
What Are the ABCDE Melanoma Warning Signs?
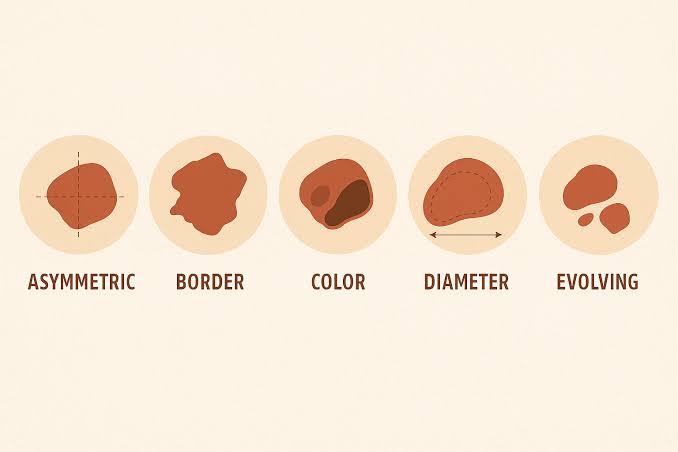
The ABCDE melanoma criteria are the most widely used and validated clinical framework for identifying early melanoma — both by physicians during professional skin examination and by patients during monthly self-examination. Each letter represents a specific visual feature that distinguishes melanoma from benign pigmented moles. Knowing how to apply these criteria is one of the most impactful things a person can do for their own skin cancer prevention.
The framework was first described in 1985 by Friedman, Rigel, and Kopf in the Journal of the American Academy of Dermatology, initially as the ABCD criteria. The fifth criterion — E for Evolution — was added by Rigel DS et al. in 2005 after research demonstrated that change over time was the most sensitive single indicator of melanoma. Together, the five ABCDE criteria form a practical checklist that guides both professional evaluation and monthly self-examination. For a comprehensive overview of the disease itself, see our guide to melanoma.
A — Asymmetry
A normal, benign mole (common melanocytic nevus) is symmetric — if you draw an imaginary line through its center in any direction, the two halves are mirror images of each other. Melanoma, by contrast, grows at variable rates in different directions because the malignant melanocytes within it proliferate unevenly. The result is a lesion where one half does not match the other.
To assess asymmetry, mentally divide the lesion through the center both horizontally and vertically. If either division reveals that the halves do not match — in shape, color distribution, or raised areas — the lesion is asymmetric. Any lesion that is asymmetric when divided in any plane warrants dermatological evaluation.
Important caveat: Asymmetry alone has moderate specificity — some benign lesions are mildly asymmetric, and early melanomas may appear nearly symmetric. Asymmetry should be interpreted alongside the other ABCDE criteria, and any doubt about whether a lesion is asymmetric is sufficient reason for evaluation.
B — Border
The border of a benign mole is smooth, well-defined, and sharply demarcated from the surrounding normal skin — there is a clear edge where the mole ends and normal skin begins. Melanoma borders are irregular. They may be:
- Notched — indentations along the border
- Scalloped — a wavy, scallop-shell-like perimeter
- Ragged or jagged — irregular projections into surrounding skin
- Indistinct or poorly defined — fading gradually into surrounding skin without a clear edge
- Satellite pigmentation — small isolated pigmented areas separate from the main lesion
The irregular border of melanoma reflects the chaotic, asymmetric growth pattern of malignant cells extending into surrounding tissue. Lentigo maligna melanoma — the type that develops on the face of older adults — characteristically has a particularly indistinct, gradually fading border that makes it easy to underestimate its true extent.
C — Color
A normal benign mole is a single, uniform color — one shade of tan, brown, or occasionally dark brown distributed evenly throughout the lesion. Melanoma characteristically displays multiple colors within a single lesion, reflecting the biological heterogeneity of malignant melanocytes at different stages of activity, regression, and inflammation.
The colors that can appear within a melanoma and what each represents:
- Dark brown or black: Dense melanin from highly active malignant melanocytes; often the first color to appear
- Tan or light brown: Less active tumor areas; early superficial spreading phase
- Red: Inflammation, neovascularization (new blood vessel formation feeding the tumor), or superficial ulceration
- White: Regression — areas where the immune system has partially destroyed melanocytes, replacing them with fibrous scar tissue; white areas within a dark lesion are particularly concerning
- Blue-gray: Deep dermal melanin (Tyndall effect) — melanin at depth scatters light, producing a blue-gray appearance rather than brown; common in invasive melanoma
- Pink or flesh-colored: Amelanotic areas; melanocytes that have lost the ability to produce melanin; can make lesions appear less threatening than they are
Any lesion with two or more distinct colors — particularly if the combination includes red, white, or blue-gray alongside brown or black — warrants evaluation. Three or more colors within a single lesion significantly raises the probability of melanoma.
D — Diameter
Most melanomas are larger than 6mm — approximately the diameter of a pencil eraser — when first diagnosed. This criterion was included in the original 1985 framework because it correlates with the size at which most melanomas present when detected by standard examination practices of the era.
However, Diameter is the least specific and least sensitive of the ABCDE criteria:
- Many melanomas are smaller than 6mm when diagnosed — particularly early nodular melanoma, lentigo maligna (early in situ stage), and acral lentiginous melanoma
- Many benign lesions (seborrheic keratoses, compound nevi, dermatofibromas) are larger than 6mm
- The 6mm threshold should never be used to provide false reassurance. “This mole is less than 6mm so I am not worried” is a potentially dangerous clinical conclusion — particularly in the presence of other ABCDE features or evolution.
Diameter is most useful as a supplementary criterion when combined with others. A rapidly growing lesion that has reached 6mm within months is far more concerning than a stable 8mm lesion that has been unchanged for 20 years.
E — Evolution
Evolution is the most sensitive of the five ABCDE criteria and the one that most frequently prompts patients to seek evaluation — because it is directly observable over time. Any change in a mole or skin lesion qualifies as evolution:
- Increase in size — even gradual growth over months
- Change in color — darkening, lightening, or development of new colors
- Change in shape — border irregularity that wasn’t present before
- Change in surface — elevation of a previously flat lesion; development of a nodule within a flat plaque
- New symptom — itching, tenderness, burning, or pain in a mole that was previously asymptomatic
- Spontaneous bleeding — bleeding without trauma or injury
- Crusting or scaling — surface breakdown
A mole that has been completely stable for 20 years and then begins to change should be evaluated urgently — not at the next annual appointment, but within days to weeks. Evolution overrides all other criteria in terms of clinical urgency. A new lesion that appeared within the past 6–12 months and was not present before also qualifies as evolution, even if it does not meet any of the other ABCDE criteria.
EFG Rule: Detecting Nodular Melanoma
The classic ABCDE criteria were developed primarily with superficial spreading melanoma in mind — the subtype with a recognizable radial growth phase and visible surface irregularities. Nodular melanoma, the second most common and most aggressive subtype, frequently does not display the ABCDE features because it begins with vertical growth immediately, is often uniformly dark or amelanotic (unpigmented), and may be small when it is already thick and dangerous.
The EFG rule — Elevated, Firm, Growing — was developed as a complementary framework specifically for recognizing nodular melanoma:
- Elevated: Raised above the skin surface; dome-shaped or nodular
- Firm: Firm to touch; not soft or compressible like a cyst or lipoma
- Growing: Visible growth over days to weeks; not stable
Any skin lesion — regardless of color or whether it meets ABCDE criteria — that is elevated, firm, and growing rapidly deserves urgent biopsy. Amelanotic (pink or flesh-colored) nodular melanoma is the most commonly delayed diagnosis in dermatology because it can resemble a pyogenic granuloma, hemangioma, or inflamed cyst. When in doubt, biopsy.
The Ugly Duckling Sign
The ugly duckling sign is a complementary melanoma detection tool that exploits the observation that in most individuals, all moles tend to resemble each other — they form a pattern, a “flock.” A melanoma frequently looks different from a patient’s other moles: it is the outlier, the lesion that doesn’t fit. This approach is particularly valuable in patients with many moles, where individual application of ABCDE criteria to each of dozens of lesions is impractical.
The concept was originally described by Grob JJ et al. (1998) and has been validated as an independent diagnostic approach with good sensitivity. In practice, patients can apply this concept during self-examination by asking: “Does any mole look different from all my other moles?” That lesion — the ugly duckling — deserves specific attention regardless of whether it meets individual ABCDE criteria.
How to Perform Monthly Skin Self-Examination Using ABCDE
Monthly skin self-examination is the practical application of the ABCDE framework at home. A systematic approach ensures no body surface is overlooked:
- Set up: Good lighting (natural daylight or bright lamp), a full-length mirror, a hand mirror, a blow-dryer or comb for the scalp, and a smartphone for photographing suspicious lesions.
- Face and neck: Examine all facial skin including the ears (inner and outer surfaces). Check the neck, including the back of the neck.
- Scalp: Part the hair systematically with a blow-dryer or comb. Ask a partner to examine the posterior scalp and crown.
- Hands and forearms: Inspect the backs of the hands, between the fingers, fingertips, and the skin around and under the fingernails. Look for dark longitudinal streaks under any nail.
- Upper body: Raise the arms and inspect the inner arms, armpits, chest, and upper abdomen. Check beneath the breasts.
- Back and buttocks: Use the hand mirror in front of the full-length mirror to inspect the entire back from shoulders to buttocks. The back is the most common melanoma site in men.
- Lower legs and feet: Sit and examine the front and back of both legs. Check the soles of the feet, between the toes, and all toenails.
- Genitalia: Inspect the genital and perianal region.
After completing the examination, apply the ABCDE framework mentally to each pigmented lesion noticed. The goal is not to diagnose — it is to identify any lesion that looks different from before or different from your other moles, then bring it to a dermatologist’s attention.
Documenting Moles with Photography
Monthly photography of your moles transforms the E (Evolution) criterion from a subjective impression into an objective measurement. A lesion that appears to be unchanged from memory alone is often documented to have grown or changed color when compared to a photograph taken 3 months earlier.
Practical photography tips for melanoma monitoring:
- Use consistent lighting — natural daylight without direct flash
- Photograph from the same distance and angle each month
- Include a ruler or coin in the frame for size reference
- Photograph the body location as well as a close-up of the lesion for anatomical reference
- Date each photograph and keep a dedicated folder organized by lesion
Dermatology practices increasingly use digital dermoscopy systems that provide professional-quality photographs with dermoscope magnification at each visit, generating automated side-by-side comparisons. For patients with many moles or a personal or family history of melanoma, this “total body photography” (TBP) approach substantially improves early melanoma detection. For guidance on whether TBP is indicated for your risk level, see our guide to skin cancer screening.
Dermoscopy: The ABCDE Framework Under Magnification
Dermoscopy — examination of a lesion using a hand-held device providing 10x polarized magnification — extends the ABCDE framework by revealing subepidermal structures not visible to the naked eye. Dermoscopy substantially improves melanoma diagnostic accuracy compared to naked-eye examination alone.
Dermoscopic features associated with melanoma include:
- Atypical pigment network (irregular meshwork pattern)
- Regression structures (white scar-like areas, blue-gray “peppering”)
- Blue-white veil (a confluent blue-white area over part of the lesion)
- Irregular streaks (pseudopods, radial streaming at the periphery)
- Irregular dots and globules distributed asymmetrically
- Atypical vascular patterns (irregular vessels, milky-red areas)
Dermoscopy also helps distinguish BCC (arborizing vessels, leaf-like pigment areas) from melanoma — reducing unnecessary biopsies of benign pigmented BCC. All dermatologists should perform dermoscopy on any suspicious pigmented lesion before deciding to observe or biopsy. For more on the full spectrum of melanoma symptoms including subtype-specific presentations, see our dedicated guide.
Do not wait for your annual skin check if you notice: Any mole or lesion that meets one or more ABCDE criteria; any mole that you are certain has changed since the last time you looked; a mole that bleeds, itches, or crusts spontaneously; a new raised, firm, growing skin nodule of any color; a dark streak under a fingernail or toenail that has appeared recently or is widening; or any lesion that simply looks different from all your other moles (ugly duckling). Annual professional skin examination catches lesions that are not yet causing concern; ABCDE-positive findings between annual visits require evaluation now, not later. For a full picture of the skin cancer symptoms across all types, see our comprehensive guide.
Frequently Asked Questions
Do all melanomas show all five ABCDE criteria?
No. No single criterion is both highly sensitive and highly specific. Most melanomas demonstrate 2–3 of the five criteria; some early melanomas may show only evolution. Nodular melanoma, in particular, may show none of the ABCDE features and is better evaluated using the EFG rule (Elevated, Firm, Growing). Any lesion that raises concern under any criterion — or that simply looks different from your other moles — deserves evaluation. Do not wait to accumulate all five criteria before seeking professional assessment.
Can a benign mole have some ABCDE features?
Yes. Some benign lesions — particularly compound nevi, blue nevi, and seborrheic keratoses — can exhibit features that partially resemble ABCDE criteria. Asymmetry and size can occur in benign lesions. This is why dermoscopy and physician evaluation are important: the ABCDE framework is a screening tool that guides who needs professional evaluation, not a diagnostic tool that patients can use to definitively rule melanoma in or out. When in doubt, see a dermatologist. For an understanding of what conditions can mimic melanoma, see our guide to melanoma symptoms.
Is the ABCDE rule useful for melanoma under the nails?
The ABCDE rule applies less directly to subungual (under-nail) melanoma, which presents as longitudinal melanonychia — a dark streak running the length of the nail. The relevant warning feature for subungual melanoma is Hutchinson’s sign: extension of the dark pigment from the nail bed onto the surrounding skin of the nail fold. Any new dark streak under a nail — particularly if widening, irregular in color, or accompanied by nail destruction — warrants urgent dermatological evaluation regardless of ABCDE criteria.
At what age should I start applying the ABCDE criteria?
There is no age minimum. Melanoma can occur at any age, including in adolescents and young adults. However, the absolute risk is highest in adults over 50, particularly those with significant UV exposure history or risk factors. Applying the ABCDE framework during monthly self-examination is appropriate from early adulthood onward. Any new mole that appears after age 40 — when new mole formation is otherwise uncommon — is particularly worth evaluating. For guidance on when to begin professional skin screening, see our guide to skin cancer screening.
Sources
- Rigel DS et al. ABCDE — an evolving concept in the early detection of melanoma. J Am Acad Dermatol. 2005.
- American Academy of Dermatology. Melanoma: Signs and Symptoms.
- National Cancer Institute. Melanoma Treatment (PDQ).
- Skin Cancer Foundation. Melanoma Warning Signs and Images.
- Friedman RJ, Rigel DS, Kopf AW. Early detection of malignant melanoma: the role of physician examination and self-examination of the skin. CA Cancer J Clin. 1985.
ABCDE Criteria in Context: When One Feature Is Enough
A common misconception about the ABCDE melanoma framework is that a lesion must satisfy multiple criteria before it warrants evaluation. This is incorrect and potentially dangerous. The five criteria are designed to be applied as independent indicators, not as a checklist requiring multiple checkmarks.
Consider the implications: a melanoma that displays only the E criterion (evolution — it is changing) but appears symmetric, has a regular border, is one color, and is under 6mm could easily be dismissed if a “need multiple criteria” mindset is applied. That same melanoma, if it is actively growing over a period of 6 weeks, has demonstrated the most sensitive indicator available and deserves prompt evaluation regardless of the other four criteria being negative.
Similarly, a new mole that appears in a 55-year-old who had never had that spot before meets the E criterion — it is a new lesion that represents a change from baseline — even if it otherwise looks perfectly benign. New moles in adults over 40, when most people are no longer forming new benign nevi, are a recognized melanoma risk signal.
The correct use of the ABCDE framework is: one or more criteria met = evaluation indicated. The more criteria that are met, the higher the clinical urgency — but a single criterion is sufficient justification for a dermatology visit.
Applying ABCDE to Specific Skin Locations
While the ABCDE criteria apply universally, specific anatomical locations present practical challenges that deserve mention:
Scalp: Melanoma on the scalp is frequently detected late because the lesion is covered by hair. When performing scalp self-examination, the goal is not comprehensive visualization of every square centimeter — it is identifying any area of scalp that feels rough, crusted, raised, or different when running fingers through the hair, which then warrants a closer look with a mirror or with a partner’s assistance.
Sole of the foot: Acral lentiginous melanoma on the plantar surface (sole) presents as an irregular, slowly darkening patch. Patients may attribute dark spots on the soles to bruising from shoes or trauma. Any persistent pigmented patch on the sole that has not faded within 4–6 weeks — the timeframe for resolution of a typical bruise — warrants evaluation.
Mucosa: Mucosal melanoma — inside the mouth, nasal cavity, or anogenital region — is not evaluated by the ABCDE criteria in the same way as skin lesions, but the general principle applies: any new or changing pigmented area on mucosal surfaces that is unexplained, persistent, or irregular in color or shape warrants evaluation. For a full overview of melanoma symptoms across all anatomical presentations, see our dedicated guide to melanoma symptoms.
Understanding the ABCDE melanoma framework thoroughly — knowing what each letter means, how to apply it during monthly self-examination, and when to act on findings — is one of the most effective evidence-based skin cancer prevention behaviors available to any individual. The biology of early melanoma is highly favorable; the same disease detected months or years later is dramatically less so. The ABCDE framework bridges that gap by putting recognition in the patient’s hands every month between annual professional skin examinations.