Varicose Veins vs Poor Circulation: Key Differences
Varicose veins and poor circulation are frequently discussed together — and for good reason. Varicose veins are among the most visible signs of impaired venous circulation in the legs, and the venous insufficiency that causes them is one of the two major forms of poor leg circulation (the other being arterial insufficiency from peripheral artery disease). Understanding the relationship between varicose veins and poor circulation — how they overlap, how they differ, and which type of circulatory problem you may be dealing with — is the foundation of appropriate evaluation and treatment.
Approximately 23 percent of adults have varicose veins — making them one of the most common vascular conditions in primary care — yet the majority of people with varicose veins do not know whether they represent a cosmetic issue only or a clinical sign of significant venous disease. Meanwhile, arterial poor circulation (from peripheral artery disease) produces an entirely different set of symptoms and risks that are frequently confused with venous poor circulation. Distinguishing between these conditions guides the appropriate diagnostic workup and prevents the serious error of treating the wrong type of circulatory problem.
What Are Varicose Veins? Anatomy and Formation
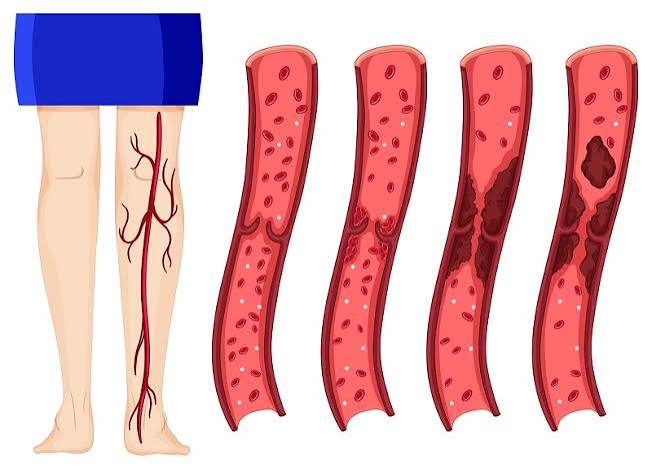
Varicose veins are abnormally dilated, tortuous superficial veins — most commonly affecting the great saphenous vein and its tributaries on the medial (inner) aspect of the calf and thigh, and the small saphenous vein on the posterior calf. They appear as blue-purple, rope-like, raised structures visible beneath the skin, often following a serpentine course and measuring 3 to 10 millimeters or more in diameter.
Varicose veins form when the one-way valves within the superficial veins become incompetent — failing to close properly after each heartbeat and allowing blood to flow backward (reflux) toward the foot rather than forward toward the heart. This venous reflux causes blood to pool in the superficial veins, gradually dilating them under the increased hydrostatic pressure. The saphenofemoral junction (where the great saphenous vein joins the deep femoral vein at the groin) is the most common location of initial valve failure — incompetence here allows reflux to propagate down the great saphenous vein, eventually producing varicosities in the calf and ankle region.
Several factors predispose to varicose vein development: female sex (progesterone relaxes vein wall smooth muscle and reduces valve competence; pregnancy additionally increases intra-abdominal venous pressure and blood volume); prolonged standing or sitting occupations (gravity imposes prolonged hydrostatic load on leg vein valves); family history (50 to 80 percent of varicose vein patients have an affected first-degree relative — genetic factors determine vein wall collagen composition and valve structure); obesity (increases intra-abdominal pressure, compressing the inferior vena cava and pelvic veins); prior deep vein thrombosis (DVT destroys deep vein valves during recanalization, causing secondary venous insufficiency that overwhelms the superficial vein system); and advanced age (cumulative valve wear over decades).
Varicose Veins as a Sign of Poor Circulation — the Venous Connection
Varicose veins are a sign of venous poor circulation — specifically, chronic venous insufficiency (CVI), a condition in which the venous return mechanism from the lower extremities is impaired. The severity of venous poor circulation exists on a spectrum from isolated cosmetic varicose veins at one end to severe chronic venous insufficiency with venous ulceration at the other:
Class 1 (Telangiectasias and reticular veins): The mildest form — thread veins (spider veins, less than 1 mm) and reticular veins (1 to 3 mm) representing superficial venous dilation without significant hemodynamic reflux. Primarily cosmetic; rarely associated with symptoms beyond occasional mild aching or cosmetic concern.
Class 2 (Varicose veins): Dilated superficial veins more than 3 mm — the classic varicose vein presentation. Often symptomatic with leg heaviness, aching, fatigue, itching, and swelling — all representing poor venous circulation that worsens throughout the day as blood pools in the dilated varicosities. Symptoms consistently worsen with prolonged standing or sitting and improve with leg elevation — the gravitational dependence of these symptoms distinguishes venous from arterial poor circulation.
Class 3 (Edema without skin changes): Leg swelling attributable to venous insufficiency — ankle and lower leg edema that is worse at the end of the day, pitting on pressure, and relieved by overnight elevation. The edema reflects chronic venous hypertension causing fluid transudation from the venous capillary bed into the interstitium.
Class 4 (Skin changes): Chronic venous hypertension produces skin changes in the lower leg: hyperpigmentation (brown discoloration from hemosiderin deposition as red blood cells extravasate into the tissue), lipodermatosclerosis (fibrosis and thickening of the subcutaneous fat from chronic inflammatory response), eczematous dermatitis (varicose eczema — itchy, inflamed skin over varicose veins or the ankle region), and atrophie blanche (white, stellate scarring patches). These changes indicate significant venous disease requiring active management.
Classes 5 and 6 (Healed and active venous ulcer): The most severe venous poor circulation manifestation — medial ankle ulcers from chronic venous hypertension impairing tissue oxygenation. Venous ulcers are the most common type of chronic lower limb ulcer (60 to 70 percent of all leg ulcers), have high recurrence rates (up to 70 percent within 3 years without sustained compression therapy), and cause significant quality-of-life impairment.
How Varicose Veins Differ from Arterial Poor Circulation
The critical clinical distinction is between venous poor circulation (varicose veins, chronic venous insufficiency) and arterial poor circulation (peripheral artery disease, PAD). These two conditions are sometimes confused because both cause leg symptoms — but they are mechanistically opposite, have very different risk factors, and require completely different treatments. Confusing them can be dangerous: compression therapy, which is the cornerstone of venous poor circulation treatment, can worsen arterial poor circulation by further impeding the already-insufficient arterial inflow.
Symptom pattern: Venous poor circulation symptoms — varicose vein aching, leg heaviness, ankle swelling — worsen with prolonged standing and are relieved by leg elevation (which drains the pooled venous blood). Arterial poor circulation symptoms — intermittent claudication (calf pain with walking), rest pain (foot pain at night) — are worsened by elevation (which reduces gravitational perfusion pressure) and relieved by dependency (hanging the leg down). This position-dependence difference is the most clinically reliable distinguishing feature at the bedside.
Skin appearance: Venous poor circulation produces warm, discolored (hyperpigmented), edematous skin with prominent varicose veins, often with a brawny, indurated texture from lipodermatosclerosis. Arterial poor circulation produces cool, pale or mottled skin with absent or diminished pulses, thin and shiny skin, loss of leg hair, and thick dystrophic toenails — reflecting chronic ischemia of the skin and its appendages.
Ulcer location and appearance: Venous ulcers occur above the medial malleolus (inner ankle) — the area of highest venous pressure from perforating vein incompetence — and have a shallow, granulating, wet bed with exudate and surrounding hyperpigmentation. Arterial (ischemic) ulcers occur at pressure points, the tips of toes, or distal foot locations, and have a pale or necrotic base, minimal exudate, and are surrounded by pale, ischemic skin.
Risk factors: Venous poor circulation risk factors include female sex, pregnancy, prolonged standing, obesity, family history of varicose veins, and prior DVT. Arterial poor circulation risk factors are the atherosclerosis risk factors: smoking, diabetes, hypertension, high cholesterol, and advanced age — the same risk factors that drive coronary artery disease and stroke.
The ankle-brachial index (ABI) provides the definitive test to distinguish the two: ABI below 0.9 confirms peripheral artery disease (arterial poor circulation); ABI of 1.0 to 1.3 is normal and supports venous insufficiency as the diagnosis in a patient with leg symptoms. Duplex ultrasound of the venous system (evaluating for venous reflux) and arterial system (measuring ABI) can both be performed in a single non-invasive evaluation session.
See our related articles on poor circulation in the legs, peripheral artery disease symptoms, deep vein thrombosis symptoms and prevention, blood clots warning signs and risk factors, and stroke prevention for adults for more detail on the overlapping vascular conditions that can affect leg circulation.
Diagnosing Varicose Veins and Chronic Venous Insufficiency
The evaluation of varicose veins and venous poor circulation begins with clinical assessment and is confirmed with duplex ultrasound:
Clinical assessment: History (symptom character, exacerbating and relieving factors, duration, prior DVT, family history, occupational standing exposure) and physical examination (standing examination of the legs to visualize varicose vein distribution, palpation of varicosities and tenderness, assessment of edema and skin changes, palpation of foot pulses to exclude concurrent arterial disease). The CEAP classification (Clinical-Etiologic-Anatomic-Pathophysiologic) standardizes venous disease severity from C0 (no visible venous disease) to C6 (active venous ulcer) — guiding treatment planning and enabling comparison across clinical studies.
Duplex ultrasound of the venous system is the essential diagnostic test — it identifies: which veins are incompetent (great saphenous, small saphenous, perforating veins, deep veins); the extent and duration of reflux (greater than 0.5 seconds after release of calf compression or Valsalva confirms pathological reflux); the diameter and depth of the incompetent saphenous trunk (determining endovenous ablation feasibility); and the status of the deep venous system (patent vs. prior thrombosis causing secondary venous disease). Duplex ultrasound is performed in the standing or reverse Trendelenburg position (to maximize hydrostatic load and demonstrate reflux) and maps the entire superficial and deep venous system of both legs.
ABI measurement should be obtained in all patients with leg symptoms to exclude concurrent peripheral artery disease — particularly before prescribing compression therapy. An ABI below 0.8 is a relative contraindication and below 0.5 is an absolute contraindication to full-compression stockings, as compression can reduce arterial inflow in a leg with marginal arterial perfusion.
Treatment Options for Varicose Veins and Venous Poor Circulation
Treatment is stratified by disease severity and directed at eliminating the incompetent venous segments responsible for the reflux:
Compression therapy — graduated compression stockings (20 to 30 mmHg or 30 to 40 mmHg) — is the foundational conservative treatment for varicose veins and chronic venous insufficiency. Compression counteracts venous hypertension by squeezing the dilated superficial veins, improving venous return velocity, reducing edema, and slowing disease progression. It is the treatment of choice for venous ulcer healing (high-compression therapy — multilayer compression bandaging) and is required after procedural varicose vein treatment to maintain results. Most insurance plans require a trial of compression therapy (typically 3 months) before approving procedural intervention.
Endovenous thermal ablation (EVTA) — radiofrequency ablation (RFA, ClosureFast procedure) or endovenous laser ablation (EVLA) — is the current standard of care for incompetent great saphenous or small saphenous veins. A thin catheter is inserted into the incompetent saphenous vein trunk under ultrasound guidance; thermal energy (radiofrequency or laser) heats and destroys the vein wall, causing permanent closure of the incompetent segment. EVTA is performed under local tumescent anesthesia as an office procedure (no general anesthesia or hospital admission required), with the patient walking immediately post-procedure. Clinical success rates exceed 90 to 95 percent at 5 years. EVTA eliminates the high-pressure reflux source that drives varicose vein formation, allowing residual varicosities to shrink or to be treated with subsequent phlebectomy or sclerotherapy.
Foam sclerotherapy involves injection of a sclerosant chemical (polidocanol or sodium tetradecyl sulfate) in foam form directly into varicose veins or perforating veins, causing chemical endothelial destruction and subsequent fibrosis and obliteration of the treated vein. Foam sclerotherapy is particularly useful for treating residual varicose tributaries after saphenous ablation, for recurrent varicosities, and for veins that are not suitable for thermal ablation (small, tortuous, or superficially located). Ultrasound-guided foam sclerotherapy allows treatment of veins not visible at the surface.
Ambulatory phlebectomy (microphlebectomy) is a minimally invasive office procedure in which varicose vein tributaries are removed through tiny (1 to 2 mm) stab incisions under local anesthesia. It is typically performed after saphenous vein ablation to remove the now-disconnected varicose tributaries, producing excellent cosmetic results. Wounds are small enough not to require sutures and heal with minimal scarring.
The Society for Vascular Surgery varicose veins patient resource covers treatment options and when to see a vascular surgeon. The NHLBI varicose veins guide explains causes, symptoms, diagnosis, and treatment. The American Academy of Dermatology varicose veins overview covers the skin manifestations of venous insufficiency and cosmetic treatment options.
- Gloviczki P, et al. The Care of Patients with Varicose Veins and Associated Chronic Venous Diseases: Clinical Practice Guidelines. J Vasc Surg. 2011;53(5 Suppl):2S-48S.
- Wittens C, et al. Editor’s Choice — Management of Chronic Venous Disease. Eur J Vasc Endovasc Surg. 2015;49(6):678-737.
- Eberhardt RT, Raffetto JD. Chronic Venous Insufficiency. Circulation. 2014;130(4):333-346.
- van den Bos R, et al. Endovenous Therapies of Lower Extremity Varicosities. J Vasc Surg. 2009;49(1):230-239.
- Rabe E, et al. Epidemiology of Chronic Venous Disorders in Geographically Diverse Populations. Int Angiol. 2012;31(2):105-115.
Varicose Veins During Pregnancy — Why They Develop and What to Do
Pregnancy is one of the most common triggers for varicose vein development or worsening of pre-existing varicose veins, for several overlapping reasons: increased blood volume (plasma volume increases approximately 50 percent during pregnancy, increasing the venous load); progesterone-mediated relaxation of vein wall smooth muscle and valve ring tissue (reducing valve competence); the enlarging uterus compressing the inferior vena cava and pelvic veins (increasing outflow resistance and raising venous pressure throughout the lower extremities); and the gravitational effect of prolonged standing on a venous system already under elevated pressure. Varicose veins appearing during pregnancy are most common in the second and third trimesters, typically in the great saphenous distribution on the medial thigh and calf, and frequently in the vulvar and perineal distribution (vulvar varicosities).
The clinical management dilemma in pregnancy-associated varicose veins is that interventional treatment (endovenous ablation, sclerotherapy) is generally deferred until after delivery and breastfeeding cessation, because procedural risks and sclerosant systemic absorption are not fully characterized in pregnancy. Conservative treatment during pregnancy — graded compression stockings (20 to 30 mmHg), regular leg elevation, walking to activate the calf muscle pump, and avoiding prolonged standing — is the recommended management strategy. Many pregnancy-related varicose veins partially or completely resolve spontaneously in the months following delivery as venous volume and pressure normalize. However, each subsequent pregnancy typically causes further varicose vein progression, and women with multiple pregnancies have correspondingly higher prevalence and severity of varicose veins. For women with pre-existing significant varicose veins planning additional pregnancies, the decision about timing of treatment (treat before next pregnancy vs. defer) should be individualized based on symptom severity and desire for additional children.
Spider Veins vs Varicose Veins — Understanding the Full Spectrum
Spider veins (telangiectasias) are frequently confused with varicose veins — both are visibly dilated superficial vessels on the legs, but they differ in size, depth, clinical significance, and treatment. Spider veins are tiny (below 1 mm), intradermal vessels visible as fine red, purple, or blue lines in sunburst, starburst, or linear patterns — typically on the outer thigh, inner knee, and ankle. They are fed by reticular veins (1 to 3 mm, blue-green feeding vessels just below the skin surface) that are not usually visible but are identifiable on examination as firm linear cords beneath the skin.
Spider veins are primarily cosmetic in most patients — causing concern about appearance rather than significant hemodynamic impairment or symptoms. However, in some patients they are associated with underlying incompetent saphenous or perforating veins — particularly when multiple spider vein clusters appear in characteristic distributions (inner ankle, outer thigh, or medial knee), which can indicate insufficiency in the underlying deep or saphenous system driving the superficial telangiectasias. In these cases, treating the underlying reflux source (duplex-guided foam sclerotherapy of the feeding reticular vein or saphenous ablation) before treating the spider veins improves cosmetic outcomes and reduces recurrence. Treating spider veins in isolation when there is a significant underlying reflux source typically results in rapid recurrence.
Treatment for spider veins is typically sclerotherapy (injection of a sclerosant solution directly into the telangiectasias with a very fine needle — 30 or 33 gauge) or laser/intense pulsed light (IPL) treatment (for very fine telangiectasias less than 0.3 mm that are too small for reliable needle injection). Multiple treatment sessions are typically required for complete cosmetic clearance. Results are cosmetic only — spider vein treatment does not affect venous hemodynamics or prevent further varicose vein development in patients with underlying venous insufficiency.
When Varicose Veins Require Urgent Evaluation
While varicose veins are usually a gradual, slowly progressive condition, several presentations require prompt medical evaluation:
Superficial thrombophlebitis: Acute onset of pain, redness, warmth, and a firm, tender cord along the course of a varicose vein indicates superficial thrombophlebitis — clot formation within a varicose vein. Though classified as “superficial” (distinguishing it from deep vein thrombosis), superficial thrombophlebitis of large varicose veins extending to within 3 to 4 cm of the saphenofemoral junction (where the great saphenous vein meets the deep femoral vein) carries significant risk of thrombus extension into the deep venous system — transforming into a proximal DVT with pulmonary embolism potential. All cases of superficial thrombophlebitis in large varicose veins should have duplex ultrasound performed to assess proximity to the saphenofemoral junction and exclude concurrent DVT; cases at or near the junction require anticoagulation.
Bleeding from varicose veins: Varicose veins at the ankle (where venous pressure is highest and skin is thinnest from chronic venous disease changes) can spontaneously rupture or bleed profusely from minor trauma. Variceal bleeding from the ankle is typically dramatic in volume (bright red venous blood pooling rapidly) but is easily controlled by firm direct pressure and leg elevation. Persistent, recurrent, or uncontrolled bleeding from varicose veins is an indication for expedited treatment of the underlying venous disease.
Non-healing leg ulcer: Any ulcer on the lower leg, particularly around the ankle, that does not show progressive healing within 4 weeks of standard wound care requires prompt evaluation by a vascular surgeon or wound care specialist. Venous ulcers require high-compression therapy (typically multilayer compression bandaging), wound care, and often underlying venous reflux treatment to achieve healing and prevent recurrence.