Finding a breast lump is one of the most frightening moments a woman can experience — and one of the most common. Each year, millions of women discover a new lump or thickening in their breast or underarm and face the same urgent question: is this cancer? The answer, statistically, is usually no. Fewer than 10% of self-detected breast lumps in women under 50 are ultimately found to be malignant, and the proportion is higher in older women — but still far from inevitable.
The problem is that physical characteristics alone cannot reliably answer that question. A lump that feels soft, smooth, and mobile may still be cancer in rare cases. A lump that feels hard and fixed may be fat necrosis from old trauma. This is why the guidance from every major medical organization is consistent: any new breast lump warrants clinical evaluation, regardless of how it feels, how old you are, or whether your last mammogram was normal.
This guide explains the most common types of benign breast lumps, what features tend to be more or less concerning, how the diagnostic process works, when to seek evaluation urgently vs. soon, and what to expect at every step of a breast lump workup.
Types of Benign Breast Lumps
Most breast lumps are not cancer. Understanding the most common benign causes helps contextualize what a new lump may represent — while reinforcing why clinical evaluation is still always necessary.
Most common benign solid breast tumor in women ages 15–35. Firm, rubbery, smooth-edged, highly mobile (“marble” feel), usually painless. Simple fibroadenomas do not increase cancer risk. Complex fibroadenomas: ~1.5–2× elevated risk.
Fluid-filled sac, most common ages 35–50. Smooth, round, mobile; often tender premenstrually. Simple cysts carry no cancer risk. Complicated or complex cysts (with internal echoes or solid components) may require aspiration or biopsy.
Firm, irregular lump from trauma, surgery, or radiation to breast tissue. Can closely mimic cancer on physical exam and imaging (irregular edges, calcifications, skin retraction). Biopsy is often necessary for definitive diagnosis.
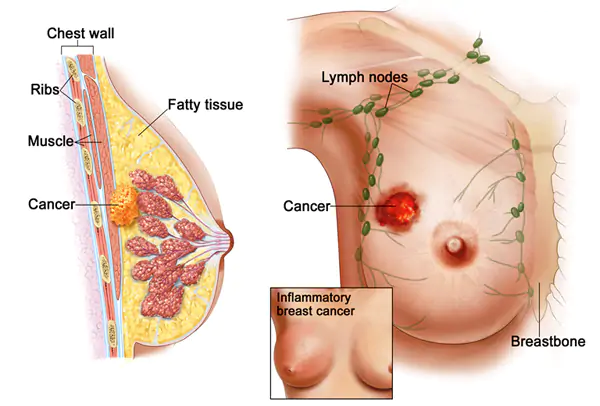
Infection of breast tissue (mastitis) or localized pus collection (abscess). Most common in breastfeeding women. Tender, warm, red area ± fever. If mastitis doesn’t respond to antibiotics in 7–10 days, inflammatory breast cancer must be ruled out.
Rare (<1% of breast tumors). Similar to fibroadenoma but grows rapidly. Can be benign, borderline, or malignant. Requires complete surgical excision with clear margins — unlike fibroadenoma, cannot be monitored alone.
Benign tumor in a breast duct; often presents with nipple discharge (bloody or clear) ± small subareolar lump. Solitary central papillomas: lower risk. Multiple peripheral papillomas: higher risk of atypia. Surgical excision is typically recommended.
What Makes a Breast Lump Suspicious?
Certain physical characteristics of a breast lump are statistically associated with higher or lower risk of malignancy. These features guide how urgently evaluation is sought — but they cannot replace imaging and biopsy. No combination of clinical features alone can reliably exclude cancer.
- Smooth, well-defined edges (easily separated from surrounding tissue)
- Soft, rubbery, or fluid-like consistency
- Highly mobile — moves freely under the finger
- Tender or painful, especially premenstrually
- Fluctuates in size or tenderness with the menstrual cycle
- Bilateral or multiple lumps
- Present for years and unchanged on prior imaging
- Hard, stone-like consistency
- Irregular or poorly defined edges
- Fixed — does not move freely under the finger
- Painless or non-tender (especially in a woman 40+)
- New lump in a postmenopausal woman
- Skin changes: dimpling, puckering, peau d’orange, redness
- Nipple changes: new retraction, inversion, or bloody discharge
- Growing in size over weeks
- Enlarged firm axillary (armpit) lymph nodes
Who Should Get a Breast Lump Evaluated — and How Fast
Within the same week (urgent): A new breast lump accompanied by skin changes (dimpling, puckering, peau d’orange, redness); new nipple retraction or bloody nipple discharge; any rapidly enlarging mass; any lump in a postmenopausal woman; any lump in a woman with a known BRCA mutation or high-risk history.
Within 1–2 weeks (prompt): Any new discrete breast lump — the standard recommendation regardless of age, tenderness, or other features. A previously evaluated lump that has changed in size, shape, or consistency.
Within 2–4 weeks (soon): Bilateral cyclical breast pain without a discrete palpable lump (mastalgia) — unlikely to represent cancer; can be assessed after one complete menstrual cycle to evaluate the cyclical pattern.
By age: Women under 25 — breast cancer rare, but any new lump should still be evaluated (ultrasound). Ages 25–50: clinical exam + imaging (ultrasound ± mammogram depending on age). Over 50: prompt evaluation; mammogram + ultrasound; malignant proportion increases with age.
The Diagnostic Process for a Breast Lump
The standard of care for evaluation of a new breast lump is the triple assessment — three independent methods that together provide near-100% diagnostic accuracy.
A trained clinician examines both breasts, characterizing the lump by size, shape, consistency, mobility, and relationship to overlying skin. Axillary and supraclavicular lymph nodes are also assessed. The clinical exam determines how urgently imaging and biopsy are needed.
Under 35: Ultrasound first — denser tissue, better ultrasound sensitivity. Ages 35–50: Both mammogram + ultrasound. Over 50: Mammogram first, then ultrasound for the mass. Results reported as BI-RADS 0–6 — BI-RADS 4 or 5 means biopsy is recommended.
Performed when imaging cannot exclude malignancy (BI-RADS 4–5). Outpatient; local anesthesia; no surgical incision; tissue cores obtained under ultrasound or mammographic guidance. Results return within 2–5 business days and provide definitive tissue diagnosis.
A benign biopsy result must be radiologic-pathologically concordant — the pathology must explain what was seen on imaging. If there is discordance (e.g., BI-RADS 4 but pathology shows only normal tissue), re-biopsy is typically performed. For a comprehensive guide to what questions to ask at each step, see the cancer questions for doctor guide.
Breast Lumps During Pregnancy and Breastfeeding
The most common breast lumps during pregnancy and breastfeeding are benign: galactoceles (milk-containing cysts), mastitis, and abscesses. However, breast cancer does occur during these periods — and because the breasts are typically enlarged and dense, new lumps may be incorrectly attributed to normal changes.
Key principles: any new discrete lump during pregnancy or breastfeeding warrants evaluation. Ultrasound is the first-line modality (no radiation; safe). Mammography is safe during pregnancy with appropriate shielding. Any solid mass not responding to antibiotics within 7–10 days should be biopsied. Core needle biopsy is safe during both pregnancy and breastfeeding.
Breast Lump vs. Breast Pain
Breast pain (mastalgia) is the most common breast symptom — affecting approximately two-thirds of women at some point in their lives. Cyclical mastalgia (bilateral pain worsening the two weeks before menstruation) is almost universally benign. If no discrete lump is felt on clinical examination, imaging is not routinely required. Non-cyclical mastalgia (unilateral or bilateral pain without a clear cyclical pattern) is more variable — a discrete tender lump with non-cyclical pain warrants imaging evaluation.
For a full list of breast changes and breast cancer symptoms to be aware of between screening appointments, see the symptoms guide. For guidance on breast cancer screening and when to start regular mammograms, see the screening article. For what to expect at a mammogram appointment, see the mammogram guide. For a complete overview of breast cancer types, stages, and treatment, see the breast cancer overview.
Frequently Asked Questions
- American Cancer Society — cancer.org — Breast cancer symptoms and signs
- National Cancer Institute — cancer.gov/types/breast
- NICE NG101 (2023) — Suspected Cancer: Recognition and Referral in Primary Care
- ACR BI-RADS Atlas 5th Edition 2013 — Breast imaging reporting and data system
- Dupont WD et al. — Breast cancer risk associated with proliferative breast disease; NEJM 1985;312:146–151
This article is for educational purposes only and does not constitute medical advice. Any new breast lump should be evaluated by a qualified healthcare provider. Do not use this information to delay seeking clinical evaluation.
Breast Cancer Treatment: Key Advances and Approaches
Breast cancer treatment has become increasingly personalized over the past two decades, driven by advances in tumor biology characterization that distinguish meaningfully different breast cancer subtypes with different biological behaviors and optimal treatment approaches. The four major molecular subtypes of breast cancer — Luminal A (hormone receptor-positive, HER2-negative, low-grade), Luminal B (hormone receptor-positive, HER2-negative, high-grade or HER2-positive), HER2-enriched (HER2-positive, hormone receptor-negative), and triple-negative (estrogen receptor-negative, progesterone receptor-negative, HER2-negative) — each have distinct prognoses, responses to systemic therapy, and optimal treatment sequencing.
Hormone receptor-positive (HR+) breast cancer: HR+ breast cancer, which accounts for approximately 70% of cases, is treated with endocrine therapy (hormone-blocking treatment) as the cornerstone of systemic therapy. For premenopausal women, tamoxifen (5–10 years) or ovarian suppression plus an aromatase inhibitor is standard. For postmenopausal women, aromatase inhibitors (anastrozole, letrozole, exemestane) have superseded tamoxifen as the preferred endocrine therapy due to superior efficacy. In metastatic HR+ breast cancer, the CDK4/6 inhibitors (palbociclib, ribociclib, abemaciclib) combined with an aromatase inhibitor or fulvestrant have transformed outcomes: the MONARCH, PALOMA, and MONALEESA trials established this combination as first-line standard of care, substantially improving progression-free and overall survival compared to endocrine therapy alone.
HER2-positive breast cancer: HER2-positive breast cancer, which accounts for approximately 15–20% of cases, was once associated with a poor prognosis but is now one of the most treatable breast cancer subtypes due to the development of HER2-targeted therapies. Trastuzumab (Herceptin) was the first anti-HER2 agent and remains a cornerstone of treatment. For early-stage HER2-positive breast cancer, neoadjuvant pertuzumab + trastuzumab + chemotherapy followed by adjuvant T-DM1 (if residual disease) is standard, based on the APHINITY and KATHERINE trials. In metastatic HER2-positive disease, trastuzumab deruxtecan (T-DXd / Enhertu) has demonstrated remarkable efficacy even in patients who have progressed through multiple prior lines of HER2-directed therapy, with response rates exceeding 60% in heavily pretreated patients (DESTINY-Breast01/02/03 trials).
Triple-negative breast cancer (TNBC): TNBC — which accounts for approximately 10–15% of breast cancers and is disproportionately common in younger women and Black women — was historically treated with cytotoxic chemotherapy alone. Several advances have improved outcomes: pembrolizumab (Keytruda) added to neoadjuvant chemotherapy for early-stage, high-risk TNBC improved event-free survival in the KEYNOTE-522 trial and is now standard for eligible patients. Olaparib (for BRCA1/2 germline mutation carriers) and sacituzumab govitecan (Trodelvy, an antibody-drug conjugate targeting Trop-2) have improved outcomes in metastatic TNBC.
For authoritative information on breast cancer, the American Cancer Society’s breast cancer resource provides patient-friendly comprehensive guides. The National Cancer Institute’s breast cancer PDQ offers evidence-based clinical summaries. The NCCN Breast Cancer Guidelines are the most widely used clinical practice standards among U.S. oncologists. For information about breast cancer symptoms that often lead to initial evaluation, see our guide to breast cancer symptoms. For information about recommended breast cancer screening approaches — including mammography and supplemental MRI for high-risk women — see our comprehensive guide to breast cancer screening. For information about what a breast lump means and how it is evaluated, see our article on breast lumps.
Breast Cancer Survivorship and Long-Term Considerations
With improving early detection and treatment advances, more than 4 million women in the United States are living after a breast cancer diagnosis — making breast cancer survivorship care an increasingly important component of oncology practice. Survivorship care addresses the long-term physical and psychological effects of breast cancer and its treatment, ongoing monitoring for recurrence, management of late effects, and promotion of healthy behaviors that may reduce recurrence risk or risk of a second primary cancer.
Surveillance after treatment: The standard surveillance approach for breast cancer survivors after completing primary treatment includes history and physical examination every three to six months for the first three years, then every six to twelve months for years four and five, then annually thereafter. Annual mammography of the treated and contralateral breast is recommended for women who had breast-conserving surgery. Breast MRI is recommended annually for high-risk survivors (BRCA mutation carriers, women who received chest radiation between ages 10–30). Routine laboratory tests, bone scans, CT scans, and PET scans are not recommended in asymptomatic survivors without specific clinical indications — evidence does not support intensive imaging surveillance for improving survival in average-risk survivors.
Endocrine therapy and bone health: Aromatase inhibitors (anastrozole, letrozole, exemestane), used for hormone receptor-positive breast cancer in postmenopausal women, reduce estrogen levels and consequently increase bone loss. Breast cancer survivors on aromatase inhibitors should have baseline bone density (DXA scan) measured and repeat scans every one to two years, with calcium and vitamin D supplementation and bisphosphonate therapy (zoledronic acid, alendronate) or denosumab (Prolia) for patients with osteoporosis or high fracture risk.
Lymphedema: Axillary lymph node dissection (ALND), performed for patients with macroscopic lymph node metastases, is a risk factor for arm lymphedema — chronic swelling of the arm, hand, or breast due to impaired lymphatic drainage. Sentinel lymph node biopsy (SLNB), which removes only the lymph node(s) most likely to contain metastatic cells, has substantially reduced lymphedema risk compared to ALND. Patients who develop lymphedema are managed with compression garments, manual lymphatic drainage, complete decongestive therapy, and avoidance of constriction or injury to the affected arm.
Cognitive effects: Some breast cancer survivors report cognitive difficulties — including problems with memory, attention, and processing speed — during and after chemotherapy treatment. This “chemobrain” or “chemofog” phenomenon is real and recognized, though its biological mechanisms are incompletely understood. Cognitive rehabilitation programs, aerobic exercise, and management of contributing factors (sleep disturbance, depression, anxiety, menopause symptoms) may be helpful.
Fertility and premature menopause: Chemotherapy and ovarian suppression in young women with breast cancer can cause premature menopause and infertility. Women who wish to preserve fertility should be referred to a reproductive endocrinologist before starting treatment for fertility preservation options (embryo or oocyte cryopreservation). Temporary ovarian suppression with GnRH agonists during chemotherapy may reduce gonadotoxicity, though this approach’s efficacy for fertility preservation remains an area of ongoing study.
Breast cancer is the most commonly diagnosed cancer in women in the United States (excluding skin cancers) and the second leading cause of cancer death in women, after lung cancer. Approximately 310,000 women and 2,800 men are diagnosed with invasive breast cancer each year in the United States. An additional 56,000 cases of ductal carcinoma in situ (DCIS), a non-invasive precursor, are diagnosed annually. Despite its frequency, breast cancer outcomes have improved substantially over the past three decades due to advances in early detection through mammography and improvements in systemic therapy. With early detection and appropriate treatment, the prognosis for breast cancer — particularly for hormone receptor-positive subtypes diagnosed at localized or regional stages — is excellent. The five-year relative survival for all stages combined exceeds 90%, and for localized disease approaches 100%. Continued investment in screening adherence, access to multidisciplinary oncology care, and clinical trial participation for eligible patients are the highest-priority strategies for further improving breast cancer outcomes at the population level.
Pingback: Nipple Discharge: When Is It a Sign of Cancer? - Horizon Health Guide