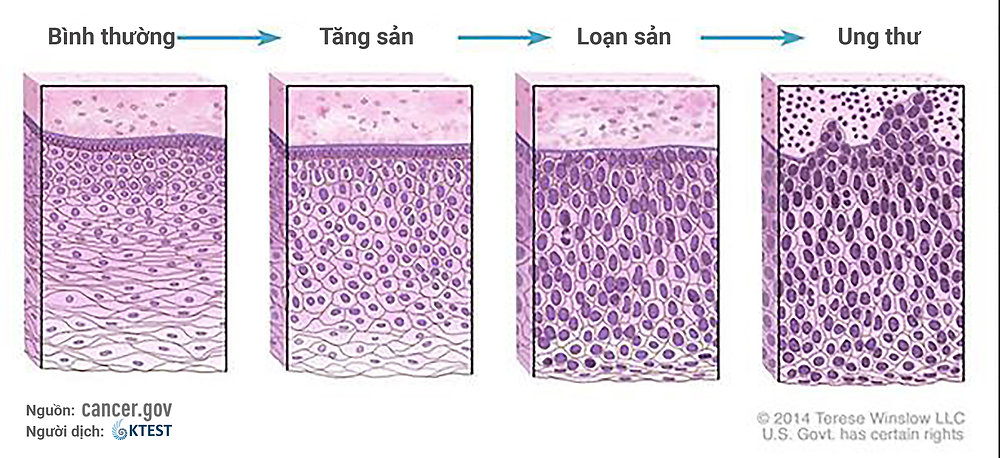
Cancer grade describes how abnormal cancer cells look under a microscope compared to normal cells of the same tissue. It is one of the most important factors reported on a pathology report — not because it tells you where the cancer has spread (that is cancer staging), but because it reveals how aggressive the cancer is likely to be and how fast it is likely to grow. Cancer grade and stage are both needed for a complete picture. Two patients with the exact same stage can have very different prognosis and treatment plans based on their cancer grade.
A small Stage I breast cancer that is Grade 3 may receive chemotherapy while an identically staged Grade 1 tumor may not — because grade predicts biological aggressiveness that imaging cannot show. Understanding cancer grade helps you ask better questions at your next oncology appointment.
Cancer Grade vs. Cancer Stage — Two Different Things
Patients often confuse grade and stage because both are numerical scales reported at diagnosis. The distinction is fundamental:
| Cancer Grade | Cancer Stage | |
|---|---|---|
| What it measures | How abnormal cancer cells look under the microscope | Where cancer is and how far it has spread |
| How determined | Pathologist examines biopsy or surgical specimen | Imaging (CT, PET, MRI) + biopsy + surgery |
| Scale | Grade 1–3 (or 1–4) in most systems | Stage I–IV |
| What it predicts | Tumor aggressiveness, growth rate, chemo response | Surgical options, systemic treatment approach, prognosis |
Grade is determined from tissue — you need a biopsy or surgical specimen to grade a cancer. No imaging test can determine grade. This is why biopsy is mandatory — not just to confirm malignancy, but to characterize the tumor’s biological behavior. A Stage IA breast cancer that is Grade 3 may be treated more aggressively than a larger Stage IIA Grade 1 breast cancer, because grade predicts a fundamentally different relapse risk.
The General Grade 1–3 System
Most solid tumors use a 3-grade scale. The pathologist evaluates two microscopic features: differentiation (how much do cancer cells resemble the normal tissue they came from?) and mitotic rate (how frequently are cells dividing?).
| Grade | Also Called | Cell Appearance | Growth Rate |
|---|---|---|---|
| Grade 1 | Low grade / Well differentiated | Cells look similar to normal tissue; organized architecture; low mitotic rate | Slow |
| Grade 2 | Intermediate grade / Moderately differentiated | Some abnormality; partial loss of normal tissue organization | Moderate |
| Grade 3 | High grade / Poorly differentiated | Cells look very abnormal; high mitotic rate; no resemblance to normal tissue | Fast |
| Grade 4 | Undifferentiated / Anaplastic | No identifiable tissue type; complete loss of normal organization | Fastest |
Nottingham Grade — Breast Cancer
The Nottingham Grading System (also called Elston-Ellis or modified Bloom-Richardson grade) is the standard grading system for invasive breast cancer. The pathologist assigns a score of 1–3 to each of three microscopic features, then totals them:
| Feature | Score 1 | Score 2 | Score 3 |
|---|---|---|---|
| Tubule formation | ≥75% of tumor forms tubular structures | 10–75% tubule formation | <10% tubule formation |
| Nuclear pleomorphism | Small, uniform nuclei similar to normal cells | Moderate nuclear size variation | Marked variation in nuclear size and shape |
| Mitotic count | Few mitoses (varies by field area) | Intermediate number of mitoses | Many mitoses visible |
Total score → Nottingham grade:
- Score 3–5 = Grade 1 (low grade, well differentiated)
- Score 6–7 = Grade 2 (intermediate grade)
- Score 8–9 = Grade 3 (high grade, poorly differentiated)
Grade is one of the three most important prognostic factors in breast cancer — alongside tumor size (T) and lymph node status (N). For ER-positive, HER2-negative breast cancer, Grade 3 signals higher recurrence risk even in node-negative patients — and often triggers Oncotype DX testing to determine whether chemotherapy is needed beyond hormonal therapy. A Recurrence Score ≥26 on Oncotype DX indicates significant chemotherapy benefit, particularly in premenopausal women (TAILORx trial, NEJM 2018–2019).
Ki-67 proliferation index measured on the biopsy correlates closely with Nottingham grade:
- Ki-67 <14%: Low proliferation → typically Grade 1; Luminal A biology
- Ki-67 14–20%: Intermediate; Luminal A or early Luminal B
- Ki-67 ≥20%: High proliferation → typically Grade 3; Luminal B or triple-negative biology
Gleason Score and Grade Groups — Prostate Cancer
The Gleason grading system is the most widely known cancer grading tool. The pathologist identifies the two most prevalent architectural patterns in the tumor and grades each on a 1–5 scale based on gland formation:
- Pattern 3: Still discrete, well-formed glands — most like normal prostate
- Pattern 4: Fused, cribriform, or poorly formed glands — significantly abnormal
- Pattern 5: No glandular formation — sheets, cords, or single cells; most abnormal
The Gleason score equals primary pattern + secondary pattern. A Gleason 3+4=7 differs importantly from 4+3=7 despite the same sum — 4+3 has predominantly higher-grade pattern and carries higher risk.
The 2014 ISUP Consensus Conference reformulated Gleason scores into five Grade Groups for clearer clinical communication:
| Grade Group | Gleason Score | Risk Level | Typical Management |
|---|---|---|---|
| Grade Group 1 | 3+3=6 | Very low risk | Active surveillance preferred for most patients |
| Grade Group 2 | 3+4=7 | Intermediate favorable | Active surveillance or treatment discussion |
| Grade Group 3 | 4+3=7 | Intermediate unfavorable | Treatment typically recommended |
| Grade Group 4 | 4+4=8 | High risk | Prompt definitive treatment required |
| Grade Group 5 | 9–10 | Very high risk | Immediate aggressive treatment |
Approximately 60% of prostate cancers diagnosed at biopsy are Grade Group 1 — so indolent in most men that active surveillance (regular PSA + repeat biopsy/mpMRI without treatment) is the standard approach. This avoids treatment side effects — incontinence, erectile dysfunction — in men whose cancer may never cause harm. Grade Group 4–5 (Gleason 8–10) requires prompt definitive treatment: surgery, radiation, or both combined with androgen deprivation therapy. Learn how PSA and other blood tests are used alongside Grade Group in the cancer blood test guide.
Cancer Grade for Other Tumor Types
Neuroendocrine Tumors (NETs) — Ki-67 as Primary Grade Marker
Neuroendocrine tumors are graded primarily by Ki-67 proliferation index, not by traditional differentiation criteria. WHO 2019 classification:
| WHO Grade | Ki-67 Index | Mitotic Rate | Clinical Management |
|---|---|---|---|
| G1 (Low grade) | <3% | <2/10 HPF | Somatostatin analogues ± observation |
| G2 (Intermediate) | 3–20% | 2–20/10 HPF | Systemic treatment may be required |
| G3 (High grade) | >20% | >20/10 HPF | Often chemotherapy required |
| NEC (Carcinoma) | >20% | >20/10 HPF | Platinum-based chemotherapy; poorest prognosis |
G1 NETs (including carcinoid tumors) may be present for years before causing symptoms and often progress slowly. NEC (neuroendocrine carcinoma) — distinct from G3 NET by its poorly differentiated morphology — is treated with platinum-based chemotherapy similar to small cell lung cancer.
Brain Tumors — WHO 2021 Molecular-Integrated Grade
The WHO 2021 classification of CNS tumors was a landmark change — it integrated molecular markers into grade for the first time. For gliomas, histological appearance alone is no longer sufficient:
- Grade 1: Pilocytic astrocytoma — often curable with surgery alone
- Grade 2: IDH-mutant diffuse glioma — slow-growing; molecular markers drive prognosis
- Grade 3: IDH-mutant anaplastic glioma — requires treatment beyond surgery
- Grade 4: Glioblastoma (IDH-wildtype GBM) — median OS 14–16 months with optimal treatment (surgery + temozolomide + radiation)
Key molecular markers now built into brain tumor grade: IDH mutation (better prognosis regardless of histologic grade), 1p/19q codeletion (defines oligodendroglioma — best-prognosis diffuse glioma), MGMT promoter methylation (predicts benefit from temozolomide in GBM).
Bladder Cancer — Low Grade vs. High Grade
The WHO 2004/2022 classification simplified bladder cancer grading to two categories, replacing the older Grade 1/2/3 system:
- Low-grade urothelial carcinoma: Regular growth pattern; low risk of progression to invasive disease
- High-grade urothelial carcinoma: Disordered growth; significant risk of progression to muscle-invasive disease; managed with intravesical BCG after resection
Lymphoma — The Grade Paradox
Lymphoma “grade” refers to clinical aggressiveness rather than cellular differentiation. The most clinically important fact in lymphoma grading is the paradox:
DLBCL (high-grade): R-CHOP achieves 60–70% long-term cure rate.
Burkitt lymphoma: >90% cure in children with intensive chemotherapy protocols.
Follicular lymphoma (low-grade): Long clinical course of 10–20+ years — but rarely cured with standard chemotherapy.
Molecular Grade — Beyond the Microscope
Traditional histological grade (what cells look like) is increasingly complemented — and in some cases replaced — by molecular characterization:
- Oncotype DX Recurrence Score (breast cancer): A 21-gene RT-PCR panel generating a Recurrence Score (RS) from 0–100. RS ≥26 = significant chemotherapy benefit, particularly in premenopausal women (TAILORx, NEJM 2019). Effectively extends grade into a numerical, actionable chemotherapy decision tool for ER+/HER2-/node-negative breast cancer.
- Ki-67 as pharmacodynamic marker: Ki-67 measured on post-neoadjuvant therapy specimens (residual disease) is an independent prognostic marker — a falling Ki-67 indicates treatment response.
- PAM50 intrinsic subtypes: Gene expression profiling identifies four subtypes regardless of histological grade — Luminal A, Luminal B, HER2-enriched, and Basal-like/Triple-negative — each with distinct prognosis and treatment implications.
- MSI/MMR status (colorectal cancer): MSI-H tumors often have Grade 2–3 histology but behave better at Stage II than microsatellite-stable (MSS) tumors — and respond dramatically to pembrolizumab immunotherapy (FDA-approved 2017 in the first tumor-agnostic approval).
Tumor markers such as CA-125, CEA, and AFP track cancer activity over time but are separate from grade, which is a fixed pathological assessment at the time of biopsy or surgery.
What Cancer Grade Means for Your Treatment
- Grade 1 in your report: Cancer cells look relatively normal. Slower growth, often less intensive treatment — potentially active surveillance (prostate), hormonal therapy alone (breast), or surgery without chemotherapy.
- Grade 3 in your report: Cells look very abnormal with rapid division. More aggressive biology — usually more intensive treatment, often chemotherapy, and closer surveillance after treatment. Does not mean untreatable.
- High grade ≠ terminal: Grade 3 breast cancer responds better to chemotherapy than Grade 1. High-grade DLBCL lymphoma is cured with R-CHOP in 60–70% of patients. Grade 3 triple-negative breast cancer achieves pCR in 40–60% with neoadjuvant chemotherapy.
- Grade and stage can diverge: A small Stage I Grade 3 tumor may be treated more aggressively than a larger Stage II Grade 1 tumor. Never evaluate grade alone.
- Grade can change over time: Some cancers dedifferentiate at recurrence — initially low-grade tumors can become higher grade. Follicular lymphoma can transform into DLBCL (high-grade transformation). Repeat biopsy at recurrence is important for this reason.
Discuss both your cancer grade and cancer stage with your oncologist — together, they determine treatment intensity, clinical trial eligibility, and long-term surveillance. Visit your cancer checkup guide to learn how grading fits into the diagnostic workup.
Frequently Asked Questions
Sources
- National Cancer Institute — Tumor Grade Fact Sheet
- American Cancer Society — Understanding Your Pathology Report
- Epstein JI et al. — 2014 ISUP Consensus Conference on Gleason Grading (Grade Groups), Am J Surg Pathol 2016
- Elston CW, Ellis IO — Nottingham Grading System for Invasive Breast Cancer, J Clin Pathol 1991
- Sparano JA et al. — TAILORx Trial (Oncotype DX in early breast cancer), NEJM 2018/2019
- WHO Classification of Tumours of the Digestive System 2019 — NET Ki-67 Grading
- WHO Classification of Tumours of the Central Nervous System 2021 — Molecular-Integrated Glioma Grading
This article is for educational purposes only and does not constitute medical advice. Cancer grade, prognosis, and treatment options should be discussed with your oncologist and pathologist.
Pingback: Cancer Second Opinion: When and How to Get One - Horizon Health Guide