Atrial Fibrillation and Stroke Risk: What to Know
Atrial fibrillation and stroke risk are linked by one of the most clinically important and preventable associations in cardiovascular medicine. AF is the most common sustained cardiac arrhythmia, affecting an estimated 33 to 44 million people worldwide, and it increases the risk of ischemic stroke by approximately 5-fold compared to people without AF — independently of all other risk factors. In older adults with additional risk factors, this relative risk can translate to an absolute annual stroke risk of 10 to 15 percent per year without anticoagulation treatment.
What makes this relationship so critical from a public health perspective is that the stroke risk conferred by AF is largely preventable: anticoagulation therapy with direct oral anticoagulants (DOACs) reduces AF-related stroke by 60 to 70 percent compared to no treatment, and is substantially more effective than antiplatelet therapy (aspirin reduces AF-related stroke by only 20 percent, at the cost of significant bleeding risk). Yet studies consistently show that a large proportion of patients with AF and high stroke risk remain either untreated with anticoagulation or treated subtherapeutically — often because of physician or patient concerns about bleeding, or because the stroke risk without treatment is underestimated relative to the bleeding risk of treatment.
Understanding how AF causes stroke, how stroke risk is quantified in AF patients, what treatment is indicated, and how the treatment decision is made helps patients and families engage effectively with the clinical decisions that determine their long-term stroke risk.
How Atrial Fibrillation Causes Stroke — The Left Atrial Appendage
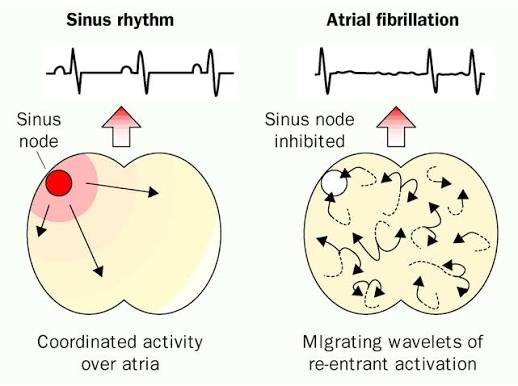
The mechanism by which AF causes stroke reflects the pathophysiology of the fibrillating atria. In normal sinus rhythm, the atria contract in an organized, coordinated wave that empties blood efficiently into the ventricles with each beat. In AF, the atria receive chaotic electrical impulses at 350 to 600 times per minute — far faster than any organized contraction is possible — and instead of contracting, they quiver. This fibrillatory motion eliminates the normal atrial pumping action, producing two consequences that promote thrombosis.
First, blood stagnates in the left atrium — particularly in the left atrial appendage (LAA), a narrow, trabeculated pouch where flow is always somewhat sluggish and where the normal atrial contraction is most important for clearing pooled blood. In AF, the LAA becomes a reservoir of stagnant blood where all three components of Virchow’s triad for thrombosis are present: stasis of blood, endothelial dysfunction from the chronically elevated wall stress and inflammation of AF, and a hypercoagulable state (elevated fibrinogen, von Willebrand factor, and other procoagulant markers in AF patients). This combination promotes thrombus formation in the LAA, where approximately 90 percent of left atrial thrombi in non-valvular AF originate.
Second, when a thrombus or thrombus fragment breaks off from the LAA and enters the systemic circulation, it travels into the aorta and then into the cerebral arterial circulation — where the relatively large size of cardiac emboli (compared to atherosclerotic emboli) tends to occlude larger arteries (the middle cerebral artery, anterior cerebral artery, or posterior cerebral artery), producing large cortical infarcts. AF-related cardioembolic strokes are typically among the most severe strokes clinically — causing significant aphasia, hemiplegia, hemisensory loss, visual field defects, or neglect — and have higher in-hospital mortality and worse long-term functional outcomes than lacunar or small vessel strokes.
The relationship between AF and stroke is also notable for being independent of AF symptom burden. Paroxysmal AF (which self-terminates within 7 days) carries comparable stroke risk to persistent or permanent AF per unit of AF burden — and silent, asymptomatic AF (detected only by ECG or long-term monitoring rather than symptoms) carries the same stroke risk as symptomatic AF. This means the presence of AF on any ECG, regardless of symptoms, triggers the same anticoagulation decision-making process.
Quantifying Stroke Risk in AF — The CHA₂DS₂-VASc Score
Because not all patients with AF have the same absolute stroke risk — a 45-year-old with lone AF and no other risk factors has a very different annual stroke risk than a 78-year-old with AF, hypertension, diabetes, and prior stroke — stroke risk stratification tools are used to identify which AF patients have sufficiently high risk to warrant anticoagulation. The CHA₂DS₂-VASc score is the internationally recommended tool for this purpose, with each letter representing a risk factor:
C — Congestive heart failure (1 point): Impaired LV function or heart failure increases embolic risk from reduced cardiac output and atrial remodeling.
H — Hypertension (1 point): The most common risk factor in AF patients, contributing both to AF development and to stroke risk independently.
A₂ — Age 75 or older (2 points): Advanced age is one of the strongest stroke risk predictors in AF and receives double weighting.
D — Diabetes mellitus (1 point): Diabetes promotes endothelial dysfunction and a procoagulant state that amplifies AF-related thrombosis risk.
S₂ — Prior Stroke or TIA (2 points): Prior cerebrovascular events are the strongest predictor of future stroke and receive double weighting.
V — Vascular disease (1 point): Prior MI, peripheral arterial disease, or aortic plaque increases cardiovascular event risk.
A — Age 65 to 74 (1 point): Intermediate age-related risk, receiving single weighting (in addition to the A₂ above).
Sc — Sex category female (1 point): Female sex is a stroke risk modifier in AF (females with other risk factors have higher absolute stroke risk than males with comparable CHA₂DS₂-VASc scores).
The maximum CHA₂DS₂-VASc score is 9. Score interpretation for anticoagulation decisions: a score of 0 in males or 1 in females (the 1 point from female sex alone) represents sufficiently low risk that anticoagulation is not recommended. A score of 1 in males (one additional risk factor beyond sex) represents an intermediate risk where anticoagulation may be considered. A score of 2 or more (regardless of sex) represents high enough annual stroke risk (estimated 2 to 15 percent per year depending on specific score) that anticoagulation is recommended unless clear contraindications exist.

Anticoagulation for AF Stroke Prevention — DOAC vs Warfarin
The landmark RE-LY, ROCKET-AF, ARISTOTLE, and ENGAGE AF-TIMI 48 trials established DOACs (dabigatran, rivaroxaban, apixaban, and edoxaban respectively) as the preferred anticoagulants for non-valvular AF stroke prevention, replacing warfarin as the previous standard for most patients. The four pivotal trial results demonstrate consistently that DOACs provide equivalent or superior stroke/systemic embolism prevention compared to warfarin, with significantly lower rates of intracranial hemorrhage (the most feared and often fatal bleeding complication of anticoagulation).
The key advantages of DOACs over warfarin include: predictable pharmacokinetics that eliminate the need for routine INR monitoring; fewer drug-drug and drug-food interactions; faster onset and offset of anticoagulant effect (simplifying management around procedures); and the availability of specific reversal agents (idarucizumab for dabigatran, andexanet alfa for factor Xa inhibitors) that can rapidly reverse anticoagulation in emergency situations. The primary limitation is higher cost than warfarin and the requirement for adequate renal function (all DOACs are renally cleared to varying degrees, with dabigatran most dependent on renal clearance).
Apixaban has the most favorable net clinical benefit across the broadest patient population in AF, based on its combination of effective stroke prevention, the lowest major bleeding rates of any DOAC, and the most compelling data in patients with CKD and advanced age. The ARISTOTLE trial showed apixaban superior to warfarin for both stroke prevention (21 percent relative risk reduction) and major bleeding (31 percent relative risk reduction) simultaneously — an unusual finding in anticoagulation trials where bleeding and efficacy are typically in tension.
Warfarin (with target INR 2.0 to 3.0) remains appropriate for specific AF populations: patients with mechanical heart valves (where DOACs are contraindicated based on the RE-ALIGN trial showing worse outcomes with dabigatran versus warfarin in mechanical valves) and patients with mitral stenosis (where DOACs are not approved). For patients with severe renal impairment (CrCl below 15 to 25 mL/min depending on the DOAC), warfarin or careful DOAC dose adjustment under specialist guidance may be preferred.
AF Stroke Prevention Beyond Anticoagulation
Anticoagulation is the cornerstone of AF stroke prevention, but several additional strategies are available or under active investigation:
Left atrial appendage occlusion (LAAO): For patients with AF and high stroke risk who have contraindications to long-term anticoagulation (most commonly prior major bleeding events — gastrointestinal bleeding or intracranial hemorrhage), percutaneous LAA occlusion with devices (the WATCHMAN and WATCHMAN FLX devices are FDA-approved in the US) provides an alternative stroke prevention strategy. By sealing the LAA with a plug-like device, clots can no longer form in this structure and embolize to the brain. The PROTECT AF and PREVAIL trials demonstrated non-inferiority of WATCHMAN to warfarin for stroke prevention with lower rates of hemorrhagic stroke and non-procedure bleeding after the initial implant period. LAAO is now a guideline-supported option (Class IIb, Level B) for patients with AF, high stroke risk, and contraindications to long-term anticoagulation.
Rate control versus rhythm control: For many years, AF management focused on whether restoring and maintaining sinus rhythm (rhythm control, through antiarrhythmic drugs or catheter ablation) was superior to simply controlling the ventricular rate in AF (rate control). The AFFIRM trial (2002) showed no survival advantage of rhythm control over rate control with anticoagulation in older AF patients. However, the more recent EAST-AFNET 4 trial (2020) showed that early rhythm control (initiated within 1 year of AF diagnosis using catheter ablation or antiarrhythmic drugs) was associated with a 21 percent reduction in cardiovascular death, stroke, and hospitalization for heart failure compared to rate control — representing a shift toward earlier rhythm restoration in appropriate candidates. Critically, in both strategies, anticoagulation based on stroke risk is continued regardless of whether sinus rhythm is restored, because rhythm control does not reliably eliminate silent AF recurrences.
Catheter ablation: Pulmonary vein isolation (PVI) by catheter ablation — disconnecting the triggers for AF that arise in the pulmonary veins from the left atrium — has emerged as the most effective rhythm control strategy, particularly for paroxysmal AF. The CASTLE-AF trial demonstrated that ablation in AF patients with heart failure significantly reduced mortality and cardiovascular hospitalization. The CABANA trial showed ablation was superior to drug therapy for AF symptom control. However, the impact of ablation on stroke risk — as distinct from symptom control — remains under investigation, and current guidelines recommend continuing anticoagulation based on CHA₂DS₂-VASc score even after successful ablation.
The American Stroke Association’s AFib and stroke page explains the connection between atrial fibrillation and stroke risk for patients. The CDC atrial fibrillation information covers prevalence, stroke risk, and treatment options. The NHLBI AF treatment guide reviews anticoagulation options and stroke prevention strategies.
Related reading: Atrial Fibrillation: Symptoms and Risks | What Is a Stroke? | Ischemic vs Hemorrhagic Stroke | High Blood Pressure and Stroke | Mini-Stroke (TIA)
Sources
- Connolly SJ, et al. Dabigatran versus Warfarin in Patients with Atrial Fibrillation (RE-LY). N Engl J Med. 2009;361(12):1139-1151.
- Granger CB, et al. Apixaban versus Warfarin in Patients with Atrial Fibrillation (ARISTOTLE). N Engl J Med. 2011;365(11):981-992.
- Hindricks G, et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation. Eur Heart J. 2021;42(5):373-498.
- Wolf PA, et al. Atrial Fibrillation as an Independent Risk Factor for Stroke (Framingham Study). Stroke. 1991;22(8):983-988.
- Lip GYH, et al. Refining Clinical Risk Stratification for Predicting Stroke and Thromboembolism in AF: CHA2DS2-VASc. Chest. 2010;137(2):263-272.
Bleeding Risk Assessment — The Other Side of the Anticoagulation Decision
The decision to anticoagulate a patient with AF involves weighing stroke prevention benefit against bleeding risk — but the contemporary evidence strongly supports the conclusion that for most AF patients with a CHA₂DS₂-VASc score of 2 or above, the stroke prevention benefit of anticoagulation substantially outweighs the bleeding risk, particularly when DOACs are used instead of warfarin.
The HAS-BLED score is the most widely used bleeding risk assessment tool in AF management, incorporating: uncontrolled Hypertension, Abnormal renal or liver function, Stroke history, Bleeding history or predisposition, Labile INR (for warfarin users), Elderly age (above 65), and Drugs (antiplatelets, NSAIDs) or alcohol. A HAS-BLED score of 3 or above identifies patients at higher bleeding risk who warrant closer monitoring and attention to modifiable bleeding risk factors — but critically, the HAS-BLED score is not intended to identify patients who should not receive anticoagulation. Rather, it is intended to identify patients in whom modifiable bleeding risk factors (uncontrolled hypertension, concurrent antiplatelet use, alcohol excess, labile INR) should be actively addressed alongside anticoagulation initiation.
An important clinical insight from comparative risk analyses is that the most feared complication of anticoagulation — intracranial hemorrhage — is dramatically less common with DOACs than with warfarin (the ARISTOTLE trial showed a 58 percent relative reduction in intracranial hemorrhage for apixaban versus warfarin; similar reductions were seen for other DOACs). Since intracranial hemorrhage from anticoagulation is typically fatal or severely disabling, while most extracranial bleeding events (gastrointestinal bleeding, bruising, hematoma) are manageable and recoverable, the DOAC-associated reduction in intracranial hemorrhage substantially changes the net clinical benefit calculation compared to the warfarin era.
The most common reason anticoagulation is withheld in AF patients who should receive it is physician and patient concern about falls — the fear that a patient who falls will develop fatal intracranial hemorrhage on anticoagulation. Multiple studies have examined this concern directly, and the consistent finding is that a patient must fall approximately 295 times per year before the added bleeding risk from anticoagulation outweighs the stroke prevention benefit in a typical AF patient with a CHA₂DS₂-VASc score of 2 or above. Even in patients who fall repeatedly, the annual stroke risk of untreated AF in high-risk patients (5 to 15 percent per year) dramatically exceeds the annual bleeding risk from anticoagulation in fallers (~1 to 2 percent fatal or severe intracranial hemorrhage risk). Falls are not a contraindication to anticoagulation in AF.
Screening for Silent AF — Who Should Be Tested
A substantial proportion of AF-related strokes occur in patients who were not previously known to have AF — in some series, up to 25 to 30 percent of cardioembolic strokes reveal new AF as the likely causative mechanism during the acute evaluation. This reflects the high prevalence of silent (asymptomatic) AF, which produces no symptoms but carries the same stroke risk as symptomatic AF. Population-based screening for AF — identifying individuals with silent AF before their first stroke — is therefore an active area of policy and research.
Current evidence supports opportunistic AF screening with a pulse check or single-lead ECG recording in adults aged 65 and above — a recommendation included in several national guidelines. A pulse that is irregular in rate and rhythm should prompt a formal 12-lead ECG, and a resting 12-lead ECG positive for AF in an otherwise asymptomatic individual triggers the full CHA₂DS₂-VASc evaluation and anticoagulation decision. The 2019 STROKESTOP trial in Sweden demonstrated that systematic invitation for ECG screening in 75 and 76-year-olds identified significantly more AF cases than routine care and was associated with fewer strokes in the screened group over the study period.
Consumer wearables with photoplethysmography (PPG) heart rate sensors have emerged as novel AF detection tools — the Apple Watch’s Irregular Rhythm Notification and atrial fibrillation history features, and the KardiaMobile single-lead ECG device by AliveCor, have both received FDA clearance for AF detection. Large studies including the Apple Heart Study (419,093 participants) demonstrated that smartwatch-based irregular pulse notifications had a positive predictive value of 84 percent for AF, and approximately one-third of notified participants were found to have AF on confirmatory patch monitoring. These technologies are expanding AF detection in the general population but require physician evaluation to confirm the diagnosis and initiate appropriate treatment — a positive wearable signal should always be followed by formal clinical evaluation.
AF Stroke After Cardioversion — Managing the Transition Risk
Cardioversion — the restoration of sinus rhythm either electrically (synchronized DC cardioversion) or pharmacologically (with antiarrhythmic drugs such as flecainide, propafenone, or ibutilide) — carries a specific stroke risk that requires careful anticoagulation management. When AF terminates and sinus rhythm is restored, the atria resume organized contractions — but the LAA may remain stunned (mechanically dysfunctional despite electrical restoration of sinus rhythm) for days to weeks, during which clots that formed during AF or the peri-cardioversion period can embolize.
The peri-cardioversion stroke risk is managed through two established protocols: (1) therapeutic anticoagulation for at least 3 to 4 weeks before cardioversion (to allow any existing LAA thrombus to dissolve) and continued for at least 4 weeks after cardioversion (until LAA stunning resolves), regardless of CHA₂DS₂-VASc score; or (2) transesophageal echocardiography (TEE) to rule out LAA thrombus, allowing cardioversion without 3 to 4 weeks of pre-anticoagulation preparation, followed by post-cardioversion anticoagulation for at least 4 weeks. The TEE-guided approach allows earlier cardioversion and is used when prompt rhythm restoration is clinically desirable — for example, in AF with hemodynamic compromise or very symptomatic patients.
After the mandatory 4-week post-cardioversion anticoagulation period, whether anticoagulation is continued long-term depends on the CHA₂DS₂-VASc score — not on whether sinus rhythm has been maintained. Because AF frequently recurs silently after successful cardioversion (even in patients who remain asymptomatic), anticoagulation cannot be safely stopped based on the absence of AF symptoms. Patients with CHA₂DS₂-VASc scores of 2 or above should continue anticoagulation indefinitely after cardioversion.
Practical Steps for AF Patients Concerned About Stroke Risk
For patients who have been diagnosed with AF — whether they have symptoms or AF was found incidentally — the following steps represent the evidence-based approach to maximizing stroke prevention:
First, ask your physician to calculate your CHA₂DS₂-VASc score explicitly, and ask what your estimated annual stroke risk is without anticoagulation. If your score is 2 or above, anticoagulation is recommended — understand the reasoning for any decision not to anticoagulate and ensure the conversation includes an explicit comparison of annual stroke risk versus annual major bleeding risk from treatment.
Second, if anticoagulation is prescribed, understand the importance of consistent adherence. Unlike most medications where missing a dose causes only modest effect attenuation, missing doses of DOAC anticoagulation for AF creates periods of inadequate stroke protection during which the risk of cardioembolic stroke returns toward the untreated level. DOACs have short half-lives (12 to 24 hours depending on the agent), meaning that consistent daily (or twice-daily) dosing is essential for continuous protection.
Third, optimize the modifiable components of your CHA₂DS₂-VASc and HAS-BLED scores simultaneously: achieve and maintain blood pressure below 130/80 mmHg (reducing both stroke risk and bleeding risk), manage diabetes aggressively, avoid concurrent NSAID use and over-the-counter aspirin without explicit physician guidance (both increase gastrointestinal bleeding risk without additional stroke prevention benefit in anticoagulated AF patients), and limit alcohol intake (alcohol both triggers AF paroxysms and increases bleeding risk).
Fourth, know the symptoms of stroke and act on them immediately. Even on anticoagulation, AF-related stroke is not completely eliminated — the 60 to 70 percent relative risk reduction means a residual stroke risk of approximately 30 to 40 percent of the untreated risk remains. FAST symptoms (Face drooping, Arm weakness, Speech difficulty, Time to call 911) in an anticoagulated AF patient require immediate emergency evaluation exactly as in any other suspected stroke.