Getting a high PSA result is one of the most anxiety-inducing lab reports a man can receive. The phrase “elevated PSA” raises the immediate specter of prostate cancer — but the reality is that most elevated PSA results are not cancer. The PSA test is sensitive but not specific: it detects when something is happening in the prostate without telling you what that something is.
What matters most after a high PSA result is the pathway that follows — not panic, and not passivity. A structured approach rules out false positives first, uses additional tests to refine the cancer probability, and uses an MRI to decide whether biopsy is even necessary. That approach gets the right answer while protecting the majority of men with elevated PSA from biopsies they don’t need.
What “High PSA” Actually Means
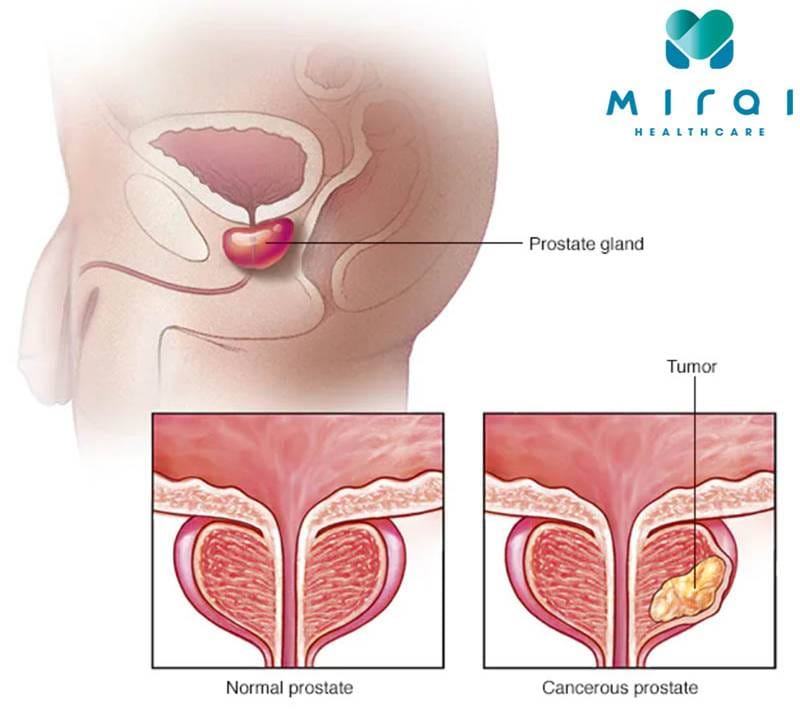
Prostate-specific antigen is produced by all prostate tissue — benign prostatic hyperplasia (BPH), prostatitis, and normal prostate cells all contribute to the serum PSA level. When PSA rises above the threshold used for your age, it means the prostate is more active than expected — not necessarily that cancer is present.
At a PSA of 4 ng/mL or above, the probability of finding cancer on biopsy is approximately 25 to 30 percent. This means roughly three out of four men with an elevated PSA at this threshold who undergo biopsy do not have prostate cancer. The most common explanation is BPH — an enlarged, highly active prostate that simply produces more PSA than a normal-sized gland.
“High” is also a relative term. A PSA of 3.5 ng/mL in a healthy 48-year-old is more concerning than a PSA of 5.5 ng/mL in a 75-year-old with a documented 80-gram prostate from BPH. Age-adjusted ranges, PSA density (PSA divided by prostate volume), and PSA trajectory over time all matter as much as the absolute number. Understanding what your result means in context is the first step toward an appropriate response.
PSA Velocity and PSA Density — Secondary Metrics That Matter
Beyond the raw PSA value, two derived metrics help interpret whether an elevated PSA represents ongoing, progressive activity or a stable baseline:
PSA velocity (PSAV) is the rate of change in PSA over time. A rise of more than 0.75 ng/mL per year when PSA is above 4 ng/mL is considered clinically significant, as is a rise of more than 0.35 ng/mL per year when PSA is between 2.5 and 4 ng/mL. The key caveat is that velocity requires at least two to three PSA measurements taken over a minimum of 12 to 18 months at the same laboratory using the same assay. A single jump from one lab to another, or from one assay platform to another, can create an apparent velocity that reflects assay differences rather than true biological change.
PSA density (PSAD) is the PSA level divided by prostate volume (measured by MRI or transrectal ultrasound). It corrects for the contribution of a large BPH prostate to total PSA. A PSA density below 0.10 ng/mL/cc is generally reassuring; above 0.15 ng/mL/cc increases clinical concern and lowers the threshold to proceed with biopsy. PSA density is particularly useful when a man with a large, clearly BPH-dominant prostate on MRI has a modestly elevated total PSA — a high volume explains much of the elevation and the adjusted density may be within normal limits.
These secondary metrics are not used in isolation. They add context to the raw PSA number and contribute to the shared decision-making process about whether and when to proceed to biopsy. If you want a deeper understanding of what how the PSA test works and what different forms of PSA measure, that background helps make sense of why PSA density and velocity carry clinical weight.
Before Worrying — Rule Out False Positives
The first step after receiving a high PSA result is not to call a urologist and schedule a biopsy. It is to determine whether the result is reliable.
Several common circumstances cause transient, false PSA elevation that disappears when the interfering factor resolves:
- Recent ejaculation (within 24–72 hours): mild but real effect; abstain for 48–72 hours before any repeat PSA draw
- Vigorous perineal activity (prolonged bicycling, horseback riding) within 24–48 hours: transiently elevates PSA
- Digital rectal exam (DRE) immediately before the blood draw: draw PSA before the DRE, or at least 2 days after
- Prostatitis or urinary tract infection: can dramatically elevate PSA to 10–20 ng/mL or higher; PSA normalizes with treatment; recheck 6 to 8 weeks after infection clears
- Prostate biopsy, TRUS, or urological instrumentation: causes significant elevation lasting 4 to 6 weeks; never draw PSA within this window
- Finasteride or dutasteride (5-alpha reductase inhibitors): these medications suppress PSA by approximately 50%; physicians must double the PSA value when a patient is on these drugs to estimate the true biological level
Additionally, a single elevated PSA that has never been seen before warrants confirmation with a second measurement at the same laboratory. PSA can vary 10 to 15 percent between tests due to normal biological variability and assay differences. Two consistent measurements at the same lab over several weeks are far more meaningful than a single reading.
Do NOT undergo prostate biopsy based on a single PSA result drawn under conditions that might have caused false elevation — recent infection, recent intercourse, cycling, or recent instrumentation. Confirm the result under controlled conditions first. A biopsy is an invasive procedure with real risks; it should only follow a reliably elevated PSA.
Next Steps After a Confirmed High PSA
Once a high PSA is confirmed as reliable and not attributable to a reversible cause, a structured evaluation follows. This pathway is outlined in the AUA Early Detection Guideline and is consistent with what you might encounter when your physician discusses prostate cancer screening options with you.
Adjunct Blood Tests
Several FDA-approved or validated biomarkers can be run from the same blood draw as total PSA to provide additional cancer risk information before committing to biopsy:
- % free PSA: The ratio of free (unbound) PSA to total PSA. A lower percentage is associated with higher cancer risk. Below 10%: approximately 56% probability of cancer on biopsy. Above 25%: approximately 8% probability. Most useful when total PSA falls in the 4 to 10 ng/mL gray zone.
- Prostate Health Index (PHI): Combines total PSA, free PSA, and [-2]proPSA (a precursor form disproportionately elevated in cancer). FDA approved for PSA 4 to 10 ng/mL. Superior to PSA or % free PSA alone for predicting clinically significant cancer.
- 4Kscore: Combines four kallikrein markers with clinical variables to directly estimate the probability that biopsy would find Grade Group 2 or higher cancer — the type that actually warrants treatment. Area under the ROC curve approximately 0.82, compared to about 0.63 for PSA alone.
Multiparametric MRI Before Biopsy
AUA, NCCN, and major international guidelines now recommend multiparametric MRI (mpMRI) before biopsy when feasible. MRI assigns a PI-RADS score from 1 (most likely benign) to 5 (most likely malignant) to any lesions identified:
- PI-RADS 1–2: Very low probability of clinically significant cancer. Biopsy can often be safely deferred; monitor PSA and consider repeat MRI or biopsy in 12–18 months if PSA continues to rise.
- PI-RADS 3: Intermediate. Clinical context, PSA density, and biomarker results determine whether to proceed to biopsy.
- PI-RADS 4–5: Biopsy is recommended. Fusion biopsy — combining MRI-targeted sampling with systematic cores — is preferable when a lesion is identified.
Biopsy (If Indicated)
Transperineal biopsy is now preferred over the traditional transrectal ultrasound (TRUS)-guided approach at centers where it is available. The transperineal route avoids passing the needle through the rectal wall, dramatically reducing infection risk including the risk of sepsis from rectal bacteria.
Fusion biopsy overlays the pre-procedure MRI image onto the real-time ultrasound during the procedure, guiding targeted sampling of suspicious zones identified by MRI while also collecting systematic cores from the rest of the prostate.
The biopsy pathology report will tell you: the number of cores positive for cancer, the percentage of each core involved, the Gleason grade, and the Grade Group — the number that matters most for deciding what happens next.
Understanding Your PSA Level
The appropriate clinical response to a high PSA depends partly on the absolute level:
PSA 4 to 10 ng/mL (“diagnostic gray zone”): The majority of elevated PSA results fall here. Cancer probability on biopsy is approximately 25 to 30 percent — meaning most men in this range have BPH, not cancer. Adjunct tests and MRI are most useful in this range to select who actually needs a biopsy and who can safely be monitored.
PSA 10 to 20 ng/mL: Cancer probability is higher; the additional value of biomarkers to avoid biopsy is somewhat lower. MRI remains important to characterize any lesion and guide biopsy technique. Cancer found at this PSA level is more likely to be Grade Group 2 or higher, and treatment is more often appropriate than surveillance.
PSA above 20 ng/mL: NCCN classifies this as high-risk disease. Biopsy is strongly indicated. If prostate cancer is confirmed, staging workup — bone scan and/or PSMA PET-CT — is performed to assess for metastatic disease before treatment planning.
PSA above 100 ng/mL: Strongly suggests locally advanced or metastatic disease. Staging imaging (PSMA PET-CT is now preferred over conventional bone scan and CT where available) is indicated even before biopsy confirms the diagnosis. Androgen deprivation therapy may be started while biopsy is being arranged.
If Your Biopsy Is Positive
The Grade Group assigned by pathology is the most important factor determining what happens next — more so than the PSA level itself.
Grade Group 1 (Gleason 6, 3+3): This is the lowest-risk prostate cancer and the one most commonly discovered after a PSA in the 4 to 10 ng/mL range. Active surveillance — monitoring the cancer rather than treating it immediately — is the standard of care for Grade Group 1 and is appropriate for most patients. The PROTECT trial, with 15 years of follow-up published in 2023, found no significant difference in prostate cancer mortality between active monitoring, radical prostatectomy, and radiation therapy for low-to-intermediate risk disease. Treating Grade Group 1 prostate cancer with surgery or radiation is a choice, not a clinical necessity, and carries real risks of incontinence and erectile dysfunction that should weigh heavily in the decision.
Grade Group 2 (Gleason 7, 3+4): Favorable intermediate risk. Active surveillance remains an option for carefully selected patients — specifically those without cribriform architecture on pathology, with fewer than 50% of biopsy cores positive, and no other adverse features. Many patients and physicians elect definitive treatment, which is also appropriate. This is a decision that deserves careful discussion about the surveillance versus treatment tradeoffs specific to the individual’s health, age, and values.
Grade Group 3 through 5 (Gleason 7 with 4+3, 8, 9–10): Unfavorable intermediate to very high risk. Active surveillance is not appropriate for these grades. Treatment with radical prostatectomy or radiation therapy — combined with androgen deprivation therapy for intermediate-high and high-risk disease — is the standard approach. Grade Group 4 and 5 cancers warrant prompt treatment after appropriate staging.
Active Surveillance — What Monitoring Actually Involves
For men with Grade Group 1 (and selected Grade Group 2) prostate cancer, active surveillance is not a passive decision to ignore cancer. It is a structured monitoring program with defined checkpoints:
- PSA every 3 to 6 months for the first 1 to 2 years, then every 6 to 12 months if stable
- Repeat biopsy within 12 to 24 months of initial diagnosis to confirm Grade Group classification (some Grade Group 1 cancers are reclassified to Grade Group 2 on a more thorough second biopsy)
- Annual or biannual MRI to monitor for lesion growth or new suspicious areas
- Repeat biopsy if PSA rises significantly or if MRI shows new suspicious findings
The goal is to detect reclassification to higher-grade disease early enough that curative treatment remains available. The UCSF, Johns Hopkins, and Toronto Sunnybrook cohort data all show that more than 80 percent of men on active surveillance for Grade Group 1 cancer remain under surveillance — without needing treatment — at 10 years.
The question of when to escalate from surveillance to treatment is one of the most nuanced decisions in prostate oncology, and it should involve a urologist and, ideally, a multidisciplinary team. Men concerned about being at elevated risk of finding themselves in this situation can review what early prostate cancer symptoms look like — or rather, don’t look like — since most early-stage disease is completely asymptomatic and found only through PSA screening.
If Your Biopsy Is Negative
A negative biopsy does not definitively exclude prostate cancer. The false-negative rate for a standard 12-core systematic biopsy is approximately 20 to 30 percent — roughly one in four to five men with a negative biopsy may have a cancer that was not sampled, particularly in the anterior prostate and apical regions that are systematically undersampled by the traditional posterior approach.
If your biopsy comes back negative:
- If MRI showed a suspicious lesion (PI-RADS 4–5) that was not adequately targeted during biopsy, a repeat fusion biopsy is appropriate
- If both MRI and biopsy were negative, continue PSA monitoring — typically every 6 to 12 months
- If PSA continues to rise after a negative biopsy, repeat biopsy in 1 to 3 years is appropriate
- PSMA PET-CT is increasingly used in men with persistently rising PSA after negative conventional biopsies; it can detect tumor foci missed by both conventional imaging and standard biopsy
Men who find themselves navigating persistently rising PSA after a negative biopsy often benefit from understanding the full landscape of prostate cancer risk factors — including genetic mutations like BRCA2 that may increase both risk of cancer and risk of aggressive disease even when early biopsies are negative.
Frequently Asked Questions
Can I have a high PSA and no cancer?
Yes — and in fact, this is the most common outcome when PSA is in the 4 to 10 ng/mL range. Benign prostatic hyperplasia is the most frequent explanation for modestly elevated PSA in men over 50. Prostatitis, urinary tract infection, and several medications and activities can also cause false elevation. Approximately 70 to 75 percent of men with PSA above 4 ng/mL who undergo biopsy do not have prostate cancer. This is the primary reason the evaluation pathway involves multiple steps before recommending biopsy — because most men with a high PSA result will not turn out to have the disease.
How quickly do I need to act on a high PSA result?
There is almost always time to think carefully. Prostate cancer — including most high-grade cancers — does not change clinically in the weeks it takes to repeat a PSA, obtain an MRI, or have a consultation with a urologist. The only situation requiring more urgent action is a very high PSA (above 100 ng/mL) with symptoms suggesting locally advanced or metastatic disease, where staging evaluation and treatment should proceed without unnecessary delay. For most men with PSA in the 4 to 20 ng/mL range, taking several weeks to gather information, seek a second opinion, or discuss options carefully does not affect outcomes.
What is the difference between a high PSA and a prostate cancer diagnosis?
A high PSA is a signal, not a diagnosis. Prostate cancer can only be diagnosed by biopsy with pathological review of prostate tissue. An elevated PSA prompts evaluation — repeat testing, adjunct biomarkers, MRI, and potentially biopsy — but none of those steps alone constitutes a diagnosis. Many men with persistently elevated PSA go through the full evaluation pathway and are ultimately found to have BPH, prostatitis, or no identifiable abnormality. If you are wondering whether your PSA level warrants concern, reviewing how prostate cancer screening guidelines frame the decision can help you and your physician have a more informed conversation.
Sources
- American Urological Association. Early Detection of Prostate Cancer Guideline 2023.
- National Comprehensive Cancer Network. Prostate Cancer v1.2024.
- Kasivisvanathan V et al. MRI-targeted or standard biopsy for prostate cancer diagnosis (PRECISION). NEJM 2018.
- Hamdy FC et al. Fifteen-year outcomes after monitoring, surgery, or radiotherapy for prostate cancer (PROTECT). NEJM 2023.
- Parekh DJ et al. The 4Kscore test reduces prostate biopsy rates. Eur Urol 2015.
Questions to Ask Your Urologist After a High PSA
Knowing what to ask during your urology appointment can help you leave with a clearer plan and less anxiety. These are the questions that move the conversation from a result to a decision:
- Was this PSA drawn under controlled conditions? Ask whether any activities in the days before the blood draw — DRE, ejaculation, cycling, recent prostate procedure — could have artificially elevated the result and whether a repeat test under controlled conditions is warranted.
- What is my PSA density? If you have had a prostate volume estimate (from MRI or ultrasound), ask for your PSA density. A high total PSA in the context of a large prostate may have a reassuringly low density.
- Should I have a repeat PSA before deciding on biopsy? A single elevated result that has never been seen before is less concerning than a persistently elevated trend. Ask whether confirmation is appropriate in your case.
- Do I need an MRI before biopsy? Guidelines now recommend MRI before biopsy when feasible. Ask whether this is available and appropriate for you. A negative MRI (PI-RADS 1–2) may allow biopsy to be safely deferred.
- Which adjunct test is most appropriate for me? % free PSA, PHI, and 4Kscore all add information but have different strengths depending on your total PSA level and clinical situation. Ask which test your urologist recommends and why.
- If biopsy finds Grade Group 1 cancer, what is the next step? Understanding that the most likely outcome of a positive biopsy in the 4–10 ng/mL PSA range is a low-grade cancer managed with active surveillance — not immediate surgery — can reduce pre-procedure anxiety significantly.
The goal of this conversation is shared decision-making. Your urologist should explain the tradeoffs of proceeding versus deferring biopsy, and you should feel informed enough to make a preference-sensitive decision. Men who want to understand the full landscape of factors that affect prostate cancer risk — including genetics, age, and race — will be better equipped to contextualize their PSA result in a broader risk picture.
Keeping a PSA Log
Because PSA trend matters as much as any single value, tracking your results over time is genuinely useful. A simple log — date, lab, PSA value, and clinical context (any activities, medications, or procedures that might have affected it) — gives your urologist the raw material to calculate velocity, assess trend, and identify whether any past spikes were artifactual.
Bring this log to every urology appointment. If you have had PSA tests through multiple providers or at multiple institutions, request copies of the actual values and dates rather than relying on memory or verbal recall. Many men have been told only that their PSA was “fine” or “a little high” without being given the actual number — and those numbers, in context and over time, are what matter for the clinical decision.