the heart cannot increase output adequately with activity, limiting oxygen delivery to exercising muscles. This produces the functional limitation graded in the NYHA (New York Heart Association) classification: Class I (no symptoms with ordinary activity), Class II (mild symptoms with moderate exertion), Class III (marked limitation with minimal exertion), and Class IV (symptoms at rest).
Heart Failure Monitoring at Home — Daily Practices That Prevent Hospitalization
Heart failure is a condition of episodic decompensation — periods of clinical stability punctuated by acute worsening events (decompensated heart failure) that require hospitalization and intensive management. A significant proportion of these hospitalizations are preventable through systematic home monitoring that detects early fluid retention before it produces overt decompensation.
Daily weight measurement is the cornerstone of heart failure home monitoring. Patients should weigh themselves every morning after urinating and before eating, on the same scale, wearing similar clothing. Weight gain of 2 to 3 pounds in one to two days, or 5 pounds in one week, is a red flag requiring immediate contact with the heart failure care team for diuretic dose adjustment. Many heart failure programs use “weight-based diuretic titration” — providing patients with written instructions for adjusting furosemide dose when specific weight thresholds are crossed, without waiting for a clinical appointment.
Symptom monitoring should accompany daily weights: changes in dyspnea (needing more pillows, developing orthopnea or PND), new or worsening ankle swelling, increased fatigue at usual activity levels, or reduced urine output despite taking diuretics are all early warning signs of decompensation that warrant proactive clinical contact. Many heart failure centers provide patients with a written action plan — a “green-yellow-red” system — that specifies what self-management actions to take and when to call the care team or seek emergency evaluation based on specific symptom and weight thresholds.
Blood pressure and heart rate monitoring at home help detect hypertensive episodes (which commonly precipitate acute decompensation in HFpEF patients) and bradycardia or tachyarrhythmias (which can worsen cardiac output in HFrEF). Target blood pressure for most heart failure patients is below 130/80 mmHg; resting heart rate targets for HFrEF patients on beta-blockers are typically 60 to 70 bpm. Deviations from target ranges should be documented and reported at care team visits.
The American Heart Association’s heart failure resources provide comprehensive patient education on managing this condition. The CDC heart failure information covers prevalence, risk factors, and monitoring guidance. The NHLBI heart failure guide addresses symptoms, diagnosis, treatment, and living well with the condition.
Related reading: Coronary Artery Disease | Heart Attack Prevention | What Causes Heart Disease? | Major Risk Factors for Heart Disease | Sleep Apnea and Heart Disease
Sources
- McDonagh TA, et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur Heart J. 2021;42(36):3599-3726.
- Packer M, et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure (EMPEROR-Reduced). N Engl J Med. 2020;383(15):1413-1424.
- Solomon SD, et al. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction (DELIVER). N Engl J Med. 2022;387(12):1089-1098.
- McMurray JJ, et al. Angiotensin-Neprilysin Inhibition versus Enalapril in Heart Failure (PARADIGM-HF). N Engl J Med. 2014;371(11):993-1004.
- Ponikowski P, et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur Heart J. 2016;37(27):2129-2200.
- Gheorghiade M, et al. Rehospitalization for Heart Failure: Problems and Perspectives. J Am Coll Cardiol. 2013;61(4):391-403.
Diagnosing Heart Failure — Tests That Confirm the Diagnosis and Identify the Cause
Heart failure diagnosis requires integrating clinical presentation (symptoms and physical examination findings) with objective evidence from laboratory tests and imaging that confirm abnormal cardiac function and, where possible, identify the underlying etiology. No single test is sufficient — the diagnosis is clinical and requires the synthesis of multiple data sources.
B-type natriuretic peptide (BNP) and NT-proBNP are the most important blood biomarkers for heart failure diagnosis and monitoring. These peptides are secreted by cardiac myocytes in response to elevated wall stress — which occurs when cardiac filling pressures are elevated, as in heart failure. Elevated BNP (above 100 pg/mL in most labs) or NT-proBNP (above 300 pg/mL, with age-stratified cutoffs for acute dyspnea) strongly supports a heart failure diagnosis in a patient with dyspnea; normal values make heart failure unlikely. BNP and NT-proBNP levels also correlate with heart failure severity and are used to monitor treatment response — successful decongestion with diuresis produces falling natriuretic peptide levels, while persistently elevated or rising levels indicate inadequate treatment or disease progression. Importantly, natriuretic peptides are elevated by factors other than heart failure (renal insufficiency, pulmonary embolism, atrial fibrillation, advanced age) and are falsely low in obesity — values must always be interpreted in clinical context.
Echocardiography is the cornerstone of heart failure evaluation. A standard transthoracic echocardiogram provides direct assessment of left ventricular ejection fraction (essential for classifying HFrEF versus HFpEF), left ventricular size and wall thickness (distinguishing dilated, hypertrophic, and restrictive patterns), right ventricular function (important for prognosis and therapeutic decisions), valvular anatomy and function (identifying valvular disease as a cause or consequence), diastolic function parameters (E/A ratio, tissue Doppler velocities, E/e’ ratio) that estimate filling pressures in HFpEF, and estimated pulmonary artery pressures through tricuspid regurgitation jet velocity. In patients whose transthoracic windows are inadequate (obesity, lung disease, chest wall deformity), transesophageal echocardiography (TEE) provides superior image quality from the esophageal acoustic window.
Chest X-ray provides rapid assessment of pulmonary congestion (interstitial edema producing Kerley B lines and perihilar haziness, alveolar pulmonary edema producing the “butterfly” or “bat-wing” opacity pattern) and cardiomegaly (a cardiothoracic ratio above 0.5). Chest X-ray abnormalities in heart failure — cardiomegaly, upper lobe vascular redistribution, pulmonary edema — are classic teaching findings, but normal chest X-ray does not exclude heart failure, particularly in HFpEF where cardiac size and pulmonary vasculature may appear normal despite significantly elevated filling pressures.
Cardiac MRI (CMR) has become increasingly important in the evaluation of cardiomyopathies and heart failure of uncertain etiology. CMR provides highly accurate and reproducible measurement of biventricular volumes and ejection fraction, detailed myocardial tissue characterization through gadolinium late enhancement imaging (identifying myocardial fibrosis, infarct scar, or infiltration patterns characteristic of specific cardiomyopathies), and quantification of cardiac iron loading in hemochromatosis. The pattern of late gadolinium enhancement (subendocardial in ischemic cardiomyopathy, mid-wall in dilated cardiomyopathy, patchy in myocarditis, diffuse subendocardial in amyloidosis) provides a highly specific “fingerprint” for different heart failure etiologies.
Coronary evaluation is important in new-onset heart failure to determine whether coronary artery disease is the underlying cause, since ischemic cardiomyopathy is the most common cause of HFrEF and revascularization may improve myocardial function in patients with viable but hibernating myocardium. Coronary CT angiography is a non-invasive option for patients with low-to-intermediate pretest probability of obstructive CAD; invasive coronary angiography is indicated in patients with high probability of CAD, those presenting with ACS-like syndromes, and those with significant angina or ischemia on non-invasive testing.
Guideline-Directed Medical Therapy for HFrEF — The Four Pillars
Heart failure with reduced ejection fraction (HFrEF) is one of the most pharmacologically well-supported conditions in medicine. Four drug classes have demonstrated statistically significant reductions in all-cause mortality in landmark randomized controlled trials, and their combined use — guideline-directed medical therapy (GDMT) — produces additive survival benefit. Current guidelines recommend simultaneous initiation of all four drug classes at low doses and titration to target doses rather than the historical practice of sequential therapy.
RAAS inhibition (ACE inhibitors, ARBs, or ARNI) was the first pharmacological class to demonstrate mortality reduction in HFrEF, with the CONSENSUS and SOLVD trials in the 1980s establishing ACE inhibitors as foundational therapy. ACE inhibitors reduce afterload (by blocking angiotensin II-mediated vasoconstriction) and preload (by reducing aldosterone-driven sodium and water retention), and reverse the maladaptive neurohormonal activation that drives heart failure progression. Sacubitril-valsartan (the ARNI) combines neprilysin inhibition (which increases natriuretic peptide levels, promoting vasodilation and sodium excretion) with angiotensin receptor blockade and has become preferred over ACE inhibitors in patients who can tolerate it, based on the PARADIGM-HF trial’s demonstration of superior mortality reduction.
Beta-blockers were initially considered contraindicated in heart failure because of their negative inotropic effects — a concern that proved wrong for the long term. Three beta-blockers (carvedilol, metoprolol succinate, bisoprolol) have demonstrated mortality benefit in HFrEF through their effects on reducing heart rate (which decreases myocardial oxygen demand and prolongs diastolic filling time), blocking adverse catecholamine effects on the myocardium, and preventing sudden arrhythmic death. Beta-blockers must be started at very low doses in compensated patients (not in acutely decompensated heart failure with clinical congestion) and titrated slowly — premature high-dose initiation can precipitate acute decompensation by the acute negative inotropic effect before the beneficial remodeling effects emerge over weeks to months.
Mineralocorticoid receptor antagonists (MRAs) — spironolactone and eplerenone — reduce mortality in HFrEF by blocking aldosterone’s effects on the heart (promoting fibrosis) and kidney (driving sodium retention). They are mild diuretics that can help with congestion management but are primarily valued for their neurohormonal blockade and anti-fibrotic effects. Their primary limitation is the risk of hyperkalemia, particularly when combined with ACE inhibitors or ARBs in patients with chronic kidney disease, requiring careful monitoring of renal function and potassium levels after initiation and dose changes.
SGLT2 inhibitors (empagliflozin and dapagliflozin) are the newest class of GDMT for HFrEF, originally developed as diabetes medications and subsequently found to have powerful cardiovascular benefits independent of glycemic effects. The DAPA-HF and EMPEROR-Reduced trials demonstrated significant reductions in cardiovascular death and heart failure hospitalizations with dapagliflozin and empagliflozin respectively, in patients both with and without diabetes. Their heart failure benefits appear to derive from multiple mechanisms: osmotic diuresis that reduces preload, renal protective effects, reduced inflammation, and possible direct myocardial effects. SGLT2 inhibitors are uniquely well tolerated with minimal hemodynamic effects, making them initiatable even in patients with low blood pressure or heart rate that limits ACE inhibitor or beta-blocker dosing.
Preventing Decompensation — Strategies That Reduce Hospitalization Risk
Acute decompensated heart failure — heart failure that worsens acutely and requires hospitalization for intravenous diuresis or other intensive management — is among the most common causes of hospitalization in older adults. Each hospitalization carries substantial risks (in-hospital mortality, hospital-acquired infections, iatrogenic complications, functional decline) and high costs, and predicts worse long-term prognosis: the 60 to 90 day post-discharge period is a particularly high-risk interval during which one-quarter of hospitalized heart failure patients are rehospitalized. Many decompensation events are precipitated by identifiable and potentially preventable triggers.
The most common precipitants of acute heart failure decompensation include dietary sodium and fluid indiscretion (sodium intake above 2,000 mg/day or excessive fluid intake exceeding the heart’s ability to compensate), medication non-adherence (missing doses of diuretics or GDMT), new arrhythmias (particularly rapid atrial fibrillation, which reduces cardiac output by shortening diastolic filling time and losing atrial contribution to ventricular filling), intercurrent infections (which increase metabolic demand and provoke inflammatory responses that worsen cardiac function), hypertensive episodes (particularly in HFpEF patients), and progressive underlying disease advancement. Identifying and addressing the precipitant is as important as managing the acute decompensation itself — patients who repeatedly decompensate despite adequate medical therapy may require evaluation for advanced heart failure therapies (cardiac resynchronization therapy, implantable cardioverter-defibrillator, left ventricular assist device, or cardiac transplantation).
Structured disease management programs — combining multidisciplinary care teams, patient and caregiver education, telephone follow-up protocols, and systems for early detection and response to worsening — have demonstrated consistent reductions in heart failure hospitalization rates across multiple randomized trials. Remote monitoring technologies, including implantable hemodynamic monitors (CardioMEMS, which directly measures pulmonary artery pressures), are increasingly used in high-risk heart failure patients to detect hemodynamic deterioration before clinical symptoms emerge, allowing preemptive diuretic adjustment that prevents hospitalization.