Angiogram: What Patients Should Know
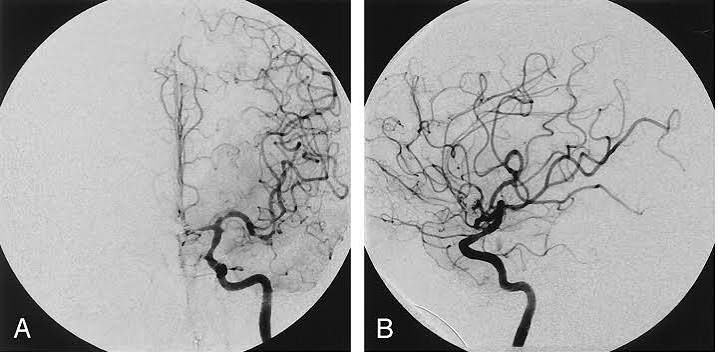
An angiogram — specifically a coronary angiogram — is the most precise available test for visualizing the coronary arteries and identifying blockages that cause heart disease. Where non-invasive tests like stress testing, coronary calcium scoring, and CT coronary angiography provide indirect or lower-resolution images of coronary anatomy, the invasive coronary angiogram delivers high-resolution, real-time X-ray images of the arterial lumen from inside — the gold standard against which all other coronary imaging modalities are measured.
For patients who have been referred for a coronary angiogram, understanding what the procedure involves, what information it provides, what risks are involved, and what comes next based on the results transforms a potentially anxiety-provoking procedure into a manageable clinical event with clear purpose and known outcomes. This guide provides the essential patient education that every person scheduled for a coronary angiogram should have before walking into the catheterization laboratory.
Why a Coronary Angiogram Is Ordered — The Clinical Indications
Coronary angiography is not ordered as a routine screening test — it is a targeted diagnostic procedure ordered when there is a specific clinical question about coronary artery anatomy that non-invasive testing cannot adequately answer, or when revascularization (treatment of a blockage by stenting or surgery) is being planned:
Acute coronary syndromes (ACS): In patients with ST-elevation myocardial infarction (STEMI — the most urgent form of heart attack, with complete coronary artery occlusion), emergency coronary angiography followed immediately by primary percutaneous coronary intervention (PCI — balloon angioplasty and stent) is performed within 90 minutes of first medical contact at PCI-capable centers, restoring blood flow before permanent muscle damage. For non-ST elevation ACS (NSTEMI and unstable angina), coronary angiography is performed within 2 to 72 hours depending on risk stratification — patients with high-risk features (dynamic ECG changes, elevated troponin, hemodynamic instability) undergo early invasive angiography within 2 to 24 hours.
Stable coronary artery disease with positive non-invasive testing: Patients with significant ischemia on stress testing (large territory of stress-induced perfusion defect on nuclear imaging, significant wall motion abnormality on stress echo, or high-risk ECG findings on exercise stress test) are referred for coronary angiography to define the anatomy and determine whether revascularization is appropriate. Similarly, patients with high-risk findings on coronary CT angiography (severe stenosis, left main or proximal LAD disease) are referred for invasive angiography for functional assessment and potential PCI planning.
Valvular heart disease pre-surgical assessment: Patients over 40 years of age undergoing open heart surgery for valve replacement or repair, congenital heart defect repair, or other cardiac surgical procedures typically undergo pre-operative coronary angiography to identify concurrent coronary artery disease that would require bypass grafting at the time of surgery — preventing a second open-heart operation later.
Heart failure of unclear etiology: Patients presenting with new-onset heart failure of unclear cause — where distinguishing ischemic cardiomyopathy (heart failure from coronary artery disease and prior infarction) from non-ischemic cardiomyopathy (dilated, viral, or toxic) changes management — may undergo coronary angiography to identify or exclude significant coronary disease as the cause of LV dysfunction.
The Difference Between Angiogram and Angioplasty
A common source of patient confusion is the distinction between the diagnostic angiogram and the therapeutic procedure (angioplasty or stenting) that may follow it. Understanding this distinction helps patients prepare appropriately:
The coronary angiogram is the diagnostic phase — it reveals what is in the arteries but does not treat anything. The cardiologist looks at the images and determines whether there is a blockage, how severe it is, and where it is located. If the angiogram reveals a blockage that warrants treatment, the cardiologist may immediately proceed to percutaneous coronary intervention (PCI) — inflating a small balloon to open the blocked artery and placing a drug-eluting stent (a small metal mesh tube coated with medication that prevents re-narrowing) to keep it open. This combined procedure — diagnostic angiogram followed immediately by PCI — is called “ad hoc PCI.” Alternatively, the cardiologist may determine that surgery (coronary artery bypass grafting — CABG) is a better option for complex multi-vessel disease and refer the patient to a cardiac surgeon.
Preparing for Your Angiogram — What to Do Before the Procedure
Adequate preparation for a coronary angiogram ensures the procedure is as safe and informative as possible. Here is what patients typically need to do in the days and hours before their procedure:
Medications to discuss with your cardiologist: Most regular medications are continued before an angiogram, but several require specific attention. Metformin should be held on the day of the procedure and for 48 hours after (if contrast is administered) in patients with CKD — contrast exposure in the setting of ongoing metformin use rarely causes lactic acidosis if renal function deteriorates post-contrast. Warfarin may need to be held for 3 to 5 days before the procedure (depending on the access site planned — transradial access can be performed with therapeutic INR; transfemoral access typically requires INR below 1.8). Direct oral anticoagulants (apixaban, rivaroxaban, dabigatran, edoxaban) are typically held for 24 to 48 hours before elective procedures. Aspirin and P2Y12 inhibitors (clopidogrel, ticagrelor, prasugrel) are generally continued — they are essential pre-treatment if PCI is anticipated. Discuss all your medications with your cardiologist or the catheterization laboratory nurse during your pre-procedure call.
The day before: Eat and drink normally until midnight (or as directed by your specific hospital protocol). Shower normally. Remove nail polish from the access-side wrist (for pulse oximetry monitoring) if transradial access is planned. Arrange transportation home — you will not be able to drive on the day of the procedure due to sedation and the need for post-procedure rest. If staying overnight, pack a small bag with essential items.
Day of the procedure: Do not eat or drink anything for 4 to 6 hours before your scheduled procedure time (clear liquids are often permitted up to 2 hours before, but follow your hospital’s specific instructions). Take your prescribed morning medications with a small sip of water unless specifically told to hold them. Arrive at the designated time — you will be checked in, asked to change into a hospital gown, have blood pressure and ECG monitored, and be connected to intravenous fluids before being brought to the catheterization laboratory.
After the Angiogram — Recovery and Next Steps
Understanding what recovery looks like — and what to watch for — helps patients manage the post-procedure period confidently at home:
Transradial recovery (same-day discharge): After the procedure, a compression wristband is applied to the access site and gradually deflated over 2 to 4 hours to achieve hemostasis (blood clotting at the puncture site). You will be observed for 1 to 2 hours in the recovery area — monitoring for access site bleeding, chest pain, or contrast reactions. Once the wristband is removed and the access site is sealed, you are discharged home with written instructions. Drive restrictions: you should not drive for at least 24 hours due to sedation effects, even if you feel completely normal. Physical activity: avoid heavy lifting or strenuous activity with the access-side arm for 5 to 7 days. Showering: permitted from the day after the procedure.
What to watch for at home: Contact the catheterization laboratory or emergency services immediately if you experience: re-bleeding at the access site (sustained pressure for 10 minutes with a clean cloth while lying the arm flat; if bleeding continues, go to the emergency department); sudden severe chest pain (may indicate coronary artery complication); rapidly expanding bruise or pulsating swelling at the wrist (possible pseudoaneurysm); coldness, numbness, or color change in the access-side hand (possible radial artery occlusion — most resolve spontaneously, but evaluation is needed); dark urine (rare sign of contrast-induced nephropathy or, very rarely, contrast reaction affecting kidneys).
Getting your results: If the angiogram was diagnostic only (no intervention performed), your cardiologist will review the images and discuss findings with you — either before discharge or at a follow-up appointment within 1 to 2 weeks. Results will describe which coronary arteries are affected, the severity of any stenoses, the overall coronary anatomy, and the recommended management (medical therapy, PCI, or surgical referral). If PCI was performed during the same procedure, you will receive results immediately and be counseled on post-stent antiplatelet therapy (dual antiplatelet therapy with aspirin plus a P2Y12 inhibitor — typically for 6 to 12 months after drug-eluting stent).
See our related articles on common heart tests explained, cardiac CT scan: what it shows, stress test for heart health, coronary calcium score, and major risk factors for heart disease. The American Heart Association cardiac procedures guide, NHLBI coronary angiography overview, and ACC/AHA coronary revascularization guidelines provide authoritative clinical standards.
- Lawton JS, et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization. J Am Coll Cardiol. 2022;79(2):e21-e129.
- Collet JP, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289-1367.
- Neumann FJ, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87-165.
- Roffi M, et al. Radial versus femoral access in patients with acute coronary syndromes. Lancet. 2015;385(9986):2465-2476.
- Mehran R, et al. Standardized Bleeding Definitions for Cardiovascular Clinical Trials (BARC). Circulation. 2011;123(23):2736-2747.
Understanding Your Angiogram Results — What the Report Means
After your angiogram, your cardiologist will discuss the findings with you in detail. Understanding the terminology used in the angiogram report helps you participate meaningfully in those conversations and make informed decisions about your care:
Coronary anatomy terminology: The left coronary artery system originates from a short common trunk called the left main coronary artery (LM), which divides into the left anterior descending artery (LAD — supplies the front wall and the septum between the ventricles, the largest territory) and the left circumflex artery (LCX — supplies the lateral and posterior walls). The right coronary artery (RCA) originates separately and supplies the right ventricle, inferior wall of the left ventricle, and the conduction system (SA node, AV node) in most patients. “Dominant” coronary anatomy refers to which artery supplies the posterior descending artery (PDA) branch — right dominant (70% of patients), left dominant (10%), or co-dominant (20%). Dominance matters because occlusion of a dominant artery affects a larger territory and carries higher risk.
Stenosis severity classification: Your report will describe blockages as a percentage diameter narrowing of the most affected segment compared to the adjacent reference vessel. The clinical decision thresholds are: less than 50% — non-obstructive atherosclerosis, medical therapy only; 50–70% (intermediate) — functional assessment with FFR or iFR pressure wire required before revascularization decision; 70% or greater — hemodynamically significant, revascularization recommended in symptomatic patients; 90% or greater — severe, high-priority lesion; 100% — total occlusion, either acute (STEMI requiring emergency PCI) or chronic (CTO, requiring specialized techniques if revascularization is pursued). Left main stenosis of 50% or greater is treated as a severe, high-priority finding because the left main supplies the majority of the left ventricle.
TIMI flow grading: The angiogram report may reference TIMI (Thrombolysis in Myocardial Infarction) flow grades — a standardized scale for describing contrast flow through the coronary artery: TIMI 0 = no flow (complete occlusion); TIMI 1 = penetration without perfusion (contrast enters but does not fill the distal vessel); TIMI 2 = partial reperfusion (contrast fills and clears the artery, but more slowly than normal); TIMI 3 = complete, brisk flow equivalent to a normal artery. The goal of PCI in STEMI is restoration of TIMI 3 flow — TIMI 3 at the end of the procedure correlates strongly with preserved myocardial function and improved survival.
Coronary Angiogram Versus Other Heart Tests — Where It Fits in the Diagnostic Pathway
Understanding how the coronary angiogram relates to the other cardiac tests you may have undergone before being referred for catheterization helps you see the complete diagnostic picture:
Exercise stress test (EST): The exercise ECG stress test detects ischemia indirectly through ST-segment changes and symptoms during exercise. Sensitivity for significant coronary artery disease is approximately 68% (missing about 1 in 3 patients with significant blockage) and specificity approximately 77% (producing false positives in about 1 in 4 patients without significant blockage). High-risk EST findings — horizontal or downsloping ST depression greater than 2 mm, early onset ST changes at low workload, hypotensive response to exercise, ventricular tachycardia during exercise — warrant coronary angiography for definitive anatomical evaluation.
Nuclear stress test (myocardial perfusion imaging): Radiotracer (technetium or thallium) distribution imaging during stress and rest identifies areas of reduced blood flow (ischemia) or absence of viable tissue (prior infarction) with higher sensitivity (85–90%) than the exercise ECG. Large territories of stress-induced ischemia — greater than 10% of the left ventricular area — are an independent indication for coronary angiography regardless of symptoms, because large ischemic burden predicts cardiac events that revascularization can prevent.
Coronary CT angiography (CTCA): The non-invasive coronary CTA uses intravenous contrast and CT imaging to reconstruct three-dimensional images of the coronary arteries without arterial catheterization. CTCA has very high negative predictive value (greater than 99%) — a normal CTCA essentially excludes significant coronary artery disease. However, calcified plaques create imaging artifacts that can overestimate stenosis severity on CT, and CTCA cannot perform functional assessment (FFR/iFR) or proceed directly to treatment. CTCA is therefore ideal for ruling out CAD in low-to-intermediate probability patients; patients with high CTCA burden or suspected significant stenosis are referred to invasive angiography for functional assessment and potential PCI.
Echocardiography: Transthoracic echocardiography evaluates left ventricular function (ejection fraction), wall motion abnormalities (suggesting prior infarction in the territory of a specific coronary artery), valve anatomy, and pericardial effusion. Regional wall motion abnormalities — hypokinesia (reduced motion), akinesia (absent motion), or dyskinesia (paradoxical outward motion) — in a coronary territory pattern indicate ischemic cardiomyopathy and guide the angiography interpretation (correlating the angiographic stenosis location with the echo wall motion territory).
Fractional Flow Reserve (FFR) and Instantaneous Wave-Free Ratio (iFR) — Making the Most of Your Angiogram
One of the most important advances in invasive cardiology over the past two decades is the ability to measure the functional significance of a coronary stenosis during the same catheterization procedure using pressure wire technology — eliminating the need for repeat testing and enabling more precise revascularization decisions:
What FFR measures: FFR (fractional flow reserve) is the ratio of the maximum blood flow achievable distal to a stenosis compared to the theoretical maximum flow if that stenosis were not present. It is measured by advancing a pressure-tipped guidewire across the stenosis and measuring the ratio of distal-to-proximal coronary pressure during pharmacological hyperemia (maximal vasodilation induced by adenosine — administered intravenously or intracoronary). An FFR value of 1.0 means there is no pressure gradient across the stenosis — the stenosis does not impede flow. The validated ischemia threshold is 0.80: an FFR of 0.80 or less indicates hemodynamically significant ischemia and PCI is beneficial; an FFR above 0.80 indicates the stenosis is not causing ischemia and medical therapy alone is as safe as PCI.
DEFER and FAME trial evidence: The landmark DEFER trial showed that patients with intermediate stenoses (40–70% diameter narrowing) and FFR greater than 0.75 who were treated medically had the same 5-year cardiac event rate as those who had PCI — demonstrating that angiographic appearance alone overestimates the functional significance of many intermediate stenoses. The FAME trial extended this evidence: FFR-guided PCI (treating only stenoses with FFR ≤0.80) compared to angiography-guided PCI (treating all stenoses ≥50%) reduced unnecessary stenting by 37%, reduced major adverse cardiac events at 1 year, and reduced costs — all without compromising safety. FFR guidance is now a Class I recommendation in international revascularization guidelines for intermediate coronary stenoses.
iFR (instantaneous wave-free ratio): iFR is an adenosine-free alternative to FFR that measures the pressure ratio across a stenosis during a specific resting period of the cardiac cycle (the “wave-free period” in diastole when microvascular resistance is naturally lowest and stable). The DEFINE-FLAIR and iFR-SWEDEHEART trials demonstrated that iFR-guided revascularization (threshold ≤0.89) was non-inferior to FFR-guided revascularization for major adverse cardiac events at 12 months, with the advantage of not requiring adenosine administration — eliminating adenosine-related side effects (chest discomfort, flushing, transient dyspnea) and reducing procedure time and cost. Most catheterization laboratories now offer both FFR and iFR, with the choice based on local expertise, patient factors, and specific stenosis characteristics.
Angiogram-Guided Treatment Decisions — What Comes After the Angiogram
The management pathway following coronary angiography depends on the anatomical and functional findings — a multidisciplinary approach that has been increasingly formalized through the concept of the “Heart Team” (interventional cardiologist plus cardiac surgeon) for complex cases:
Medical therapy alone: Patients with non-obstructive coronary artery disease (less than 50% stenosis), intermediate stenoses with FFR greater than 0.80, or mild single-vessel disease without ischemia are managed with optimized medical therapy — high-intensity statin (rosuvastatin 20–40 mg or atorvastatin 40–80 mg), aspirin 75–100 mg daily, blood pressure control (target less than 130/80 mmHg), diabetes management (HbA1c less than 7.0%), smoking cessation, and lifestyle modification. Several trials (COURAGE, ISCHEMIA) demonstrated that optimal medical therapy alone achieves equivalent long-term outcomes compared to PCI in many stable CAD patients — PCI provides superior symptom relief but does not reduce MI or death in stable patients with preserved LV function when added to optimal medical therapy.
Percutaneous coronary intervention (PCI): PCI is the preferred revascularization strategy for single-vessel or two-vessel disease (except proximal LAD disease in the setting of reduced LV function), acute coronary syndromes (STEMI and high-risk NSTEMI), and stable CAD patients with significant ischemia who remain symptomatic despite optimal medical therapy. Drug-eluting stents (DES) — thin metallic mesh platforms coated with antiproliferative drugs (everolimus, zotarolimus, biolimus) on a polymer — are used in virtually all contemporary PCI; DES reduces restenosis rates from approximately 20–30% with bare-metal stents to less than 5% at 1 year. After DES implantation, dual antiplatelet therapy (DAPT) with aspirin plus a P2Y12 inhibitor — clopidogrel, ticagrelor, or prasugrel — is prescribed for 6 to 12 months to prevent stent thrombosis (acute stent occlusion, which carries high mortality risk).
Coronary artery bypass grafting (CABG): CABG is preferred over PCI for left main coronary artery disease, three-vessel disease with reduced LV function, complex multi-vessel disease with high SYNTAX score (≥23), two-vessel disease involving the proximal LAD with diabetes, and anatomically complex lesions not suitable for PCI (severely calcified, long diffuse disease, chronic total occlusions in multiple vessels). CABG uses conduits — typically the internal mammary arteries (IMA — left IMA is the graft of choice for LAD, providing 90–95% 10-year patency) and saphenous vein grafts — to bypass blocked coronary arteries and supply blood downstream from the obstruction. The SYNTAX trial established that for complex three-vessel and left main CAD, CABG provides superior long-term freedom from repeat revascularization and improved survival compared to PCI, particularly in patients with diabetes and high SYNTAX scores.