Diabetes and Stroke Risk: What You Need to Know
Diabetes and stroke risk are connected by one of the most clinically significant metabolic relationships in vascular medicine. Diabetes — both Type 1 and Type 2 — increases ischemic stroke risk by approximately 2 to 4-fold compared to non-diabetic individuals, and this elevated risk persists even after adjusting for the other cardiovascular risk factors that commonly accompany diabetes (hypertension, dyslipidemia, obesity). In population terms, diabetes is responsible for approximately 8 to 12 percent of all strokes globally, and the proportion is increasing as diabetes prevalence continues to rise — from approximately 422 million adults in 2014 to an estimated 643 million by 2030 according to WHO projections.
Beyond the increased incidence of stroke, diabetes substantially worsens stroke outcomes. Diabetic patients who experience ischemic stroke have larger infarct volumes (partly because hyperglycemia in the acute setting worsens ischemic brain injury through multiple mechanisms), lower rates of favorable functional recovery at 90 days, higher rates of post-stroke dementia and cognitive decline, and higher 30-day and 1-year mortality than non-diabetic stroke patients matched for stroke severity. This double burden — more strokes and worse outcomes from each stroke — makes diabetes one of the highest-impact modifiable risk factors for stroke prevention and recovery.
How Diabetes Damages Cerebral Blood Vessels
Diabetes drives cerebrovascular disease through multiple simultaneous mechanisms, each targeting different segments of the vascular tree and different aspects of stroke pathophysiology:
Endothelial dysfunction is one of the earliest and most fundamental vascular consequences of diabetes. Hyperglycemia impairs endothelial nitric oxide synthase (eNOS) — the enzyme that produces nitric oxide (NO), the primary vasodilatory and anti-thrombotic signal in the arterial endothelium. Reduced NO availability leads to impaired vasodilation, increased platelet adhesion and aggregation, upregulation of adhesion molecules (VCAM-1, ICAM-1) that recruit inflammatory cells to the vessel wall, and increased endothelial permeability — collectively creating a pro-atherosclerotic and pro-thrombotic endothelial state. Endothelial dysfunction in diabetes is measurable before clinical vascular disease develops, explaining why diabetic patients accumulate atherosclerotic burden faster than non-diabetic individuals at comparable traditional risk factor levels.
Advanced glycation end-products (AGEs) accumulate in diabetes as glucose non-enzymatically reacts with proteins and lipids over time. AGEs cross-link collagen in vessel walls, increasing arterial stiffness (reducing the compliance buffer that normally dampens pulse pressure), impairing nitric oxide signaling, and activating RAGE (receptor for advanced glycation end-products) — a multiligand receptor that drives NF-κB-mediated inflammatory gene expression in endothelial cells, smooth muscle cells, and macrophages. The arterial stiffness produced by AGE accumulation is particularly relevant for cerebrovascular disease because stiff arteries transmit more of the cardiac pulse pressure to the cerebral microcirculation, which normally operates at much lower pressures than the systemic circulation and is more vulnerable to pulsatile injury.
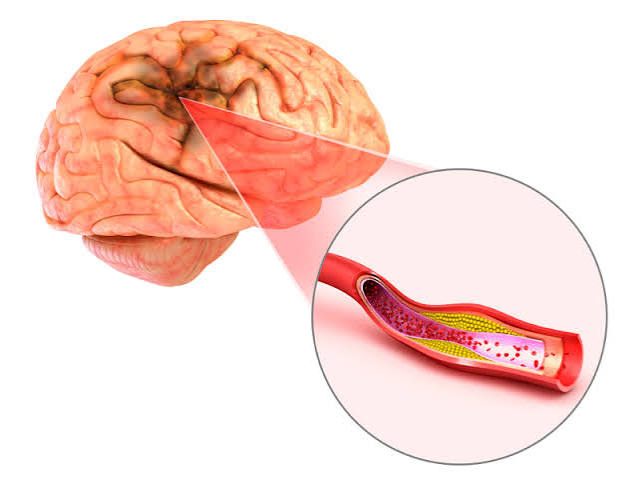
Accelerated large vessel atherosclerosis: Diabetes accelerates the formation and progression of atherosclerotic plaque in the carotid arteries, intracranial arteries, and aortic arch — the large vessel sources of ischemic stroke from artery-to-artery embolism and in situ thrombosis. Multiple mechanisms contribute: LDL glycation (glycated LDL is more readily oxidized and taken up by macrophage scavenger receptors than native LDL), insulin resistance (the hyperinsulinemia of early Type 2 diabetes directly promotes smooth muscle cell proliferation and lipid accumulation in the arterial wall), and the chronic inflammatory state of diabetes that destabilizes existing atherosclerotic plaques.
Small vessel disease (diabetic cerebral microangiopathy): In addition to large artery disease, diabetes causes structural damage to the small perforating arteries that supply deep brain structures — the same vessels affected by hypertensive lipohyalinosis. Diabetic microangiopathy in the brain causes lacunar infarcts and white matter hyperintensities (detectable on brain MRI as areas of increased T2 signal in the periventricular and subcortical white matter), which impair cognitive function, increase fall risk, and predispose to lacunar stroke. Diabetes and hypertension have synergistic effects on cerebral small vessel disease — patients with both conditions have far more extensive white matter disease than patients with either condition alone.
Promotion of atrial fibrillation: Diabetes promotes AF through cardiac autonomic neuropathy (which impairs the autonomic regulation of heart rate and rhythm), structural cardiac remodeling (left ventricular hypertrophy and diastolic dysfunction driven by hypertension and hyperglycemia-induced fibrosis), and systemic inflammation. AF in diabetic patients carries a higher cardioembolic stroke risk than AF in non-diabetic patients because diabetes is itself a component of the CHA₂DS₂-VASc score, contributing an additional point to the stroke risk calculation.
Hyperglycemia During Stroke — Acute Worsening of Infarct
An important and underappreciated dimension of the diabetes-stroke relationship is the acute effect of elevated blood glucose at the time of stroke on brain injury severity. Multiple lines of evidence demonstrate that hyperglycemia in the hours following ischemic stroke significantly worsens outcome — even in patients without pre-existing diabetes who develop stress hyperglycemia from the physiological response to acute illness.
The mechanisms by which acute hyperglycemia worsens ischemic brain injury include: increased production of lactic acid through anaerobic glycolysis in ischemic but still-viable penumbra neurons (worsening intracellular acidosis, which is directly toxic to neurons); increased generation of reactive oxygen species from glucose metabolism; impaired microvascular reperfusion through blood-brain barrier disruption (high glucose increases endothelial permeability, worsening cerebral edema and hemorrhagic transformation risk); and impaired collateral blood flow (hyperglycemia reduces NO-mediated vasodilation in collateral vessels that maintain penumbra viability).
Clinical trials of intensive insulin therapy to correct hyperglycemia in acute stroke have generally not shown the dramatic outcome improvements predicted by the mechanisms above — reflecting the difficulty of translating pathophysiological reasoning to clinical benefit and the risk of hypoglycemia from aggressive insulin therapy (hypoglycemia is also severely harmful to ischemic neurons). Current guidelines recommend avoiding marked hyperglycemia (glucose above 180 mg/dL) in the acute stroke period and avoiding hypoglycemia (below 60 mg/dL), with insulin therapy initiated for persistent glucose above 180 mg/dL.
Stroke Prevention in Diabetes — Evidence-Based Treatment Priorities
The evidence base for stroke prevention in diabetic patients identifies several interventions with strong, quantified benefit:
Blood pressure control is the single most impactful intervention for stroke prevention in diabetic patients. The UKPDS (UK Prospective Diabetes Study) demonstrated that tight blood pressure control (mean achieved BP 144/82 mmHg versus 154/87 mmHg in the control group) reduced stroke by 44 percent in Type 2 diabetes — the largest single risk factor modification effect in the entire UKPDS. The ACCORD BP trial showed further benefit from intensive BP targets (below 120 mmHg systolic) specifically for stroke in diabetic patients, even though the primary cardiovascular composite endpoint was not significantly reduced. Current guidelines target blood pressure below 130/80 mmHg in diabetic patients, with ACE inhibitors or ARBs as preferred agents (providing both BP reduction and nephroprotective benefit).
Statin therapy: High-intensity statin therapy is recommended for all diabetic patients with established cardiovascular disease or chronic kidney disease and for diabetic patients aged 40 to 75 with LDL above 70 mg/dL or additional cardiovascular risk factors — regardless of baseline LDL level. The CARDS trial (Collaborative Atorvastatin Diabetes Study) demonstrated that atorvastatin 10 mg versus placebo in Type 2 diabetic patients without prior CVD reduced stroke by 48 percent over 4 years. The benefit of statins in diabetes extends beyond LDL reduction to anti-inflammatory, plaque-stabilizing, and endothelial-function-improving pleiotropic effects.
GLP-1 receptor agonists: Liraglutide (LEADER trial), semaglutide (SUSTAIN-6 trial), and albiglutide (Harmony Outcomes trial) have all demonstrated significant cardiovascular event reduction in Type 2 diabetic patients with established CVD or high cardiovascular risk — including significant stroke reduction for semaglutide (39 percent relative reduction in SUSTAIN-6). GLP-1 RAs reduce stroke risk through multiple mechanisms including blood pressure reduction, weight loss, improved endothelial function, anti-inflammatory effects, and plaque stabilization beyond their primary glycemic effect. Current guidelines recommend GLP-1 RAs for Type 2 diabetic patients with established cardiovascular disease (or high CV risk) who need additional glucose control or weight management beyond metformin.
SGLT2 inhibitors: Sodium-glucose cotransporter-2 inhibitors (empagliflozin, canagliflozin, dapagliflozin) reduce cardiovascular death and heart failure hospitalization in diabetic patients with established CVD, primarily through hemodynamic mechanisms (reducing preload and afterload through osmotic diuresis). The evidence for stroke reduction specifically is less consistent across the SGLT2 inhibitor trials than the heart failure benefit — the EMPA-REG OUTCOME trial showed a non-significant 6 percent reduction in stroke, while CANVAS showed a non-significant 10 percent increase. SGLT2 inhibitors are strongly indicated for diabetic patients with heart failure or chronic kidney disease regardless of the stroke outcome data.
Glycemic control: The effect of tight glycemic control on macrovascular outcomes (stroke, MI, cardiovascular death) in diabetes is more modest and controversial than its effect on microvascular outcomes (retinopathy, nephropathy, neuropathy). The ACCORD trial showed that intensive glycemic control (HbA1c target below 6 percent) increased mortality compared to standard control (below 7 to 7.9 percent), likely from increased hypoglycemia, and did not reduce stroke significantly. Current recommendations target HbA1c below 7 percent for most patients, with individualized targets based on age, hypoglycemia risk, comorbidities, and patient preference — with the primary glycemic target being avoidance of marked hyperglycemia and hypoglycemia rather than achieving the lowest possible HbA1c.
The American Stroke Association diabetes and stroke resource explains how diabetes raises stroke risk and what prevention strategies are most effective. The CDC diabetes and heart health page covers the cardiovascular complications of diabetes and their prevention. The NHLBI stroke risk factors page reviews diabetes alongside other major stroke risk factors and prevention approaches.
Related reading: High Blood Pressure and Stroke | Cholesterol and Stroke Risk | What Is a Stroke? | Atrial Fibrillation | Ischemic vs Hemorrhagic Stroke
Sources
- Emerging Risk Factors Collaboration. Diabetes Mellitus, Fasting Glucose, and Risk of Cause-Specific Death. N Engl J Med. 2011;364(9):829-841.
- UKPDS Group. Tight Blood Pressure Control and Risk of Macrovascular and Microvascular Complications in Type 2 Diabetes (UKPDS 38). BMJ. 1998;317(7160):703-713.
- Marso SP, et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes (SUSTAIN-6). N Engl J Med. 2016;375(19):1834-1844.
- Colhoun HM, et al. Primary Prevention of Cardiovascular Disease with Atorvastatin in Type 2 Diabetes (CARDS). Lancet. 2004;364(9435):685-696.
- Capes SE, et al. Stress Hyperglycaemia and Prognosis of Stroke in Nondiabetic and Diabetic Patients. Stroke. 2001;32(10):2426-2432.
Prediabetes and Stroke Risk — The Continuum Begins Before Diagnosis
The cerebrovascular risk associated with impaired glucose metabolism does not begin abruptly at the diagnostic threshold for diabetes — it follows a continuous relationship that starts in the prediabetes range (fasting glucose 100 to 125 mg/dL, or HbA1c 5.7 to 6.4 percent) and increases progressively with worsening glycemic control. Large prospective cohort studies including the Whitehall II study and the ARIC (Atherosclerosis Risk in Communities) study have demonstrated that individuals with prediabetes have 5 to 25 percent higher stroke risk than individuals with normal fasting glucose — a gradient that reflects the cumulative vascular effects of even modestly elevated glucose over time.
The implications for stroke prevention are important: waiting for formal diabetes diagnosis before initiating intensive risk factor management misses years of accumulating vascular damage. Adults with prediabetes who also have hypertension, dyslipidemia, or obesity are particularly high-risk — the cardiovascular risk factors cluster together in metabolic syndrome, and stroke risk in metabolic syndrome is higher than additive from the individual components. The American Diabetes Association recommends annual screening for diabetes in individuals with prediabetes and any additional risk factor, with intensive lifestyle modification (the Diabetes Prevention Program showed 58 percent reduction in diabetes progression with lifestyle intervention) as the primary intervention to reduce both diabetes development and its vascular consequences.
Stroke Recovery in Diabetic Patients — Special Challenges
Diabetic patients who survive ischemic stroke face a more challenging recovery course than non-diabetic patients for reasons that extend beyond the larger initial infarct volumes described above:
Impaired neuroplasticity: The cellular and synaptic mechanisms underlying stroke recovery — neuroplasticity, the reorganization of surviving brain circuits to compensate for damaged ones — appear to be impaired in the diabetic brain. Hyperglycemia reduces BDNF (brain-derived neurotrophic factor) expression, impairs LTP (long-term potentiation, the cellular correlate of learning and motor recovery), and reduces angiogenesis in the peri-infarct zone. Animal studies consistently show smaller infarct volumes but inferior recovery in diabetic compared to non-diabetic stroke models after ischemia of equivalent severity, and clinical studies confirm this pattern.
Increased post-stroke dementia risk: Pre-existing white matter disease from diabetic cerebral microangiopathy — the diffuse small vessel damage that precedes clinically apparent stroke — creates a vulnerable cognitive substrate. A single stroke that causes only mild functional deficits in a non-diabetic patient may unmask significant cognitive impairment in a diabetic patient with pre-existing white matter disease and subclinical cognitive reserve depletion. Post-stroke cognitive impairment is 2 to 3 times more common in diabetic than non-diabetic stroke survivors and is more likely to progress to dementia over the subsequent years.
Increased recurrent stroke risk: Diabetic stroke survivors have significantly higher rates of recurrent stroke than non-diabetic survivors despite similar secondary prevention treatment — reflecting the accelerated vascular disease progression in diabetes. The 5-year recurrent stroke rate in diabetic patients is approximately 30 to 40 percent higher than in matched non-diabetic patients on equivalent antiplatelet, statin, and antihypertensive therapy. This heightened residual risk underscores the importance of optimal secondary prevention — achieving blood pressure below 130/80 mmHg, LDL below 70 mg/dL, adding GLP-1 RA or SGLT2 inhibitor for those with established CVD — and frequent monitoring for new vascular events.
Wound healing and infection risk: Diabetic patients who require hospitalization for stroke and subsequent inpatient rehabilitation face higher rates of urinary tract infection (particularly if bladder dysfunction from stroke occurs), pneumonia (from aspiration or impaired immune response), and pressure ulcers (from impaired peripheral perfusion and reduced sensory awareness in those with peripheral neuropathy). These medical complications prolong hospitalization, interrupt rehabilitation, and independently worsen functional outcomes independent of the stroke itself.
Practical Steps for Diabetic Patients Concerned About Stroke Risk
For adults living with diabetes who want to actively reduce their stroke risk, the evidence supports a structured approach prioritizing interventions with the strongest impact:
The single most impactful step is achieving blood pressure below 130/80 mmHg consistently — not just at physician office visits (where white-coat effect can produce artificially favorable readings) but across the full 24-hour period including morning surge hours. Home blood pressure monitoring with a validated upper arm cuff, with morning readings taken before medication and recorded to share with the treating physician, provides the most accurate picture of blood pressure control and guides medication dose adjustments between office visits.
Ask your physician about statin therapy if you are not already taking one. All adults with Type 2 diabetes who are aged 40 to 75 with LDL above 70 mg/dL are candidates for statin therapy by 2018 ACC/AHA guidelines — the absolute risk reduction from statins in diabetic patients is substantial because their baseline cardiovascular risk is elevated. If you are already on a statin and your LDL is above 70 mg/dL, discuss intensification to high-intensity statin or adding ezetimibe.
If you have established cardiovascular disease (prior heart attack, stroke, or peripheral arterial disease) or are at high cardiovascular risk, ask about GLP-1 receptor agonists — liraglutide or semaglutide have demonstrated stroke reduction in clinical trials and are indicated in this setting. The cardiovascular benefit of these medications is now established independently of their blood glucose-lowering effect, making them appropriate for patients even when glycemic control is relatively satisfactory.
Know the FAST stroke symptoms — Face drooping, Arm weakness, Speech difficulty, Time to call 911 — and act on them immediately if they occur. Diabetic patients are at higher risk of silent stroke (small infarcts without obvious clinical symptoms) that only become apparent on MRI, but symptomatic stroke requires the same immediate 911 response as in non-diabetic patients. Do not wait to see if the symptoms resolve — a resolving symptom may be a TIA (transient ischemic attack), which carries up to 10 to 15 percent 90-day stroke risk and requires emergency evaluation even when symptoms clear completely.
Type 1 vs Type 2 Diabetes — Differences in Stroke Risk Profile
Both Type 1 and Type 2 diabetes confer elevated stroke risk, but through partially different pathophysiological profiles and with different magnitudes of relative risk:
Type 1 diabetes (autoimmune insulin deficiency) is associated with a particularly high relative risk of ischemic stroke — some large cohort studies report 3 to 5-fold elevated stroke risk in Type 1 diabetic patients compared to age-matched non-diabetic individuals. The stroke risk in Type 1 diabetes is strongly related to the duration of diabetes and the quality of long-term glycemic control. Because Type 1 diabetes is diagnosed at younger ages and patients live with the disease for decades, the cumulative vascular burden from chronic hyperglycemia and associated risk factors (hypertension developing in midlife, nephropathy-associated dyslipidemia and coagulopathy) creates significant stroke risk even before patients reach the age when stroke is most common. Additionally, hypoglycemia — far more common in insulin-using Type 1 patients than in most Type 2 patients — may itself be a stroke risk factor through catecholamine-mediated cardiac arrhythmia, platelet activation, and inflammatory signaling.
Type 2 diabetes presents a different risk profile. Because Type 2 diabetes occurs predominantly in older adults who already have hypertension, dyslipidemia, and obesity, the relative risk increase attributable specifically to diabetes (2 to 4-fold) is harder to separate from the risk conferred by its metabolic context. However, diabetes independently predicts stroke even in fully adjusted multivariate analyses. The metabolic syndrome — the clustering of central adiposity, insulin resistance, hypertension, dyslipidemia, and proinflammatory state — creates a vascular risk milieu that exceeds the sum of its parts, and Type 2 diabetes represents the severe end of this spectrum. Treatment of Type 2 diabetes in the context of metabolic syndrome requires simultaneously addressing all components rather than focusing exclusively on glycemic control.
Insulin Resistance as a Brain Vulnerability Factor
Insulin resistance — the reduced responsiveness of peripheral tissues to insulin signaling that precedes and accompanies Type 2 diabetes — has effects on the brain that go beyond the vascular mechanisms described above. The brain is not merely a passive victim of vascular injury in diabetes; it is directly affected by impaired insulin signaling in ways that increase stroke risk and worsen recovery.
Insulin receptors are expressed throughout the brain, particularly in the hippocampus (critical for memory) and cortex (critical for executive function). Insulin signaling in the brain regulates synaptic plasticity, neurotrophin production (particularly BDNF), mitochondrial function, and inflammatory responses. Insulin resistance in the brain — which develops in parallel with peripheral insulin resistance and may be even more pronounced in the brain than peripherally in some individuals — reduces BDNF expression, impairs synaptic plasticity, and promotes neuroinflammation through NF-κB activation. These changes reduce the brain’s resilience to ischemic injury and impair the neuroplasticity mechanisms needed for post-stroke recovery.
The relationship between insulin resistance and cognitive decline is now well-established in large cohort studies: insulin-resistant individuals have higher rates of progression to mild cognitive impairment (MCI) and Alzheimer’s disease, and this relationship is partly independent of cerebrovascular disease — suggesting that metabolic dysfunction in the brain itself contributes to neurodegeneration. Post-stroke cognitive impairment in diabetic patients is therefore driven by two converging processes: ischemic injury from the stroke and pre-existing metabolic impairment of neural function from insulin resistance. This dual mechanism explains why relatively modest strokes can cause disproportionate cognitive impairment in diabetic patients with pre-existing metabolic brain vulnerability.
Screening and Prevention in High-Risk Populations
The combination of diabetes and other stroke risk factors creates multiplicatively elevated risk in specific subgroups that warrant particularly aggressive stroke prevention efforts:
Adults with diabetes and hypertension have approximately 6 to 8-fold elevated stroke risk compared to non-diabetic normotensive individuals — a risk that may approach 1 to 2 percent annual stroke risk even without established cardiovascular disease. This group represents the clearest case for early, aggressive, multifactorial risk factor intervention — targeting both blood pressure below 130/80 mmHg and LDL below 70 mg/dL simultaneously provides approximately 50 to 60 percent relative stroke risk reduction compared to usual care.
Adults with diabetes and atrial fibrillation form a very high-risk group in which the interaction between diabetes’s procoagulant state and AF’s stroke mechanism (left atrial appendage thrombus) produces particularly severe cardioembolic strokes. CHA₂DS₂-VASc scoring in diabetic AF patients almost always results in scores of 2 or above (diabetes alone contributes 1 point, plus age and hypertension which are near-universal in diabetic AF patients), making anticoagulation clearly indicated in this group. The choice between DOACs and warfarin in diabetic patients with AF and chronic kidney disease requires careful consideration of renal function, as all DOACs are renally cleared to varying degrees.
Adults with diabetes and prior ischemic stroke or TIA represent the most urgent secondary prevention scenario — 5-year recurrent stroke risk in this group approaches 30 to 40 percent without optimal treatment. The combination of high-intensity statin, blood pressure below 130/80 mmHg, antiplatelet therapy, and GLP-1 RA (in those with established CVD) provides the best available risk reduction, but requires active engagement with medication adherence, regular monitoring, and lifestyle modification to achieve and maintain the intervention targets that translate into reduced stroke incidence.