Vascular Ultrasound for Circulation Problems
Vascular ultrasound — also called duplex ultrasonography — is the primary non-invasive imaging tool used to evaluate the circulation in arteries and veins throughout the body. Unlike cardiac ultrasound (echocardiography), which examines the heart muscle, chambers, and valves, vascular ultrasound focuses on the blood vessels themselves: the carotid arteries supplying the brain, the peripheral arteries and veins in the limbs, the renal arteries supplying the kidneys, the abdominal aorta, and the mesenteric arteries supplying the bowel.
The technique uses no radiation, requires no contrast injection, causes no discomfort beyond mild transducer pressure, and provides real-time information about both the anatomical structure of blood vessels (atherosclerotic plaque, vessel diameter, wall thickening) and the functional state of blood flow (velocity, direction, waveform pattern, resistance). For patients referred for vascular ultrasound, understanding what the test can detect, how it is performed, and what the results mean for their circulation helps them engage with their vascular specialist or cardiologist more effectively.
How Vascular Ultrasound Works — The Technology Behind the Test
Vascular duplex ultrasound combines two distinct ultrasound modalities that work simultaneously to provide a complete picture of vessel structure and function:
B-mode (brightness mode) grayscale imaging uses sound waves transmitted from the transducer head, which penetrate tissue and echo back at different intensities depending on tissue density. Fluid (including blood in vessel lumen) appears black (anechoic). Soft tissue appears gray at varying shades. Calcified structures (atherosclerotic calcium, bone) appear bright white (hyperechoic) with acoustic shadowing behind them. Atherosclerotic plaque within arterial walls appears as thickening of the intima-media layer — measured as the intima-media thickness (IMT) — with soft, hypoechoic (dark) plaque indicating lipid-rich, vulnerable composition and hyperechoic plaque indicating fibrous or calcified, more stable composition. B-mode imaging also measures vessel diameter accurately — critical for aneurysm surveillance (abdominal aortic diameter measured to determine repair timing) and for detecting thrombosis within veins or arteries.
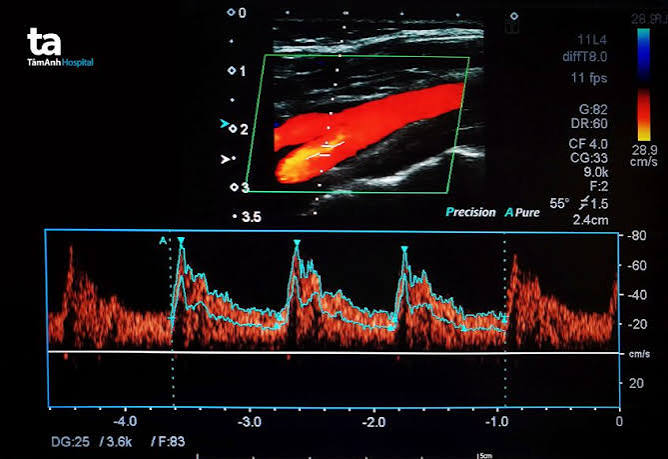
Color-flow Doppler imaging superimposes a color-coded map of blood flow direction and relative velocity onto the B-mode image. By convention, flow toward the transducer is displayed in red and flow away in blue — though the actual direction relative to the anatomy depends on transducer positioning. Turbulent, high-velocity flow in a stenotic segment appears as a mosaic of mixed colors (aliasing artifact). Areas of reversed flow (in the post-stenotic zone or the normal early-diastolic reversal in peripheral arteries) appear in the opposite color to the predominant flow direction.
Pulsed-wave (PW) spectral Doppler measures the precise velocity of blood at a specific depth within the vessel using a sample volume placed by the operator. The resulting spectral waveform — displayed with time on the x-axis and velocity on the y-axis — provides quantitative velocity measurements (peak systolic velocity, end-diastolic velocity, time-averaged mean velocity) and qualitative waveform shape analysis (triphasic/biphasic/monophasic in peripheral arteries; phasic/continuous in veins) that are the primary diagnostic criteria for arterial stenosis grading and venous occlusion detection.
Carotid Artery Ultrasound — Evaluating Stroke Risk
Carotid duplex ultrasound is among the most frequently performed vascular studies, used to evaluate patients at risk for ischemic stroke from carotid artery atherosclerosis — the second most common cause of ischemic stroke after cardioembolism:
Clinical indications for carotid duplex: Any patient who has experienced a transient ischemic attack (TIA — a brief neurological deficit lasting less than 24 hours with no infarction on imaging), minor ischemic stroke with good neurological recovery, or amaurosis fugax (transient monocular visual loss — a TIA equivalent involving the ophthalmic artery, a branch of the ICA) should have urgent carotid duplex performed within 24 to 48 hours to identify significant carotid stenosis — because the highest stroke risk period is the first 48 to 72 hours after TIA, and revascularization during this window (carotid endarterectomy or stenting) substantially reduces stroke risk. Patients with an audible carotid bruit on auscultation, those undergoing pre-operative cardiac surgery assessment, and high-risk asymptomatic patients (those with peripheral arterial disease, coronary artery disease, or multiple cardiovascular risk factors) may also undergo carotid duplex for stenosis screening.
Internal carotid artery stenosis grading: The NASCET (North American Symptomatic Carotid Endarterectomy Trial) criteria — based on the ratio of the minimum residual ICA lumen to the normal distal ICA diameter on digital subtraction angiography — have been translated into duplex velocity thresholds by the Society of Radiologists in Ultrasound consensus guidelines. Normal ICA (0% stenosis): PSV less than 125 cm/s, no plaque or intimal thickening, ICA/CCA PSV ratio less than 2.0. Mild stenosis (1–49%): PSV less than 125 cm/s with intimal thickening or plaque; ratio less than 2.0. Moderate stenosis (50–69%): PSV 125–229 cm/s, ratio 2.0–4.0. Severe stenosis (70–99%): PSV 230 cm/s or greater, ratio 4.0 or greater, EDV 100 cm/s or greater. Near-occlusion: high-grade stenosis with markedly reduced or reversed ICA flow. Total occlusion: no flow in ICA on any Doppler modality.
Lower Extremity Arterial Duplex — Peripheral Arterial Disease Evaluation
Peripheral arterial disease (PAD) affects 8 to 12 million Americans — up to 20% of adults over 65 — and is significantly underdiagnosed because many patients attribute their leg symptoms to aging or arthritis rather than circulatory insufficiency. Vascular ultrasound is the most informative imaging tool for mapping the location and severity of PAD in patients being considered for revascularization:
Arterial waveform analysis: Normal peripheral arteries at rest display a triphasic Doppler waveform: a sharp, high-amplitude forward-flow peak in systole (rapid ejection of blood by the heart); a brief period of flow reversal in early diastole (elastic recoil of the arterial wall against closed aortic valve); and a low-amplitude forward-flow component in late diastole. The loss of the diastolic reversal component — producing a biphasic waveform — indicates moderate upstream obstruction. A monophasic waveform (blunted, rounded systolic peak with continuous low-velocity forward flow throughout diastole) indicates severe proximal obstruction with high downstream resistance — the characteristic waveform distal to a significant stenosis or occlusion. Waveform qualitative analysis is the primary tool for characterizing PAD severity in segmental arterial evaluation (aortoiliac, femoral, popliteal, tibial segments), supplemented by PSV ratios at the level of stenosis (PSV ratio greater than 2.0 = greater than 50% stenosis; greater than 4.0 = greater than 75% stenosis).
Deep Vein Thrombosis — The Venous Duplex Evaluation
Deep vein thrombosis (DVT) — blood clot within the deep venous system of the legs, pelvis, or upper extremities — carries risk of pulmonary embolism (PE), post-thrombotic syndrome (chronic venous insufficiency), and recurrent thrombosis. Venous duplex ultrasonography is the first-line diagnostic test for suspected DVT, with excellent accuracy for the clinically important proximal DVT (femoral, popliteal veins) that carries the highest PE risk:
The compression test is the cornerstone of DVT diagnosis by ultrasound. The transducer is placed transversely over the vein and gentle downward pressure is applied to compress the vessel. A normal, patent vein collapses completely and its walls touch — full compressibility excludes DVT at that level with very high confidence. A thrombosed vein does not compress — the thrombus fills the lumen and prevents wall-to-wall collapse. Acute thrombus appears hypoechoic (dark, soft) and may expand the vein; chronic thrombus appears more echogenic (brighter, harder), contracts, and may calcify, with partial recanalization creating internal flow channels visible on color Doppler. The compression test is repeated at standardized levels throughout the venous system being evaluated: common femoral vein at the groin, femoral vein in the thigh, and popliteal vein at the back of the knee. If proximal DVT is confirmed at any of these levels, anticoagulant therapy is initiated.
For patients with a high clinical pre-test probability (Wells score ≥2) and negative proximal compression ultrasound, a negative D-dimer blood test (D-dimer less than 500 ng/mL) effectively excludes proximal DVT and is used to decide against repeat imaging; if D-dimer is elevated in a high-suspicion patient with negative proximal ultrasound, repeat ultrasound in 5 to 7 days (to detect propagation of isolated calf DVT into the proximal system) or CT venography is performed.
Abdominal Aortic Aneurysm Screening — Who Should Be Tested
The abdominal aorta normally measures 1.5 to 2.5 cm in diameter in adults. An abdominal aortic aneurysm (AAA) — defined as infrarenal aortic diameter of 3.0 cm or greater — develops silently in most patients until rupture (a surgical emergency with overall mortality of 70 to 90%, including those who die before reaching hospital). Vascular ultrasound provides accurate, radiation-free AAA measurement and is the recommended screening tool:
The US Preventive Services Task Force (USPSTF) recommends one-time AAA screening ultrasound for men aged 65 to 75 who have ever smoked (at least 100 cigarettes in their lifetime). This recommendation is based on evidence that screening reduces AAA-related mortality by 43% in this population by detecting aneurysms at the small, asymptomatic stage — enabling risk-stratified surveillance (small AAA: 3.0–5.4 cm, surveilled with annual ultrasound) or elective surgical repair (large AAA: 5.5 cm or greater in men, 5.0 cm or greater in women — repaired before rupture risk exceeds procedural risk). Women who have ever smoked and patients with a family history of AAA (first-degree relative) have elevated AAA risk and may benefit from individualized screening discussion with their physician, though current USPSTF evidence is insufficient to recommend routine screening in these groups.
See our related articles on ankle-brachial index test, angiogram: what patients should know, common heart tests explained, how doctors diagnose heart disease, and major risk factors for heart disease. The American Heart Association PAD guide, NHLBI peripheral arterial disease overview, and ACC/AHA PAD management guidelines provide authoritative clinical standards.
- Gerhard-Herman MD, et al. 2016 AHA/ACC Guideline on the Management of Patients with Lower Extremity Peripheral Artery Disease. J Am Coll Cardiol. 2017;69(11):e71-e126.
- Ricotta JJ, et al. Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease. J Vasc Surg. 2011;54(3):e1-e31.
- Abramowitz HB, et al. Society of Radiologists in Ultrasound (SRU) consensus guidelines for carotid ultrasound stenosis classification. Radiology. 2003;229(2):340-346.
- USPSTF. Abdominal Aortic Aneurysm: Screening. US Preventive Services Task Force Recommendation Statement. JAMA. 2019;322(22):2211-2218.
- Wells PS, et al. Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. N Engl J Med. 2003;349(13):1227-1235.
Renal Artery Ultrasound — Diagnosing Renovascular Hypertension
Renovascular hypertension — secondary hypertension caused by reduced blood flow to one or both kidneys due to renal artery stenosis — accounts for 1 to 5% of all hypertension cases but is often curable with revascularization, making accurate diagnosis important. The kidney responds to reduced perfusion pressure by activating the renin-angiotensin-aldosterone system (RAAS), releasing renin which cleaves angiotensinogen to angiotensin I, converted to angiotensin II (a potent vasoconstrictor) by ACE — producing blood pressure elevation that responds poorly to standard antihypertensive medications because the underlying renal ischemia is driving the process. Renal artery duplex ultrasound is the first-line imaging investigation for suspected renovascular hypertension, though it is technically demanding and operator-dependent:
Clinical features suggesting renovascular hypertension: Hypertension onset before age 30 (suggesting fibromuscular dysplasia — a non-atherosclerotic, non-inflammatory arterial wall disease predominantly affecting young women, causing renal artery stenosis in the mid-vessel and distal segments); abrupt onset or acceleration of previously controlled hypertension in an older patient with known atherosclerosis (suggesting atherosclerotic renal artery stenosis — the most common form, typically involving the renal artery ostium and proximal segment); refractory hypertension requiring three or more antihypertensive medications at optimal doses; deterioration of renal function after initiation of ACE inhibitor or ARB (bilateral renal artery stenosis or unilateral stenosis to a solitary kidney causes a dramatic drop in GFR when efferent arteriolar dilation from ACE inhibition is blocked); unexplained asymmetric kidney size greater than 1.5 cm difference on imaging; flash pulmonary edema episodes in a patient with bilateral renal artery stenosis.
Duplex criteria and limitations: The primary diagnostic criterion for hemodynamically significant renal artery stenosis is renal artery PSV greater than 180 cm/s combined with a renal-to-aortic ratio (renal artery PSV divided by aortic PSV) greater than 3.5 — achieving approximately 85% sensitivity and 92% specificity for stenosis of 60% or greater. An elevated renal resistance index (RI = 1 minus end-diastolic velocity divided by PSV of the intrarenal interlobar arteries, with normal less than 0.70) greater than 0.80 suggests intrinsic parenchymal disease and predicts a poor response to renal revascularization — an important finding that guides the decision between angioplasty and medical therapy. Technical limitations are significant: visualization of the renal arteries requires the patient to fast for 4 to 6 hours before the examination (to minimize bowel gas that causes signal degradation); obesity significantly impairs image quality; multiple renal arteries (present in 20 to 30% of individuals) may be missed; and the examination requires 45 to 60 minutes of skilled operator time. CT angiography and MR angiography provide superior visualization of the renal arteries and are typically used to confirm positive or equivocal duplex findings before revascularization planning.
Mesenteric Artery Duplex — Evaluating Chronic Mesenteric Ischemia
Chronic mesenteric ischemia (CMI) — inadequate blood flow to the intestines due to atherosclerotic stenosis of the mesenteric arteries — causes a characteristic clinical syndrome of postprandial abdominal pain and significant weight loss. Patients fear eating because pain follows meals (the increased intestinal oxygen demand during digestion cannot be met by the stenotic mesenteric arteries), leading to food avoidance and progressive malnutrition. CMI is rare but serious, often misdiagnosed as peptic ulcer disease, irritable bowel syndrome, or malignancy before the vascular etiology is identified — typically requiring significant weight loss and multiple negative gastrointestinal investigations before the diagnosis is considered.
Mesenteric duplex evaluates the celiac artery (CA) and superior mesenteric artery (SMA) — the two major vessels supplying the small intestine and most of the large intestine. The inferior mesenteric artery (IMA) is more difficult to visualize and less frequently the isolated cause of CMI. Duplex velocity criteria for significant mesenteric stenosis: fasting SMA PSV greater than 275 cm/s or fasting CA PSV greater than 200 cm/s indicates hemodynamically significant stenosis (greater than 70% diameter narrowing). Postprandial augmentation testing — measuring SMA velocity 30 minutes after a standardized liquid meal — shows marked velocity increase in normal vessels (increased intestinal demand drives increased flow) and blunted augmentation in stenotic vessels (the artery cannot increase flow to meet demand). CMI generally requires stenosis of both the celiac artery and SMA (or their collateral network is impaired) because the rich collateral connections between the celiac and SMA territories allow one artery to compensate for the other — isolated single-vessel stenosis rarely causes symptoms. Revascularization (mesenteric angioplasty and stenting or surgical bypass) relieves symptoms in more than 90% of appropriately selected patients, often producing dramatic weight recovery.
How to Prepare for Your Vascular Ultrasound Appointment
Preparation requirements for vascular ultrasound vary depending on which vessels are being evaluated:
Carotid duplex: No specific preparation required. Wear a loose, low-cut neckline or a garment that can be easily pulled aside to allow transducer access to the neck. Remove necklaces and earrings. The examination takes 30 to 45 minutes. You will lie on your back with a small pillow under your head and neck; the sonographer applies water-based gel to the skin and moves the transducer along both sides of the neck systematically. The examination is completely painless.
Abdominal vascular duplex (aorta, renal arteries, mesenteric arteries, iliac arteries): Fast for 4 to 6 hours before the examination — water and necessary medications with small sips are permitted. Fasting minimizes bowel gas, which severely degrades image quality for deep abdominal vessels. Avoid carbonated beverages on the day of the examination. The examination takes 45 to 90 minutes depending on the complexity and the number of vessels being evaluated.
Lower extremity arterial duplex (PAD evaluation): No specific preparation. Wear or bring loose-fitting shorts or trousers that can be rolled up to mid-thigh. The examination evaluates from the aortoiliac segment down through the tibial vessels to the ankle — a complete bilateral lower extremity arterial study takes 60 to 90 minutes.
Lower extremity venous duplex (DVT evaluation): No specific preparation. Compression stockings (if worn) should be removed before the examination. The sonographer will need access to the groin and the full length of the thigh and calf.
Vascular Ultrasound Versus Other Vascular Imaging Tests
Vascular duplex ultrasound is the first-line imaging tool for most vascular conditions, but its limitations mean that CT angiography, MR angiography, and invasive angiography are often required for definitive diagnosis or pre-operative planning:
CT angiography (CTA): Uses intravenous iodinated contrast and thin-slice CT imaging to reconstruct three-dimensional images of the arterial anatomy. CTA provides superior visualization of deep vessels (renal arteries, mesenteric arteries, iliac arteries), calcified plaque (which causes significant imaging artifacts on MRA but is directly visualized on CTA), and vessel relationships with surrounding structures. Limitations: radiation exposure (significant for surveillance of young patients or repeated examinations), iodinated contrast risk (nephropathy in patients with CKD, allergy in those with prior contrast reactions), and inability to provide real-time or functional information.
MR angiography (MRA): Uses gadolinium contrast (or non-contrast time-of-flight techniques) and MR imaging to visualize blood vessels. MRA avoids radiation and iodinated contrast — preferable for young patients, those with contrast allergy, and those requiring repeated surveillance imaging. Limitations: contraindicated in patients with certain metallic implants (pacemakers, cochlear implants — though MR-conditional devices are increasingly available), claustrophobia, and calcified plaque is not directly visualized (though this eliminates the overestimation artifact seen on CTA near calcified plaque).
Catheter-based invasive angiography: The gold standard for vascular imaging — direct contrast injection into the vessel under fluoroscopy provides the highest-resolution real-time images and enables simultaneous intervention (balloon angioplasty, stenting). Reserved for patients in whom non-invasive imaging is indeterminate, when intervention is planned, or when pressure measurements (fractional flow reserve across a renal or mesenteric stenosis) are needed to confirm hemodynamic significance before committing to revascularization.
Vascular ultrasound’s unique strengths — no radiation, no contrast, real-time capability, portability, low cost, and the ability to repeat examinations for surveillance — make it the indispensable foundation of non-invasive vascular diagnosis, complemented by CTA, MRA, or invasive angiography when its limitations are reached.