
A mammogram is a low-dose X-ray examination of the breast. It is the primary tool used for breast cancer screening in average-risk women and the standard first imaging study when a breast symptom — a new lump, nipple discharge, or skin change — requires evaluation. Despite being among the most commonly ordered imaging tests in medicine, many women approach their first mammogram with significant anxiety about what will happen, whether it will hurt, and what the results will mean.
That anxiety is compounded by a statistical reality: approximately 10% of women who undergo a screening mammogram are called back for additional imaging. For the majority, that callback does not end in a cancer diagnosis — it ends in a second set of images and a normal result. But receiving a callback without having been told in advance that this is common and usually benign creates unnecessary fear. This article is designed to be the resource you read before, not after, your mammogram appointment.
This guide covers what types of mammograms exist, how to prepare for the exam, what happens during the procedure, how to read the BI-RADS score in your results letter, how 2D and 3D mammography differ, what the evidence says about radiation safety, and how mammogram costs work under U.S. insurance.
Types of Mammograms
Before the procedure itself, it helps to understand what type of mammogram you are having — because this affects what to expect during and after the appointment.
Performed on women with no current breast symptoms. Goal: detect cancer before it causes signs. Standard 4 images (2 per breast). Results read later by radiologist and sent within 1–30 days. Covered without cost-sharing under ACA for eligible women.
Performed for a specific clinical reason: palpable lump, nipple discharge, abnormality on prior screening, or callback follow-up. Additional views taken. Radiologist may interpret in real time. May include ultrasound at the same appointment. Typically subject to cost-sharing.
Standard since the 2000s. Captures a flat X-ray image per view. Widely available. Effective baseline technology for screening — still used where 3D is not available.
FDA-approved 2011. Acquires multiple images from different angles; reconstructed into 1mm slices. Detects 27–41% more invasive cancers vs 2D alone, with 15% fewer callbacks. Radiation dose similar to 2D. ACR recommended when available.
How to Prepare for a Mammogram
Proper preparation takes less than five minutes but meaningfully improves image quality and reduces the likelihood of needing repeat images.
No deodorant, antiperspirant, powder, lotion, or perfume under arms or on breasts. Metallic particles in these products appear as calcifications on the image and can trigger callbacks.
Two-piece outfit (top and separate pants or skirt) — you will remove clothing from the waist up. Remove chest and neck jewelry before or at the facility.
If you menstruate, schedule the week after your period begins. Breast tissue is less tender in this phase. Premenstrual tenderness can make compression more uncomfortable.
Arrange transfer of prior mammogram images from other facilities. Comparison to prior years is one of the most powerful tools a radiologist has for finding interval changes.
Inform the mammography technologist about: breast implants (requires additional displacement views); prior breast surgery (lumpectomy, reduction, biopsy — creates scar tissue visible on images); current pregnancy or breastfeeding; personal history of breast cancer or breast symptoms.
What to Expect During a Mammogram
Understanding what happens in the exam room reduces the anxiety that comes from imagining the unknown. The complete appointment for a standard screening mammogram takes approximately 15 to 30 minutes. The actual X-ray exposure for all four images combined takes only a few seconds.
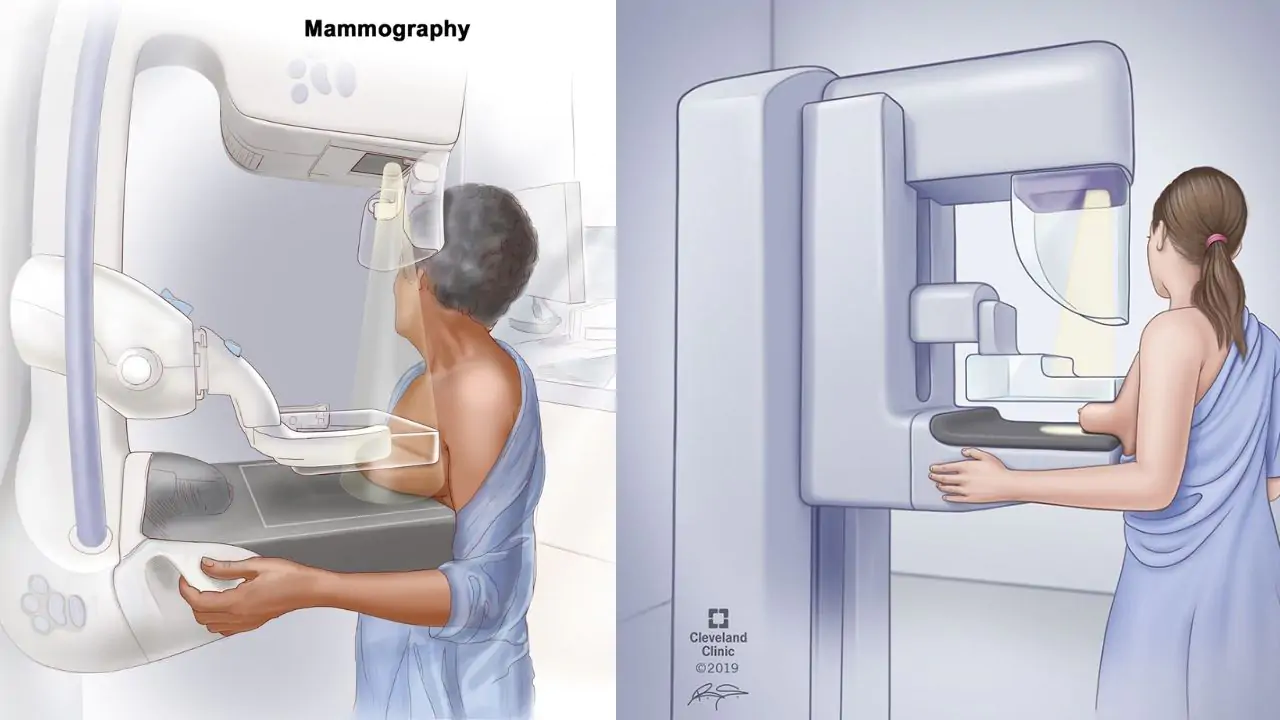
Positioning and Compression
You will stand at the mammography unit. A trained mammography technologist will position each breast on a flat imaging platform. A compression paddle is then lowered to flatten the breast against the detector.
Why compression is necessary: Compression reduces breast thickness so less radiation is needed; it separates overlapping tissue layers that can hide cancers; and it holds the breast still during the brief exposure to prevent motion blur. Without adequate compression, image quality drops significantly.
How much pressure: Approximately 25–40 lbs (111–178 N) of force, regulated by MQSA not to exceed 45 lbs (200 N). The compression feels like firm squeezing pressure and lasts only 10 to 20 seconds per image position. If the compression feels genuinely painful rather than just uncomfortable, tell the technologist — she can adjust positioning or apply slightly less pressure.
Views and Images
Standard screening mammogram: four images total — craniocaudal (CC: top-down view) and mediolateral oblique (MLO: angled side view) for each breast. The MLO view is angled at approximately 45–60 degrees and includes the axillary tail of the breast where a significant proportion of breast tissue and lymph nodes lie. Diagnostic mammograms include these plus additional targeted views depending on the area of concern.
After the Exam
No restrictions or recovery time are required after a mammogram. You can return to normal activities immediately. Your results will be communicated within 1–30 days depending on the facility.
Understanding Your Mammogram Results
When to Expect Results
Federal law (MQSA) requires mammogram results to be communicated to patients within 30 days. In practice, most facilities report within 1–2 weeks; many now post results to patient portals within 1–3 business days. For a normal result, you receive a brief letter or portal message with the result and your recommended return interval. For an abnormal result, facilities typically call directly. If you have not received results within 30 days, contact the imaging facility.
BI-RADS Categories
Every mammogram report includes a BI-RADS (Breast Imaging Reporting and Data System) score — a standardized system developed by the American College of Radiology that tells both clinicians and patients what was found and what to do next:
| BI-RADS | Finding | Recommended Action |
|---|---|---|
| 0 | Incomplete — additional imaging needed | Diagnostic mammogram, ultrasound, or MRI |
| 1 | Negative — no abnormality found | Routine next scheduled screening |
| 2 | Benign finding — clearly not cancer | Routine next scheduled screening |
| 3 | Probably benign — <2% malignancy risk | 6-month short-interval follow-up mammogram |
| 4A | Low suspicion — 2–10% malignancy risk | Core needle biopsy recommended |
| 4B | Moderate suspicion — 10–50% malignancy risk | Core needle biopsy recommended |
| 4C | High suspicion — 50–95% malignancy risk | Core needle biopsy recommended |
| 5 | Highly suggestive of malignancy — >95% | Biopsy required |
| 6 | Known biopsy-proven malignancy | Treatment planning imaging |
What a Callback Means
A BI-RADS 0 result means additional imaging is needed before the radiologist can make a final assessment — not that cancer has been found. This is the most common “abnormal” mammogram result. Approximately 10% of screening mammograms result in a callback. Of women called back:
- Approximately 90% are cleared with additional imaging alone (diagnostic mammogram views, targeted ultrasound)
- Approximately 10% are recommended for biopsy
- Of those biopsied: approximately 20–25% are diagnosed with cancer; 75–80% have benign findings
If a biopsy is recommended (BI-RADS 4 or 5), core needle biopsy — guided by ultrasound or stereotactic (mammogram) technique — is the standard outpatient procedure. It is performed under local anesthesia through a small puncture, with no surgical incision, and results typically return within 2–5 business days. For a complete guide to what to ask at every stage, see the cancer questions for doctor guide.
2D vs 3D Mammography — What the Evidence Shows
How They Differ
In 2D mammography, all breast tissue is compressed into one flat image per view. When tissue layers overlap, a cancer can be hidden behind normal tissue (a false negative) or normal structures can stack in a pattern that mimics a mass (a false positive requiring a callback). In dense breast tissue, both problems are amplified.
3D mammography (digital breast tomosynthesis) resolves the overlap problem by acquiring images at multiple angles — typically 11 to 25 exposures across an arc — and reconstructing them into thin (1 mm) slices. A radiologist scrolls through these slices one at a time, separating tissue structures that would overlap on a single 2D view. Modern DBT systems generate a synthetic 2D image from the tomosynthesis data, so a separate 2D acquisition is usually not needed.
Clinical Evidence
The landmark U.S. study is Friedewald SM et al. (JAMA 2014), analyzing 454,850 screening examinations at 13 academic and community sites before and after implementing DBT:
- Invasive cancer detection rate: Increased 41% with DBT (1.0 vs 0.7 per 1,000 screened)
- All-cancer detection: Increased 29% (1.2 vs 0.93 per 1,000)
- Recall rate (callbacks): Decreased 15% — meaning fewer false-positive callbacks
3D mammography simultaneously catches more cancers and produces fewer unnecessary callbacks — improvement in both sensitivity and specificity. Radiation dose with combined DBT plus synthetic 2D is approximately 0.4–0.5 mSv, similar to 2D FFDM alone.
Mammogram Safety and Radiation
A standard 2-view-per-breast mammogram delivers approximately 0.4 mSv of effective radiation dose. To put that in context:
- Natural background radiation in the U.S.: approximately 3 mSv per year (about 0.008 mSv per day)
- One mammogram = approximately 7 weeks of natural background radiation
- A cross-country airplane flight (New York to Los Angeles): approximately 0.04 mSv — a mammogram is roughly equivalent to 10 such flights
- Chest X-ray: approximately 0.1 mSv — one mammogram is roughly 4 chest X-rays
The lifetime cancer risk from routine mammography screening — one mammogram per year for 30 years — is estimated to be extremely small, orders of magnitude smaller than the benefit from early breast cancer detection. Radiation is not a meaningful reason to delay or avoid a mammogram.
MQSA Certification
The Mammography Quality Standards Act (1992) requires all U.S. mammography facilities to be certified. Certification requirements include: annual FDA-approved facility inspection; annual equipment physics testing; radiologists must have completed at least 60 hours of breast imaging training and read a minimum of 960 mammograms per 24 months; and equipment must meet image quality and dose standards. When scheduling a mammogram, confirm the facility is MQSA-certified. You can verify certification at the FDA’s MQSA program website.
Mammogram Cost and Insurance
ACA coverage (Section 2713): ACA-compliant health plans must cover screening mammograms without any cost-sharing — no copay, no deductible, no coinsurance for the screening mammogram itself.
Medicare Part B: Covers one screening mammogram per year for women age 40 and older at 100% — no cost to the patient when the provider accepts Medicare assignment.
Diagnostic mammogram coverage: Unlike screening mammograms, diagnostic mammograms are typically subject to standard cost-sharing. If your screening mammogram leads to a callback and a follow-up diagnostic mammogram, you may receive a bill. Understanding this difference before a callback occurs helps you avoid a financial surprise during an already stressful time.
Uninsured: The National Breast and Cervical Cancer Early Detection Program (NBCCEDP), administered by the CDC through state health departments, provides free or low-cost mammograms to low-income, uninsured, and underinsured women. Eligibility varies by state. Contact your state health department or visit the National Cancer Institute for programs in your area.
For a deeper look at when to begin breast cancer screening, how often to screen, and what guidelines apply based on your risk level, see the breast cancer screening guidelines article. For a complete overview of breast cancer types, stages, and treatment, see the breast cancer overview. For signs that should prompt earlier evaluation, see the breast cancer symptoms guide.
Frequently Asked Questions
- Friedewald SM et al. — Breast cancer screening using tomosynthesis in combination with digital mammography; JAMA 2014;311(24):2499–2507
- Gøtzsche PC & Jørgensen KJ — Screening for breast cancer with mammography; Cochrane Database Syst Rev 2013
- Hubbard RA et al. — Cumulative probability of false-positive recall or biopsy recommendation after 10 years of screening mammography; Ann Intern Med 2011
- U.S. FDA — Mammography Quality Standards Act and Program
- National Cancer Institute — cancer.gov/types/breast/screening-fact-sheet
This article is for educational purposes only and does not constitute medical advice. All screening decisions should be made in consultation with a qualified healthcare provider based on individual risk factors, history, and clinical context.
Advances in Mammography Technology
Mammography technology has evolved significantly since its introduction as a screening tool, with key innovations improving both sensitivity (ability to detect cancers that are present) and specificity (ability to avoid false positives from findings that are not cancers).
Digital breast tomosynthesis (3D mammography): DBT — which acquires multiple low-dose X-ray images through the breast at different angles and reconstructs them into a three-dimensional image set — has replaced standard 2D digital mammography as the preferred technology at most U.S. breast imaging centers. DBT improves cancer detection rate by approximately 40% compared to 2D digital mammography (studies show an additional 1.2–2.7 cancers per 1,000 screens) and reduces recall rate (false positive callbacks) by approximately 15%. The FDA has cleared numerous DBT systems, and the latest generation of DBT reconstructs both 3D images and synthetic 2D images from the same acquisition, eliminating the need for a separate 2D exposure.
Contrast-enhanced mammography (CEM): CEM uses an iodine-based intravenous contrast agent with dual-energy mammographic acquisitions to identify areas of tumor angiogenesis (abnormal blood vessel formation associated with malignancy). CEM has sensitivity similar to breast MRI for detecting breast cancer while using equipment available at most breast imaging centers rather than requiring a dedicated MRI scanner. It is emerging as an alternative to MRI for supplemental screening in women at intermediate risk or for problem-solving.
AI-assisted mammography reading: Artificial intelligence algorithms for mammography reading have received FDA clearance and are increasingly deployed at mammography programs to assist radiologists in identifying subtle findings. Studies evaluating AI-assisted reading show either non-inferiority to radiologist reading alone or modest improvements in sensitivity, with potential applications including triage of the reading workload (prioritizing cases with suspicious findings for earlier reading), second-read assistance, and supporting radiologists reading high volumes of cases. AI in mammography remains an area of active development and regulatory evaluation.
For guidance on mammography — including what to expect during the procedure, how to prepare, and how to interpret results — see our main guide to mammography. For guidance on who should have mammograms and at what intervals, see our article on breast cancer screening. For information about breast cancer risk factors that may affect your screening schedule, see our guide to breast cancer risk factors.
Pingback: Mammogram Screening: A Complete Guide by Age and Risk Level - Horizon Health Guide