Prostate cancer is frequently called a “silent disease” — and that label is accurate for most men who have it. The majority of prostate cancers, particularly those caught through routine PSA screening, produce no symptoms at all at the time of diagnosis. This is precisely why screening exists: to find cancers before symptoms develop, when treatment is most likely to succeed.
When prostate cancer does produce symptoms, it usually means one of two things: either the tumor has grown large enough to press on the urethra and disrupt urinary flow, or the cancer has spread beyond the prostate to other parts of the body. Understanding which symptoms suggest which scenario — and how urgently each warrants attention — is the practical goal of this article.
Why Early Prostate Cancer Has No Symptoms
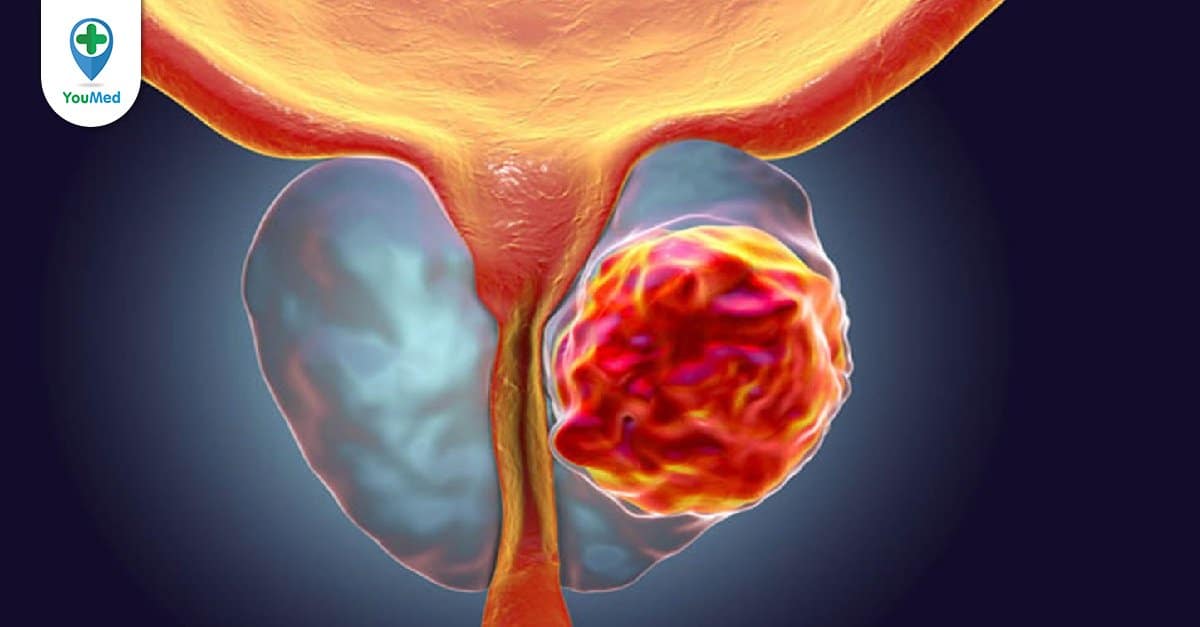
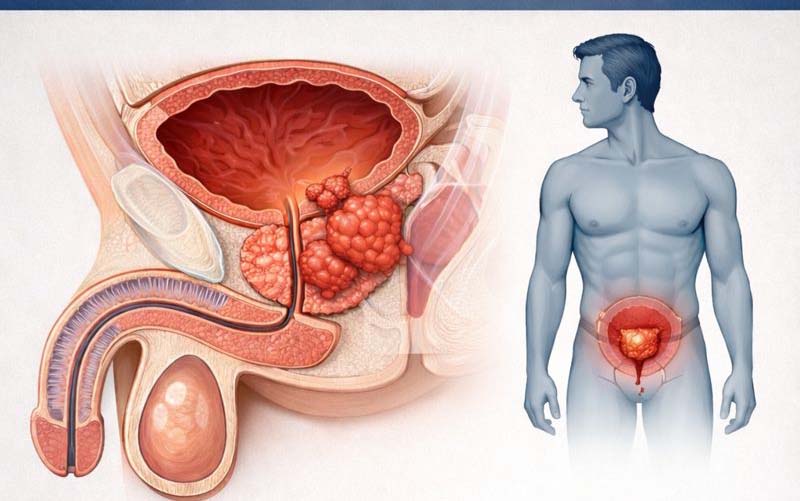
To understand why prostate cancer is so often asymptomatic at early stages, it helps to understand the anatomy. The prostate gland surrounds the urethra at the base of the bladder. Prostate cancers most commonly arise in the peripheral zone — the outer portion of the gland, away from the urethra. A tumor growing outward in the peripheral zone can reach significant size without ever pressing on the urinary channel.
By contrast, benign prostatic hyperplasia (BPH) — the non-cancerous enlargement that affects nearly every man after age 50 — grows from the transition zone, the inner portion immediately surrounding the urethra. This is why BPH produces prominent urinary symptoms at relatively small sizes, while prostate cancer often does not.
The practical implication is important: a man with significant urinary symptoms is more likely to have BPH than prostate cancer. Conversely, the absence of urinary symptoms does not reassure against prostate cancer. The only reliable way to detect prostate cancer before it produces symptoms is through PSA testing — which is why screening discussions matter.
Urinary Symptoms That Can Occur
When prostate cancer grows large enough or has spread to affect the urethra or bladder, it can produce urinary symptoms that overlap substantially with BPH. These include:
- Weak or slow urinary stream: Feeling that urine flows slowly or with less force than usual; needing to strain to initiate or maintain flow
- Frequency: Needing to urinate more often than usual, especially at night (nocturia)
- Urgency: A sudden, strong need to urinate that is difficult to defer
- Hesitancy: Difficulty starting the urine stream, sometimes requiring waiting or straining
- Incomplete emptying: The feeling that the bladder has not fully emptied after urinating
- Intermittent stream: Flow that starts and stops rather than flowing continuously
- Dribbling: Leaking small amounts after urination ends
These symptoms are identical to those caused by BPH and cannot be used to distinguish one condition from the other. A man presenting with these symptoms to his physician will typically be evaluated for both. Blood in the urine (hematuria) or blood in the semen (hematospermia) can also occur, and while both have many benign causes, they warrant medical evaluation to rule out prostate cancer and other urological conditions.
Urinary Symptoms: Prostate Cancer vs. BPH vs. Other Causes
The overlap between prostate cancer urinary symptoms and those of other common urological conditions is so significant that symptoms alone cannot guide diagnosis. Understanding the differential is helpful for contextualizing a new symptom:
Benign prostatic hyperplasia (BPH) is by far the most common cause of lower urinary tract symptoms in men over 50. It is not cancer and does not become cancer. The symptoms it produces are caused by the enlarged prostate compressing the urethra from the inside. BPH affects the majority of men in their 60s and 70s, and its prevalence increases with each decade.
Overactive bladder (OAB) produces urgency and frequency without an enlarged prostate. It is a bladder muscle condition, not a prostate condition, and can affect men and women alike.
Urinary tract infection (UTI) in men produces urgency, frequency, and often burning with urination. Men have shorter UTI episodes than women, and UTIs in men often signal an underlying problem (BPH, prostate infection, kidney stone) and warrant workup.
Prostatitis — inflammation of the prostate — can produce significant pelvic pain, urinary symptoms, and sometimes systemic illness. Acute bacterial prostatitis is a medical urgency with fever, chills, and severe perineal pain. Chronic prostatitis/chronic pelvic pain syndrome is more indolent and produces chronic pelvic pain, urinary symptoms, and sometimes sexual dysfunction.
A physician evaluating a man with new urinary symptoms will use a combination of history, physical examination (including digital rectal exam), urine analysis, PSA testing, and sometimes imaging or urodynamics to identify the cause.
Sexual Symptoms
Prostate cancer and its treatment can affect sexual function in several ways, though the cancer itself causes sexual symptoms less commonly than BPH or prostatitis.
Erectile dysfunction (ED): While ED is common in men over 50 for many reasons — cardiovascular disease, diabetes, medications, psychological factors — prostate cancer invading the neurovascular bundles adjacent to the prostate can cause erectile dysfunction. This is more likely with locally advanced cancer that has extended beyond the prostate capsule. For most men diagnosed with low-to-intermediate risk prostate cancer, erectile function at the time of diagnosis is not significantly different from age-matched peers without cancer.
Blood in semen (hematospermia): This is alarming to most men but is most commonly benign — caused by prostatitis, seminal vesicle inflammation, or minor bleeding from the prostate. In men over 40 with persistent hematospermia, prostate cancer is in the differential and warrants evaluation including PSA testing. Isolated hematospermia without other symptoms rarely indicates cancer.
Decreased semen volume: Locally advanced prostate cancer involving the seminal vesicles can reduce ejaculate volume. This is a late sign in most cases and indicates locally advanced disease.
Painful ejaculation: More commonly associated with prostatitis, but can occur with prostate cancer invading adjacent structures.
Symptoms of Advanced and Metastatic Prostate Cancer
When prostate cancer spreads beyond the prostate — which is less common in the PSA screening era but still occurs — the symptoms it produces depend on where it spreads. Prostate cancer has a strong predilection for the bones and lymph nodes.
Bone pain: The most common site of prostate cancer metastasis is bone, particularly the axial skeleton — spine, pelvis, ribs, and skull. Bone metastases produce deep, persistent aching that is different in character from musculoskeletal pain: it is often constant, present at rest and at night, and does not follow the mechanical pattern of back pain that worsens with activity and improves with rest. Spine involvement is the most common and produces mid-back or lower back pain; hip and pelvic involvement produces deep hip pain or groin pain. New, persistent bone pain in a man over 50 warrants medical evaluation.
Lower extremity swelling: Lymph node metastases in the pelvis can obstruct lymphatic drainage, causing bilateral leg swelling. Vascular compression by bulky pelvic lymph nodes can also contribute to lower extremity edema.
Weight loss and fatigue: Unintentional weight loss, persistent fatigue, and loss of appetite are nonspecific signs of advanced cancer that can occur with metastatic prostate cancer. These systemic symptoms indicate that the cancer is sufficiently advanced to produce metabolic effects.
Urinary obstruction in advanced disease: Locally advanced prostate cancer can invade the bladder or completely obstruct the urethra, leading to urinary retention — the inability to urinate at all. This is a urological emergency requiring immediate catheterization and evaluation.
Epidural spinal cord compression is the most serious acute complication of metastatic prostate cancer. When cancer in the vertebrae compresses the spinal cord, it causes rapidly progressive back pain, leg weakness, numbness, and eventually loss of bowel or bladder control. This is a neurological emergency. If you experience sudden severe back pain combined with leg weakness, numbness, or loss of bladder or bowel control, go to the emergency department immediately — irreversible paralysis can occur within hours if compression is not relieved.
When to See a Doctor
Different symptoms warrant different levels of urgency. Here is a practical framework:
Emergency (go immediately or call 911):
- Back pain with leg weakness, numbness, or loss of bladder/bowel control — possible spinal cord compression
- Complete inability to urinate despite strong urge — urinary retention
- Fever with severe pelvic pain and difficulty urinating — possible acute bacterial prostatitis
Urgent (call your doctor today or go to urgent care):
- Blood in urine, especially if visible and painless
- Sudden severe pelvic or perineal pain
- New severe bone pain — especially in the spine, pelvis, or hips
Non-urgent (schedule a routine appointment):
- Progressive worsening of urinary symptoms over weeks to months
- Frequent nighttime urination (nocturia) affecting sleep quality
- Erectile dysfunction with no obvious cause
- Blood in semen on more than one occasion
- Any of the above if you are over 50 and have not had a recent PSA test
What to Expect at Your First Appointment
When you see a physician for urinary or other prostate-related symptoms, the initial evaluation typically includes:
History: How long have symptoms been present? Are they progressively worsening? Any blood in urine or semen? Any family history of prostate cancer? Any bone pain? Prior PSA levels if known.
International Prostate Symptom Score (IPSS): A standardized seven-question questionnaire that quantifies urinary symptom severity on a 0–35 scale. Scores guide whether symptoms are mild (0–7), moderate (8–19), or severe (20–35) and help track changes over time.
Physical examination: Abdominal exam for bladder fullness or masses. Digital rectal exam (DRE) to assess prostate size, symmetry, and texture. Nodules, induration, or asymmetry on DRE raise concern for cancer and trigger further evaluation regardless of PSA level.
Laboratory tests: Urine analysis to check for infection, blood, or protein. PSA blood test if not recently checked. Creatinine if there is concern for urinary obstruction affecting the kidneys.
Imaging: Not always required at initial evaluation, but may include renal and bladder ultrasound to assess for hydronephrosis (kidney backup) or post-void residual volume to evaluate bladder emptying.
Symptoms That Are NOT Specific to Prostate Cancer
It is worth being clear about what does NOT signal prostate cancer specifically:
- Difficulty urinating in a man over 60 is far more likely to be BPH than cancer. BPH affects 70–80% of men in their 70s; prostate cancer causing symptoms is much less common.
- Urinary urgency and frequency are classic BPH and overactive bladder symptoms, not prostate cancer-specific signs.
- Erectile dysfunction has many causes — cardiovascular disease, diabetes, medication side effects, and age — and is not a specific sign of prostate cancer.
- Pelvic or perineal discomfort is most often associated with prostatitis (prostate inflammation), not cancer.
- A single episode of blood in semen is almost always benign in men under 40 and most cases in older men are also benign.
The key takeaway: no symptom uniquely identifies prostate cancer. Symptoms prompt evaluation, which includes PSA testing. The PSA test — not symptoms — is the clinical tool that triggers the diagnostic pathway for most prostate cancers diagnosed today. Understanding the full picture of who is at risk for prostate cancer helps determine how urgently any symptom warrants a physician visit.
Frequently Asked Questions
Can prostate cancer cause back pain?
Yes — but only in advanced disease. Metastatic prostate cancer that has spread to the spine and pelvis is a major cause of back pain in men with known prostate cancer. However, back pain in a man without a prior prostate cancer diagnosis is overwhelmingly more likely to be musculoskeletal in origin. Red flags that distinguish cancer-related bone pain from ordinary back pain include: constant pain present at night and at rest (not relieved by changing position), mid-thoracic or upper lumbar location (not the typical lumbar pattern of mechanical back pain), associated weight loss or fatigue, and age over 60 with no prior PSA screening. If these red flags are present alongside new persistent back pain, a physician evaluation that includes a PSA test is appropriate.
Does prostate cancer cause pain when urinating?
Burning or pain with urination (dysuria) is not a typical prostate cancer symptom. It is a hallmark of urinary tract infection and sometimes prostatitis. Prostate cancer, when it does produce urinary symptoms, typically causes obstruction-type symptoms — weak stream, hesitancy, frequency, incomplete emptying — rather than pain with urination. A man with painful urination should be evaluated for infection before attributing the symptom to prostate cancer.
At what stage does prostate cancer cause symptoms?
Most prostate cancers detected through PSA screening today are Stage I or II — confined to the prostate and producing no symptoms. Urinary symptoms most commonly appear when cancer has grown locally within or adjacent to the prostate (Stage III). Bone pain, weight loss, fatigue, and lower extremity swelling indicate Stage IV metastatic disease. The entire point of PSA-based prostate cancer screening is to detect cancer at Stage I or II, when it is still curable, rather than waiting for symptoms that indicate more advanced disease.
Can prostate cancer symptoms appear suddenly?
Onset of prostate cancer symptoms is usually gradual. The exception is spinal cord compression — which can progress rapidly from mild back pain to severe neurological deficits within hours to days — and acute urinary retention, which can occur suddenly when an advanced tumor completely obstructs the urethra. For most men, symptoms — if they occur at all — worsen progressively over months to years. Sudden onset of severe back pain with any neurological symptoms requires emergency evaluation.
Sources
- American Cancer Society. Prostate Cancer Signs and Symptoms 2023.
- National Comprehensive Cancer Network. Prostate Cancer v1.2024.
- Bubendorf L et al. Metastatic patterns of prostate cancer at autopsy. Hum Pathol 2000.
- Loblaw DA et al. Malignant extradural spinal cord compression in cancer. J Clin Oncol 2007.
- American Urological Association. Early Detection of Prostate Cancer Guideline 2023.
How Prostate Cancer Is Staged — and Why Symptoms Matter
Staging describes how far prostate cancer has spread at the time of diagnosis. The stage at diagnosis directly determines treatment options and prognosis, which is why the presence or absence of symptoms carries important clinical meaning.
Stage I and II (localized): Cancer is confined to the prostate. No symptoms. PSA may be mildly to moderately elevated. This is the stage at which prostate cancer is typically detected through PSA screening and is most likely to be curable with surgery or radiation. The vast majority of prostate cancers diagnosed in the United States today are at this stage — a direct consequence of widespread PSA-based prostate cancer screening.
Stage III (locally advanced): Cancer has extended beyond the prostate capsule to adjacent structures — seminal vesicles, bladder neck, or pelvic wall. May produce urinary symptoms if the bladder outlet is involved. Still potentially curable in many cases, but less reliably so than localized disease. Urinary symptoms in a man who has not had prior PSA screening may represent Stage III disease.
Stage IV (metastatic): Cancer has spread to regional lymph nodes (Stage IVA) or to distant organs, most commonly bone (Stage IVB). Produces the systemic symptoms described earlier — bone pain, lower extremity swelling, weight loss, fatigue. Treatment at this stage is systemic (androgen deprivation, chemotherapy, novel hormone agents) rather than local. Stage IVB disease is treatable but generally not curable with current therapies, though many men live for years with well-controlled metastatic disease.
The lesson in staging for a man experiencing symptoms is direct: if you are experiencing urinary obstruction, bone pain, or systemic symptoms that might indicate prostate cancer, early evaluation matters. The sooner locally advanced disease is identified, the more treatment options remain available.
The Role of the Digital Rectal Exam
The digital rectal exam (DRE) — a physical examination in which the physician inserts a gloved, lubricated finger through the rectum to feel the posterior surface of the prostate — has a meaningful role in prostate cancer detection that complements the PSA test.
A normal prostate on DRE is smooth, symmetrical, and approximately walnut-sized with a clearly defined central groove. Findings on DRE that raise concern for prostate cancer include:
- A hard nodule or area of induration (firmness) within the prostate
- Asymmetry between the two lobes of the prostate
- Loss of the central sulcus (the groove between the lobes)
- Extension of the hard area beyond the prostate capsule
A suspicious DRE is an indication for further evaluation regardless of PSA level — because prostate cancer arising in the peripheral zone can be palpable on DRE before it significantly elevates PSA. Men with a normal PSA but an abnormal DRE should be referred to urology for evaluation including imaging and potentially biopsy.
Many men are reluctant to undergo DRE, but the exam takes approximately 30 seconds, causes brief discomfort rather than pain, and provides clinical information that the PSA test alone cannot. For men over 50 discussing prostate cancer evaluation with their physician, combining a PSA test with a DRE provides a more complete screening picture than either test alone.
Should I See My Primary Care Doctor or a Urologist About Possible Prostate Cancer Symptoms?
For most men, the right first step is a primary care physician (PCP) or internist — not immediate referral to a urologist. Your PCP can perform an initial evaluation including history, physical examination, urinalysis, and PSA testing. If the PSA is elevated, DRE is abnormal, or urinary symptoms are severe and progressive, your PCP will refer you to a urologist for further evaluation.
Men with symptoms that suggest advanced prostate cancer — persistent bone pain, unexplained weight loss, significant fatigue, or lower extremity swelling without another explanation — and who are over 60 and have not had recent PSA testing should ask their PCP to order a PSA and consider whether urology referral is appropriate at the same visit.
Men who have already been diagnosed with prostate cancer and develop new symptoms — especially new bone pain, back pain with neurological features, or urinary obstruction — should contact their oncologist or urologist rather than waiting for a scheduled appointment. New symptoms in a man with known prostate cancer may indicate disease progression and warrant prompt reassessment. For context on what risk factors might have contributed to a diagnosis, our guide to prostate cancer risk factors covers the full picture from genetics to lifestyle.
Prostate cancer, when caught at the localized stage before symptoms develop, is one of the most treatable cancers in medicine. The priority is not to memorize a symptom checklist — it is to stay engaged with routine health care, know your risk profile, and have the PSA conversation with your physician at the appropriate age for your risk level.