Troponin Test: What It Means for Your Heart
The troponin test is the most important blood test in emergency cardiac medicine ??? the gold standard biomarker for detecting acute myocardial infarction (heart attack) and the centerpiece of the rapid evaluation protocols used in emergency departments worldwide to determine, within hours, whether chest pain is caused by a heart attack. Understanding what the troponin test measures, why the pattern of results matters more than any single value, and what causes troponin to be elevated besides a heart attack helps patients and their families make sense of what can be an alarming and confusing test result.
Troponin is not a medication or a chemical the hospital injects ??? it is a protein your own heart muscle cells release when they are injured. Under normal conditions, troponin levels in the blood are extremely low (often below the detection limit of standard assays). When heart muscle cells die ??? from any cause ??? they rupture and release their contents, including troponin, into the blood. Modern high-sensitivity troponin assays can detect vanishingly small amounts of this released protein, making troponin the most sensitive early indicator of cardiac cell death available.
What Cardiac Troponin Is and Why It Is Specific to the Heart
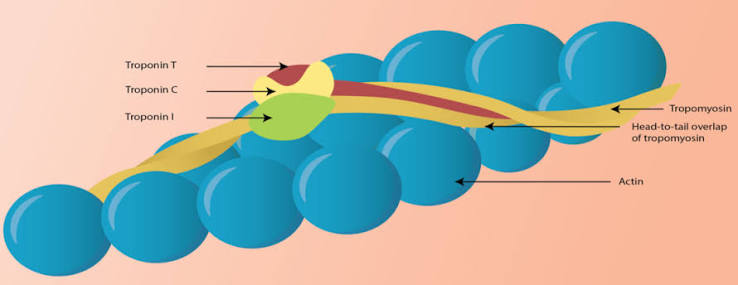
Troponin is part of the protein complex that regulates muscle contraction in all striated muscle ??? both skeletal (voluntary) muscle and cardiac muscle. The troponin complex consists of three subunits: troponin C (binds calcium, triggering contraction), troponin I (inhibits muscle contraction when calcium is absent), and troponin T (anchors the complex to tropomyosin on the actin filament). The cardiac isoforms of troponin I (cTnI) and troponin T (cTnT) have amino acid sequences that differ sufficiently from the skeletal muscle isoforms that highly specific antibody-based assays can distinguish cardiac troponin from skeletal muscle troponin.
This cardiac specificity is what makes the troponin test so valuable: elevated skeletal muscle damage from strenuous exercise, trauma, or rhabdomyolysis raises creatine kinase (CK) but does not raise cardiac-specific troponin above the 99th percentile reference limit in most cases. A positive cardiac troponin test therefore specifically indicates cardiac muscle cell damage ??? not general muscle damage from non-cardiac causes. This specificity is why troponin has replaced creatine kinase-MB (CK-MB) as the primary biomarker for MI diagnosis: CK-MB is also found in skeletal muscle and can be elevated by musculoskeletal injuries, while cardiac-specific troponin assays are highly selective for cardiac injury.
How the Troponin Test Is Used in the Emergency Department
When a patient arrives at the emergency department with chest pain, the troponin test is one of the first blood tests drawn ??? along with an ECG (electrocardiogram), which provides immediate electrical evidence of ST elevation suggesting complete coronary occlusion (STEMI). The troponin test addresses the second major question: is there biochemical evidence of cardiac cell death that confirms an NSTEMI (non-ST elevation myocardial infarction)?
The validated approach for troponin interpretation in chest pain assessment follows the European Society of Cardiology (ESC) 0h/1h or 0h/2h rapid rule-out/rule-in algorithm: blood is drawn at presentation (0 hours) and again at 1 hour (or 2 hours). If both values are below very low thresholds AND the absolute change between the two draws (the “delta troponin”) is below a small cutoff ??? the acute MI is effectively ruled out with a negative predictive value exceeding 99 percent. This protocol allows safe early discharge of the majority of chest pain patients who do not have an MI, dramatically reducing unnecessary hospital admissions while maintaining patient safety.
Patients whose 0-hour troponin is very high, or whose 1-hour delta change is very large, are “ruled in” ??? the pattern is highly predictive of acute MI, and cardiology consultation, further imaging, and consideration of cardiac catheterization follow. Patients in the “observe zone” ??? neither definitively ruling out nor ruling in at 1 hour ??? require a third draw at 2 to 3 hours for final classification. High-sensitivity troponin assays (hsTnI or hsTnT) enable this rapid protocol; older conventional assays could not detect troponin changes over 1 hour reliably.
Non-Cardiac Causes of Elevated Troponin ??? What Else Raises It
One of the most important concepts in troponin interpretation is that a positive troponin test does not exclusively mean a heart attack. Cardiac troponin is elevated by any process that causes cardiomyocyte injury or death ??? including conditions entirely outside the coronary arteries:
- Pulmonary embolism (PE): A large pulmonary embolism causes acute right ventricular pressure overload ??? the RV is suddenly forced to pump against a blocked pulmonary circulation. This RV strain causes wall stress and microinfarction of the RV free wall, releasing troponin. Troponin elevation in PE predicts hemodynamic instability and early mortality ??? it is used to classify PE severity and guide decisions about thrombolysis vs. anticoagulation alone.
- Myocarditis: Inflammation of the heart muscle from viral infection (most commonly), autoimmune disease, or drug toxicity (checkpoint inhibitor immunotherapy, anthracycline chemotherapy) directly damages cardiomyocytes and releases troponin. The distinguishing features from MI: typically younger patients, preceding viral illness, chest pain in a non-coronary distribution, ECG changes that don’t follow a coronary territory, and cardiac MRI showing epicardial or mid-wall LGE rather than subendocardial LGE.
- Chronic kidney disease (CKD): Patients with advanced CKD have chronically elevated troponin ??? primarily hsTnT ??? due to impaired troponin clearance and low-grade uremia-induced myocardial injury. The critical distinguishing feature: CKD-related troponin elevation is stable across serial measurements (no significant delta). When a CKD patient presents with chest pain and an elevated troponin, clinicians must assess the delta (is it rising from the patient’s elevated CKD baseline?) rather than comparing the absolute value to the general population URL.
- Sepsis and critical illness: Systemic inflammatory response and hemodynamic instability in sepsis cause direct myocardial depression through cytokine effects, coronary microvascular thrombosis, and relative ischemia ??? troponin elevation in ICU patients is common and predicts mortality independently of the primary diagnosis.
- Takotsubo (stress) cardiomyopathy: After extreme emotional or physical stress, a massive sympathetic surge causes reversible apical LV ballooning mimicking anterior MI ??? with troponin elevation, ST changes, and chest pain. Distinguished from anterior STEMI by coronary angiography showing no culprit coronary occlusion, and by the characteristic apical ballooning on echo or ventriculography in a non-coronary distribution.
- Type 2 MI (supply-demand mismatch): MI without plaque rupture ??? troponin elevation from myocardial ischemia due to severe tachycardia, hypertension crisis, anemia, or hypotension in a patient with pre-existing CAD. Treatment is directed at the precipitating cause (rate control, blood pressure management, transfusion) rather than the coronary intervention used for type 1 MI.
Troponin Results After a Heart Attack ??? What to Expect During Recovery
For patients who have been diagnosed with an acute MI and are asking what to expect from troponin levels during their hospital stay and recovery:
Troponin rises continuously in the first 12 to 24 hours after an MI, reaching a peak that roughly corresponds to the amount of heart muscle damaged. Larger heart attacks (complete proximal coronary artery occlusion, large territory at risk) produce higher peak troponin values than small heart attacks (partial occlusion, small territory). After the peak, troponin falls gradually ??? cTnI typically normalizes within 5 to 7 days, while cTnT may remain detectably elevated for 10 to 14 days in large MIs because of its slower release from damaged cells and longer plasma half-life.
Hospitals perform serial troponin measurements (typically at admission, 3 to 6 hours, and 12 to 24 hours) not only to confirm the diagnosis but to track the peak (infarct sizing) and verify the falling pattern (confirming the acute event has stabilized rather than ongoing ongoing injury from incomplete reperfusion). After discharge, troponin is not routinely re-measured unless new symptoms develop ??? a single elevated discharge troponin in a patient who has been treated and is stable does not indicate a new event and should not prompt alarm.
See our related articles on blood tests for heart health, common heart tests explained, what is an electrocardiogram, heart failure symptoms and monitoring, and major risk factors for heart disease. The American Heart Association heart attack diagnosis guide, NHLBI heart attack diagnosis page, and ESC NSTEMI guidelines provide authoritative clinical standards for troponin use.
- Thygesen K, et al. Fourth Universal Definition of Myocardial Infarction. J Am Coll Cardiol. 2018;72(18):2231-2264.
- Collet JP, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289-1367.
- Mueller C, et al. ESC 0h/1h-algorithm using high-sensitivity cardiac troponin T for the diagnosis of NSTEMI. Eur Heart J. 2019;40(7):605-614.
- Apple FS, et al. High-Sensitivity Cardiac Troponin Assays: Practice Recommendations from the AACC. Clin Chem. 2022;68(11):1496-1506.
- Konstantinides SV, et al. 2019 ESC Guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2020;41(4):543-603.
Understanding Your Troponin Number ??? What the Values Actually Mean
One of the most confusing aspects of the troponin test for patients and families is interpreting what a specific number means ??? especially since different hospitals use different assay brands with different units and different thresholds. Here is a practical framework for understanding troponin results without getting lost in the numbers:
The 99th percentile upper reference limit (URL) is the critical threshold: Each laboratory establishes a “99th percentile URL” ??? the troponin concentration exceeded by only 1 percent of healthy adults without cardiac disease. Any value above this threshold is considered elevated. The URL varies by assay and manufacturer: for the widely used Roche Elecsys hsTnT assay, the URL is 19 ng/L; for Abbott ARCHITECT hsTnI, it is 26 ng/L; for Siemens ADVIA Centaur hsTnI, it is 45 ng/L. The specific number that matters at your hospital depends on which assay they use ??? ask your nurse or doctor which assay is in use if you want to interpret your specific number.
How far above the URL matters: A troponin 1.5 times above the URL (mild elevation) has very different implications than a troponin 10 times above the URL. Very high elevations ??? especially when combined with a large absolute delta (change from the first draw to the second draw) ??? are strongly associated with large myocardial infarctions requiring urgent intervention. Mild elevations without significant delta may indicate chronic stable myocardial stress from heart failure or kidney disease rather than an acute MI.
The delta is often more informative than the absolute value: The absolute change between serial troponin draws ??? called the delta ??? is what distinguishes acute injury from chronic stable elevation. The ESC-validated 0h/1h algorithm uses specific delta thresholds in absolute units (not percentages) because high-sensitivity assays are more reproducible in absolute change than percentage change at low concentrations. However, as a general rule, a change of more than 20 to 30 percent from the baseline value at 1 to 2 hours is considered a significant delta indicating acute MI. A troponin that is mildly elevated but completely stable (less than 5 percent change) over 3 to 6 hours points toward a chronic, non-acute cause.
Sex Differences in Troponin ??? Why Women Are Sometimes Underdiagnosed
An important and clinically consequential finding in cardiovascular medicine is that women and men have different baseline troponin levels ??? and that using a single sex-neutral troponin threshold may lead to underdiagnosis of MI in women. Understanding this disparity helps patients advocate for appropriate testing:
Women have lower baseline troponin levels than men, likely because women have smaller heart muscle mass (the amount of cardiomyocyte protein, including troponin, released at rest is proportional to total muscle mass). The 99th percentile URL for hsTnI is approximately 16 to 20 ng/L in healthy women versus 30 to 53 ng/L in healthy men for most assay brands ??? a substantial difference. When hospitals use a single sex-neutral threshold (often derived predominantly from male reference populations), a woman with a troponin of 20 ng/L may be below the hospital’s URL and classified as “negative” even though her troponin is above the female-specific 99th percentile ??? missing an NSTEMI.
The ESC 2020 NSTEMI guidelines recommend using sex-specific troponin thresholds in the 0h/1h rapid rule-out/rule-in algorithm. Studies using sex-specific cutoffs have demonstrated that approximately 20 percent of women diagnosed with “unstable angina” (no troponin elevation) under sex-neutral thresholds would be correctly reclassified as NSTEMI under sex-specific thresholds ??? improving their access to guideline-directed early invasive treatment. If you are a woman being evaluated for chest pain and your troponin is reported as “normal” at a level close to the threshold, it is reasonable to ask whether sex-specific troponin thresholds were applied.
Troponin and Long-Term Cardiovascular Risk ??? The Population Perspective
Beyond its role in acute MI diagnosis, cardiac troponin measured in outpatient settings ??? even at low concentrations using high-sensitivity assays ??? predicts long-term cardiovascular events and mortality in the general population. This finding has opened the door to using hsTn as a chronic cardiovascular risk marker, not just an acute biomarker:
Large population studies (the Atherosclerosis Risk in Communities study, the Cardiovascular Health Study, the Heart and Soul Study) have demonstrated that hsTnT or hsTnI concentrations ??? even within the “normal” range below the 99th percentile URL ??? predict future MI, heart failure hospitalization, and cardiovascular death over 5 to 10 years of follow-up. The relationship is continuous (higher troponin within the normal range = higher event risk) and independent of traditional risk factors including LDL cholesterol, blood pressure, diabetes, and smoking.
The biological interpretation is that low-level circulating troponin in stable outpatients reflects subclinical myocardial injury ??? the ongoing, low-grade cardiomyocyte turnover and stress that accompanies hypertensive heart disease, early heart failure, subclinical coronary artery disease, and aging-related myocardial fibrosis. A patient with hsTnT of 15 ng/L (below the 19 ng/L URL) has a measurably higher 10-year cardiovascular event rate than a patient with hsTnT of 3 ng/L ??? even though both are technically “normal.” This population-level insight has not yet translated into routine clinical recommendations for outpatient troponin screening of asymptomatic adults (the appropriate response to a mildly elevated troponin in an asymptomatic person is unclear ??? further research is needed before this becomes clinical practice).
Troponin in Specific Conditions ??? A Practical Reference
Several common scenarios warrant knowing specifically how troponin behaves and how to interpret results:
After strenuous exercise: Vigorous prolonged exercise (marathon running, intense endurance training) causes transient troponin elevation in healthy athletes ??? typically 2 to 5 times the URL, peaking 1 to 3 hours after exercise and normalizing within 24 hours. This “exercise-induced troponin release” does not indicate myocardial damage or cardiovascular disease in the absence of symptoms ??? it likely reflects reversible cardiomyocyte membrane permeability change from high wall stress during sustained exercise. An asymptomatic runner whose troponin is drawn shortly after a marathon and found elevated should not be treated as an MI ??? clinical context (no chest pain, no ECG changes, troponin normalizes within 24 hours) distinguishes exercise physiology from pathology.
After electrical cardioversion or defibrillation: External defibrillation and synchronized cardioversion cause troponin release proportional to the energy delivered. A troponin drawn within 4 to 6 hours of electrical cardioversion will often be elevated ??? this reflects myocardial cell membrane disruption from the current, not an MI. The clinical significance: post-cardioversion troponin elevation should not trigger an unnecessary coronary angiography unless accompanied by new ECG changes, symptoms, or hemodynamic instability suggesting a true ischemic event.
In cardiac contusion (chest trauma): Blunt chest trauma (motor vehicle accident, fall, direct blow) can cause myocardial contusion ??? bruising of the heart muscle ??? with troponin elevation, ECG changes, and occasionally arrhythmias. Troponin is measured in trauma patients with significant chest injury to detect cardiac contusion. Unlike MI, cardiac contusion does not result in coronary artery occlusion ??? coronary angiography is not indicated unless a distinct ischemic pattern suggests a coincidental acute coronary syndrome.
During chemotherapy (cardiotoxicity monitoring): Anthracycline chemotherapy (doxorubicin, epirubicin) and HER2-targeted agents (trastuzumab, pertuzumab) cause cardiomyocyte injury that may manifest as troponin elevation before echocardiographic LV function decline becomes apparent. Troponin-based cardiotoxicity monitoring during cancer treatment identifies patients who may benefit from early cardioprotective intervention (ACE inhibitor, beta-blocker) to prevent irreversible cardiomyopathy. Oncologists and cardiologists may measure troponin at baseline, during, and after high-risk chemotherapy regimens ??? ask your oncology team whether troponin monitoring is planned as part of your treatment protocol.
Questions to Ask Your Doctor About a Troponin Result
If you receive a troponin result ??? whether in an emergency setting or as part of a follow-up ??? here are the questions that help clarify what the result means in your specific situation:
- “Is this value above or below the 99th percentile upper reference limit for your lab?” ??? This tells you whether the result is “elevated” by the hospital’s specific assay threshold, rather than relying on a general number from the internet.
- “Was this a single draw or were serial measurements done?” ??? A single elevated troponin alone is not sufficient to diagnose acute MI. Serial measurements and the delta pattern are required per international guidelines.
- “Are you using sex-specific cutoffs?” ??? Particularly relevant for women, where sex-neutral thresholds may underestimate MI risk.
- “If my troponin is elevated but stable (no delta), what are the likely explanations given my medical history?” ??? This opens the conversation about non-MI causes (CKD, heart failure, pulmonary embolism) versus acute MI, and helps you understand the clinical reasoning.
- “What is the next step based on this result?” ??? Whether it is early discharge (ruled out), observation and repeat testing, or urgent cardiology consultation, understanding the clinical pathway based on your troponin result reduces anxiety and helps you prepare for what comes next.